
Abstract
Patients with bronchiectasis (BE) present exacerbations that increase with severity of the disease. We aimed to determine the annual cost of BE treatment according to its severity, determined by FACED score, as well as the parameters associated with higher costs. Multicentre historical cohorts study with patients from six hospitals in Spain. The costs arising during the course of a year from maintenance treatment, exacerbations, emergency visits and hospital admissions were analysed. In total, 456 patients were included (56.4% mild BE, 26.8% moderate BE and 16.9% severe BE). The mean cost was €4671.9 per patient, which increased significantly with severity. In mild BE, most of the costs were due to bronchodilators and inhaled steroids; in severe BE, most were due to exacerbations and inhaled antibiotics. Forced expiratory volume in 1 second (FEV1%), age, colonization by Pseudomonas aeruginosa and the number of admissions were independently related to higher costs. The highest costs were found in patients with BE associated with chronic obstructive pulmonary disease, with the most exacerbations and with chronic bronchial colonization by Pseudomonas aeruginosa (PA). In conclusion, BE patients gave rise to high annual costs, and these were doubled on each advance in severity on the FACED score. FEV1%, age, colonization by PA and the number of admissions were independently related to higher costs.
Keywords
Introduction
Non-cystic fibrosis bronchiectasis (hereafter BE) is an irreversible dilatation of the bronchi that is associated with infectious exacerbations even in its initial stages. In more advanced stages, patients can experience chronic bronchial colonization (CBC) by potentially pathogenic microorganisms (PPM), which involves more symptoms, short- or long-term treatment with antibiotics and a progressive deterioration of the pulmonary function and quality of life. 1 –3 In common with other airway diseases, the severity of BE cannot be explained by one single variable, such as radiological extension, the CBC or the extent of functional impairment. 4 –6 The FACED score 7 was recently developed to classify patients’ severity with a multidimensional scale, which includes age, degree of dyspnoea, FEV1%, presence of CBC by Pseudomonas aeruginosa (PA) and number of lobes affected.
The few studies published to date on the costs associated with BE show that these are high, 8 –10 and possibly greater than those described for chronic obstructive pulmonary disease (COPD). 11 –14 Since most of the direct costs of the BE management can be attributed to exacerbations and baseline treatment, 15,16 it is reasonable to suppose that more severe patients give rise to higher health costs. This is an important topic, in the light of the current levels of diagnosis, 17,18 hospitalization and mortality 10,19 of BE patients.
These days the incorporation of financial studies into clinical trials is recommended as a means to evaluate the cost-efficiency of new treatments, 20,21 like those being developed for patients with BE. 22 –24 These analyses require prior knowledge of data on the financial impact of BE, such as the annual cost of treatment and the proportion attributable to exacerbations and treatments in a stable phase, as well as the variables that exert the greatest influence on these costs. Given the lack of information in this respect, our objective was to determine, via a representative multicentre study, the annual cost of the treatment of patients with BE according to their severity, (as determined by the FACED score) and the circumstances that are associated with higher costs.
Material and methods
Study design
Multicentre retrospective study of historical cohorts, in which six Spanish hospitals took part. Data were used in accordance with the Data Protection Law 15/1999 and authorization was given by the Ethics Committee for clinical research of the Unió Catalana d’Hospitals (register number 14/45).
Study population
All patients >18 years, monitored in specialized outpatient clinics for BE between January and December 2013, with BE diagnosed by high-resolution computed tomography of the thorax, 25 were included consecutively. Cases with coexisting COPD were monitored in these specialized clinics because the diagnosis of BE preceded that of COPD, or because they were referred from other consulting rooms due to the detection of clinically relevant BE (chronic expectoration, bronchial colonization by PPM, etc.). Patients were excluded if they lacked sufficient data to calculate the FACED score or determine the number of treatments, exacerbations or hospital admissions. Therefore, the collected data thoroughly reflect all the costs arising from baseline treatment and exacerbations.
Variables of the study
The data collected were demographic; related to BE; spirometry in stable phase; microbiology (presence of CBC according to established criteria 26 ); and radiology (location, extension and severity of the BE). The FACED score was calculated to determine severity of BE, dividing patients into mild (0–2 points), moderate (3–4 points) or severe BE (5–7 points). 7 The annual costs analysed were as follows: number of exacerbations, visits to emergency rooms and admissions, series of oral or home intravenous antibiotics, cyclic azithromycin, inhaled antibiotics, inhaled corticosteroids, long-acting beta-agonists (LABA), short- or long-acting anticholinergics, respiratory physiotherapy cycles, home oxygen therapy, home nebulizer and admission to a convalescence centre.
All the data were collected meticulously from the medical records from each hospital, from primary healthcare centres as well as each autonomous community’s electronic prescription program.
Unit prices assignment
The unit prices of drugs were obtained from the Vademecum (Edition 2013). Hospital dispensation drugs prices were obtained from the database of the General Council of Official Pharmacists’ Associations (2013). The cost of each hospital admission was obtained from the statistics website of the Ministry of Health: €3783.61. 27 Other costs (emergency room visit, respiratory physiotherapy, home oxygen therapy, home nebulizers and admission into convalescence centre) were calculated from the mean of the tariffs established in the Official Bulletins of the participating autonomous communities. 28 –31 Table 1 shows the unit prices with respect to non-pharmacological costs. Detailed information on all collected variables is available as a supplementary file.
Unit costs apart from drugs.

Cost of hospital admission: mean price of the hospital stay for bronchiectasis in 2012, according to data from the Statistics Portal of the Ministry of health, Social Services and Equality. 27 All other costs: mean of the tariffs established in the Official Bulletins of the participating autonomous communities. 28 –31
Statistical analysis
SPSS Statistics software, version 21.0 (SPSS, Chicago, Illinois, USA) was used for statistical analysis. Quantitative variables were tabulated as mean and standard deviation, and qualitative variables as absolute numbers and percentages. The Kolmogorov–Smirnov test was used to analyse distribution of variables. The Mann–Whitney test was used to compare quantitative variables between two groups and the Kruskal–Wallis test for those between more than two groups. The χ2 test was used to compare qualitative variables. To evaluate differences in costs between subgroups of patients, we used the student’s t test for independent groups. A multiple regression analysis was used to determine which variables were independently associated with a higher total cost. All variables that presented a significant relationship with cost were included, apart from total FACED score, as its components were already included. The analysis was adjusted for possible confounding factors (gender, body mass index, smoking, Charlson index, number of lobes affected, degree of dyspnoea, number of exacerbations, chronic colonization by different PA microorganisms, age and COPD). A p value <0.05 was considered significant.
Results
Clinical data
In total, 456 patients were included, with a mean age of 67.2 ± 15.5 years (61.2% women). According to the FACED score, 56.4% had mild BE, 26.8% moderate and 16.9% severe. Table 2 shows their demographic characteristics according to their severity group. Greater severity involved more symptoms, a higher score on the Charlson index, CBC and mortality (p < 0.001); 54.8% of the patients presented CBC by PPM 26 (83.4% of those with severe BE (p < 0.001)). The most frequent microorganisms were PA (68%), Haemophilus influenzae (25.6%), Stapylococcus aureus (8.8%) and atypical mycobacteria (8.4%). More than 30 different etiologies of BE were recorded.
Demographic characteristics of the patients.
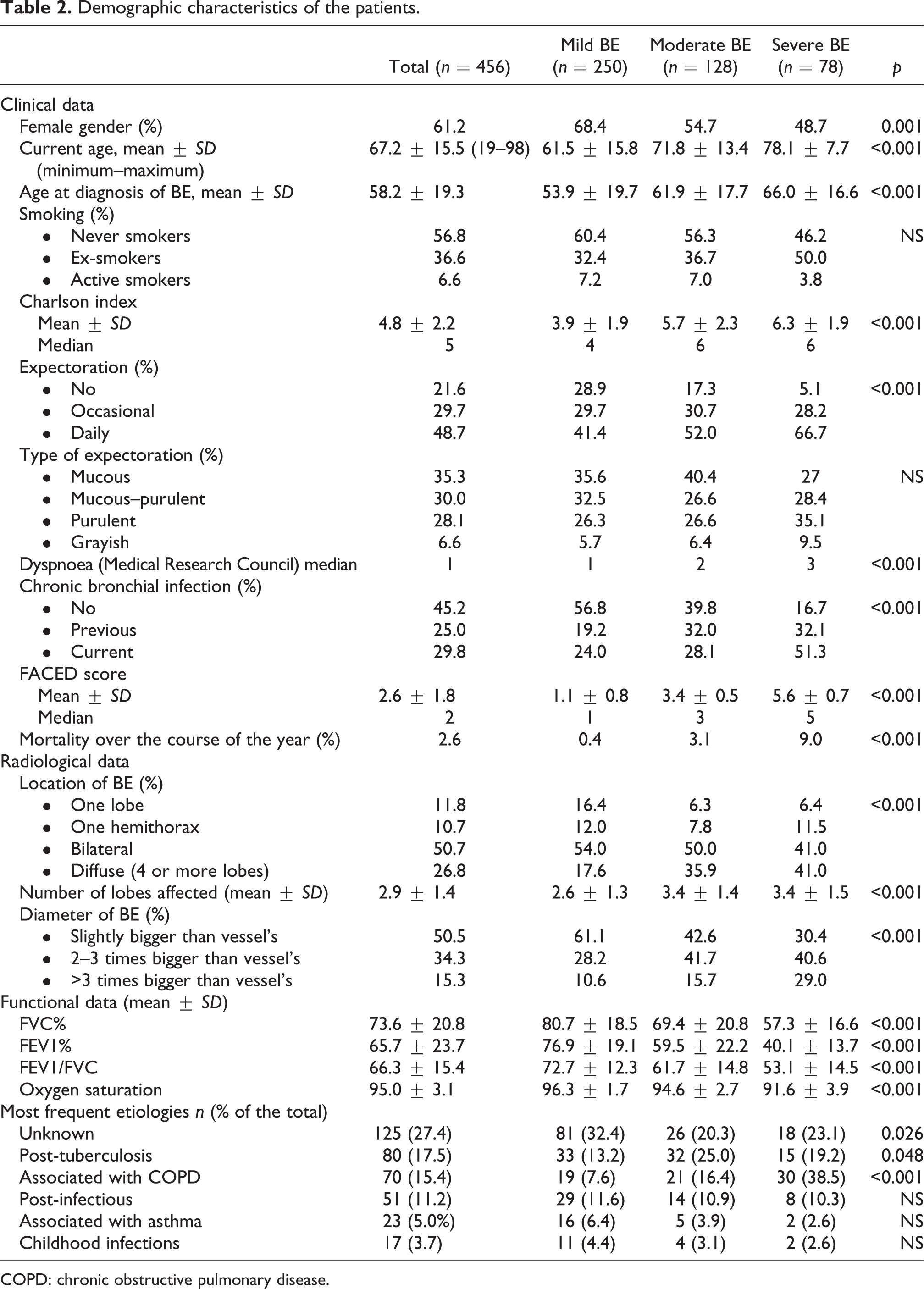
COPD: chronic obstructive pulmonary disease.
Table 3 details the baseline treatments and exacerbations according to the severity of BE. We found that the use of inhalers, oral antibiotics and cyclical azithromycin, inhaled antibiotics, respiratory physiotherapy and home oxygen therapy was greater with greater severity (p < 0.001). In severe BE, the use of inhalers, cyclical azithromycin, inhaled antibiotics and home oxygen therapy were particularly noteworthy. The most severe patients presented a greater number of exacerbations, emergency room visits and hospital admissions (p < 0.001) over the course of the year.
Baseline treatments and exacerbations according to the severity of bronchiectasis.

LABA: Long-acting beta-agonists; ICS: inhaled corticoid.
Cost analysis
The mean annual cost per patient was €4671.9 ± 6281.1, and it increased with severity: €2993.3 in mild BE, €4731.7 in moderate BE and €9998.9 in severe BE (p < 0.001). Total cost increased by €1449.3 ± 143.3 for every point of the FACED score (Figure 1).

Overall costs according to severity of bronchiectasis. Graph A: Overall cost according to the FACED score. Graph B: Total cost according to the severity group: Mild BE (0–2 points), moderate BE (3–4 points) or severe BE (5–7 points). BE: bronchiectasis.
Table 4 shows the various costs according to severity. There was a statistical correlation between severity of BE and the majority of costs. In mild patients, the greatest impact was due to inhalers, whilst in moderate and severe patients it was due to exacerbations (p < 0.001). With respect to the costs for exacerbations, in mild BE these were mainly due to oral antibiotics (74.3%), whilst in severe patients hospital admissions were mostly responsible (55.5%), representing 27.3% of the total cost, as opposed to 6.7% in mild patients.
Costs in total, and according to the severity of bronchiectasis.
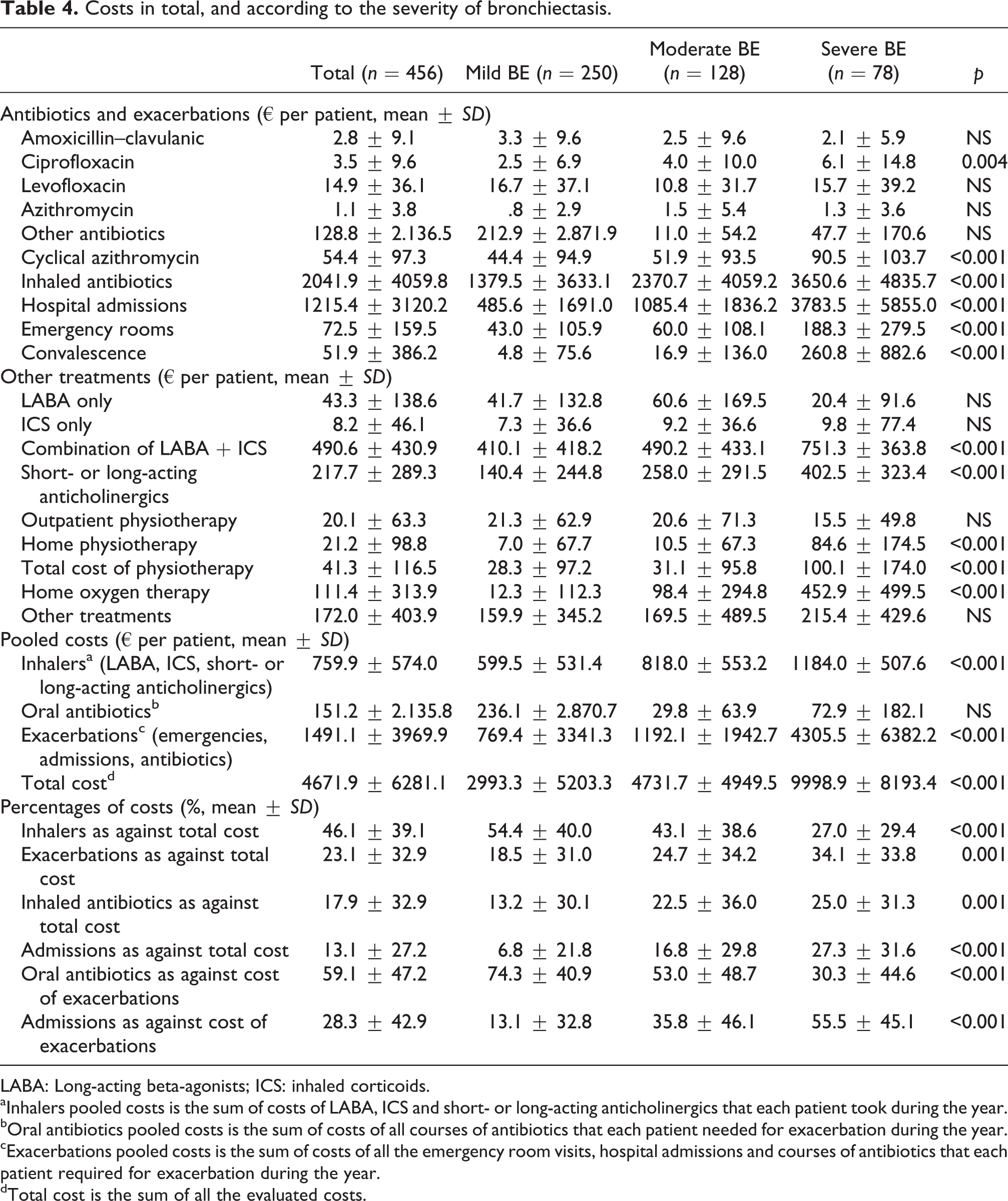
LABA: Long-acting beta-agonists; ICS: inhaled corticoids.
aInhalers pooled costs is the sum of costs of LABA, ICS and short- or long-acting anticholinergics that each patient took during the year.
bOral antibiotics pooled costs is the sum of costs of all courses of antibiotics that each patient needed for exacerbation during the year.
cExacerbations pooled costs is the sum of costs of all the emergency room visits, hospital admissions and courses of antibiotics that each patient required for exacerbation during the year.
dTotal cost is the sum of all the evaluated costs.
Multivariate analysis
The multiple regression analysis showed that FEV1%, age, PA colonization and the number of hospital admissions were the variables independently associated with a higher total cost. These variables explained 55% of the variance in the cost (Table 5).
Multivariate analysis.

Dependent variable: overall cost. CBC by PA: Chronic bronchial infection by PA. CBC: chronic bronchial colonization; PA: Pseudomonas aeruginosa.
aVariance explained by the model: 55%.
bVariance explained by the model: 43.2%.
A second multivariate analysis was performed to further determine the relationship of FACED score, as a sum of variables, with the cost per patient. We included FACED score in the model, without including its component variables. We found that FACED score was indeed associated with a higher total cost, and that in conjunction with the Charlson index and the number of hospital admissions it accounted for 43.2% of the variance (Table 5).
Analysis of subgroups
There were 70 patients with BE associated with COPD, which presented a mean cost similar to that of the severe BE (€7448.5 ± 7934.6) and higher than that of patients without COPD. Their highest economic impact was attributable to exacerbations, particularly admissions (Table 6). Distribution of COPD severity according to global initiative for chronic obstructive lung disease (GOLD) stage was: I (10%), II (35.7%), III (31.4%), and IV (22.9%). Costs also increased with COPD severity. Interestingly, GOLD IV patients were more expensive mainly due to inhaled antibiotic, whilst those with GOLD III were more expensive due to exacerbations.
Costs in patients with COPD and in patients with exacerbations.

LABA: long-acting beta-agonists; ICS: inhaled corticoids.
aInhalers pooled costs is the sum of costs of LABA, ICS and short- or long-acting anticholinergics that each patient took during the year.
bOral antibiotics pooled costs is the sum of costs of all courses of antibiotics that each patient needed for exacerbation during the year.
cExacerbations pooled costs is the sum of costs of all the emergency room visits, hospital admissions and courses of antibiotics that each patient required for exacerbation during the year.
dTotal cost is the sum of all the evaluated costs.
Ninety-eight patients (21.5%) presented more than two exacerbations during the year (Table 6). Total cost of this subgroup was €737,009, a 34.5% of the overall outlay of the 456 patients included (€2,130,416.6). Even more significant were the 26 patients (5.7%) who required two or more hospital admissions, with a mean cost of €16,754.2, and received treatments worth €435,609.2 (20.4% of the total expenditure).
The third subgroup comprised 170 cases (37.3%) with current or previous CBC by PA. These patients had a mean cost similar to that of the severe BE group (€8654.4). This was the subgroup with the greatest burden on the overall cost of the study, as its overall expenditure amounted to €1,471,248 (69.1% of the total).
Discussion
This is the first study on the direct annual costs of treatment in patients with BE and the determining factors involved. We found that patients with BE present a high annual cost, which is doubled at every severity stage, as measured by the FACED score, and increased by almost €1500 for every point in this scale. The variables associated with increased cost were age, the Charlson index, pulmonary function deterioration, the number of hospital admissions and CBC by PA. Most of the costs were attributable to inhaled bronchodilators and steroids, although in severe patients the greatest economic impact was due to exacerbations and inhaled antibiotics. Some subgroups presented a higher cost, such as the patients with BE associated with COPD, patients with frequent exacerbations or those colonized by PA.
The few pharmacoeconomic studies of BE to date, based on reviews of large databases in the United States, 8 –10 have already shown that patients with BE represent significant medical costs: an additional cost of $5681 per year with respect to controls without BE 8 ; an increase of $2319 in the first year after the diagnosis of BE, 9 and a mean cost of hospital admission for exacerbation of BE of $7827. 10 In our series we calculated the costs of each patient’s treatment directly case by case, applying unit prices taken from official sources, and obtained a mean cost of €4671.9. The discrepancy with the American studies may be due to differences in socioeconomic circumstances and healthcare systems, but also to the fact that we did not include the costs of complementary tests or indirect expenses (loss of productivity, ambulances, etc.). The aforementioned studies selected cases of BE by means of diagnostic codes and therefore lacked the clinical data that would allow them to correlate health costs with the severity of BE. We observed a notable increase in cost with increased severity of the disease, as measured by the FACED score. This reaffirms the importance of early diagnosis of BE, in order to apply treatments that prevent CBC and repeated exacerbations, and thus avoid a consequent increase in health costs.
The pharmacoeconomic literature on COPD is more extensive. 11 –14,32 –34 Several studies have found very variable costs ranging between US$2911 and €8575 per patient/year, with higher costs in severe COPD. 11 –14,34 These costs are not comparable, due to differences in the healthcare systems and methodologies involved. The mean cost in our series is higher than that in studies with similar methodologies and unit prices, 11,12 especially due to baseline treatments (basically inhalers and inhaled antibiotics), which represent 64% of the total cost. Most of the COPD studies exclude patients with BE, so our study is the first to evaluate financial aspects in patients with both diseases.
FEV1%, age, colonization by PA and the number of hospital admissions were variables independently associated with a higher total cost, as were FACED score and Charlson index. As hospital admission was the greatest unit cost, its statistical relationship with total cost is obvious. The rest of the variables were interrelated, and they represent an increased cost because they give rise to more treatments and hospital admissions. Thus, patients with an FEV1% < 50% received more intensive maintenance treatments (basically inhalers, oxygen therapy and physiotherapy) but also required more admissions (p < 0.001). Patients colonized by PA received expensive treatments and required more admissions (p < 0.001). Older patients presented a lower FEV1% and were readmitted to hospital more frequently. The association of FACED score with a higher cost is due to the fact that several of its component parts are independently associated with higher costs. Finally, the Charlson index has already demonstrated its relationship with higher sanitary costs. 35 As age plays a very important role in its final value, it is not surprising that it was also associated with higher costs in our patients.
We identified three subgroups of patients associated with higher costs: patients with BE associated with COPD, patients with more than two exacerbations and patients with CBC by PA. All of them are possible targets for interventions designed to reduce health expenditure. The first of these subgroups has scarcely been considered in pharmacoeconomic studies, as COPD studies tend to exclude patients with BE and vice versa. They presented a poorer FEV1%, required more maintenance treatments and hospital admissions. An early diagnosis of BE in patients with COPD is required (patients with FEV1 < 50%, isolation of PPM and at least one hospital admission in the previous year), 36 as well as an optimization of its baseline treatment in order to avoid CBC and exacerbations. The subgroup of exacerbator patients had a comparable cost per patient (€7520.5), and a considerable impact on the overall cost (34.5%), due to treatment of exacerbations, but also to baseline treatments, oxygen therapy and convalescence, which were heavily used. Finally, patients with CBC by PA were the subgroup with the greatest impact on overall cost (69.1%). They had more admissions than those who were not colonized, but most of their costs were due to their baseline treatments, particularly inhaled antibiotics (€3682.4 per patient). It is very important to investigate if early treatment after the first isolation of PA can avoid CBC, exacerbations and hospital admissions, and thus reduce costs.
Our study has the merit of being the first study to evaluate the direct annual cost of the treatment of BE in a group of patients managed along the same lines, monitored in specialized outpatient clinics for BE with a strict application of the available guidelines. 26,37 One limitation of the study is the small number of patients included. However, they are representative of those that are usually managed in specialized clinics. Given that they also come from very different populations, we believe that the costs results are applicable to most patients with bronchiectasis that are managed by Pneumologists in our country (Primary Care patients are probably less expensive). Another of the limitations of our study is the possible selection bias due to the exclusion of patients with insufficient data. Nevertheless, we consider it was minimal, thanks to the use of electronic medical records with systematic data collection. We used a cost for hospital admission (€3783.61) 27 that probably undervalued its impact. However, as we do not know the real cost of an admission for exacerbation of BE, we assigned this cost as it is a trustworthy parameter, as it was the mean cost of more than 7000 admissions in our country, and therefore applicable to all participating hospitals. Finally, we did not evaluate the possible influence on the cost of comorbidities, although we did evaluate Charlson comorbidity index, which was less strongly associated with total cost than the other variables.
Bearing in mind the results of our study, as well as the increase in BE prevalence 17,18 and in the number of hospital admissions it causes, 10,19 strategies are required to optimize its management. It would be appropriate to monitor severe patients in specialized outpatient clinics for BE, in order to harmonize the baseline treatment according to available guidelines 26,37 and apply antibiotic treatments at the correct dosages and time periods, thereby controlling CBC and reducing the need for hospital admissions. Strategies that need improvement include patient self-care 38 and the use of day hospitals and home intravenous antibiotic therapy 39 in case of exacerbation. The great outlay on inhaled corticosteroids is striking and should be reduced, given the scanty evidence on its benefits and the possibility that it may be counterproductive by altering airway microbiome. 40 We believe that pharmacoeconomic studies like this one are necessary, in order to help determine whether specific treatments such as inhaled antibiotics, are cost-effective as a means of reducing hospital admissions or the need for more expensive therapies.
In conclusion, our results show that patients with BE represent a high direct annual cost in treatments, which rises with the severity of the disease, as measured by the FACED score. The variables associated with higher costs are FEV1%, age, colonization by PA and the number of hospital admissions. It is essential to establish clinical management strategies to optimize expenses in the stable phase, reduce the exacerbations and hospital admissions, control CBC and make an early diagnosis of BE in patients with COPD. In order to define more precisely the real impact of BE on the healthcare system as well as the efficiency of the treatments applied, further studies are needed to calibrate the overall cost of patients by including both direct and indirect expenses, along with the real cost of hospitalization for BE.
Footnotes
Acknowledgments
Juan Carlos Martínez Sánchez, Àrea de Bioestadística, Universitat Internacional de Catalunya, Barcelona: performed the statistical analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.