
Abstract
Acute exacerbations of chronic airway disease are common occurrences that cause a major burden of illness. Acute exacerbations are associated with impaired health status, increased lung function decline, hospitalization and increased risk of death. Exacerbation avoidance is a major priority. Despite this goal, exacerbations continue to occur and the need for effective models of care that optimize patient outcomes are urgently needed. ‘Treatable Traits’ is an approach to personalized medicine that has been proposed for the management of airway diseases. The treatable traits approach allows for the recognition of clinically important, identifiable and treatable disease characteristics, followed by targeted and individualized treatment interventions to address each trait. We review the literature relating to treatable traits in airway diseases; in particular, those traits that can predict exacerbations and approaches to management that aim to prevent exacerbations by using a treatable traits model of care. We propose this approach as a potentially useful model of care to both prevent and manage acute exacerbations.
Introduction
Chronic airway diseases are common and have a significant burden on affected individuals, their families and health-care systems. 1 Worldwide, lung conditions are one of the most frequent causes of death. 2 The breadth of conditions that fall under the term of a chronic airway disease include asthma, chronic obstructive pulmonary disease (COPD), cystic fibrosis (CF) and bronchiectasis. Each disease is characterized by acute exacerbations, defined as an acute worsening of respiratory symptoms that require a treatment change. These events range from mild to severe.
Exacerbations impose major negative health impacts upon individuals and a high cost burden upon society. Exacerbations are important as they speed the progression of disease, increase the decline in lung function and are related to significantly greater risk of hospitalization and mortality in asthma, COPD and bronchiectasis. 1,3 Exacerbations therefore are highly important events. The major goals of management in chronic airway diseases are exacerbation prevention and prompt and effective management of exacerbations when they do occur.
COPD, asthma and bronchiectasis are complex. They each have diverse aetiology and disease mechanisms, and manifest a range of symptoms. The impact of each disease on individual patients is also heterogeneous, which means that not all disease manifestations occur in every person, or in the same person at all times. This heterogeneity and complexity has led to the recognition that treatment approaches cannot be ‘one size fits all’, but individualized strategies to patient care are needed, or in other words, personalized medicine approaches for chronic airway diseases. 4 –7 The ‘Treatable traits’ strategy is an approach that has be proposed as a way to implement personalized medicine for chronic airway disease. Treatable traits are disease characteristics that are clinically relevant, identifiable and modifiable (Figure 1). 4,5,7 In this review, we will examine the potential application of a treatable trait strategy for patients with chronic airway diseases, namely COPD, asthma and bronchiectasis, as these are the conditions where the treatable traits strategy has been proposed. Typically, the treatable traits concept has been applied to the management of adults with asthma and COPD in their stable phase. Our focus is to explore the application of treatable traits as predictors of exacerbations and during acute exacerbations of adults with airway diseases.

Treatable traits domains and criteria to be considered a trait. Figure reproduced with permission from the Centre of Excellence in Severe Asthma (https://www.severeasthma.org.au)
The burden of chronic airway disease
Chronic airway diseases have a significant burden, with persistent symptoms, reduced health-related quality of life (HRQoL), associated morbidity and mortality and associated health-care costs.
Asthma directly affects an estimated 330 million people worldwide, 8 of which approximately 3–10% have severe treatment-refractory disease. 9,10 People with severe asthma experience uncontrolled symptoms, 11 impaired quality of life, 12,13 frequent exacerbations, hospitalizations 14 and are at increased risk of death. 15 Asthma also places a substantial financial burden on both individuals (e.g. medication costs and reduced work capacity) and society (e.g. health-care costs, reduced workplace productivity). 16 –18 Asthma exacerbations are responsible for 0.6% of all hospital admissions in Europe, as well as lost time at work/school, 18 and death. 15 In 2016, the Global Burden of Disease collaboration estimated that 420,000 people in the world died from asthma, that is, more than 1000 deaths worldwide per day. 19
An estimated 251 million people worldwide have COPD, based on WHO estimates. 20 COPD is currently the third leading cause of mortality worldwide, 21 with over 3 million reported deaths in 2016 (5.4% of all global deaths). 20 Acute exacerbations occur in up to half of patients and approximately 20% require hospitalization. 22 COPD is the second leading cause of preventable hospital admissions, with rates of admission predicted to exceed that of ischaemic heart disease within the next 5 years. 23 In 2016–2017 in Australia 78,000 potentially preventable hospital admissions were recorded. 24 It is therefore unsurprising that COPD is associated with poorer HRQoL, worse functional impairment and significant healthcare costs.
The burden of bronchiectasis is becoming increasingly recognized worldwide; however, there remains a paucity of prevalence data. Quint et al. sought to determine the incidence and prevalence of bronchiectasis in adults from the United Kingdom, between 2004 and 2013 and identify its impact upon mortality. Using data from the Clinical Practice Research Datalink, a large computerized database of longitudinal primary care medical records, they report increasing bronchiectasis incidence and prevalence. The point prevalence of bronchiectasis increased in women from 350.5 per 100,000 people in 2004, to 566.1 per 100,000 people in 2013. Similarly in men, the prevalence increased from 301.2 per 100,000 people in 2004, to 485.5 per 100,000 people in 2013. 25 These rates increased over the study time and were higher in older people. Another large study from Germany estimated the prevalence of bronchiectasis to be slightly lower (an estimated 67 cases per 100,000 in 2013). 26
Acute exacerbations
Exacerbations or lung attacks are a major contributor to disease burden across these chronic airway diseases. 27 Exacerbations refer to episodes of acute worsening of disease symptoms, which commonly result in increased healthcare use, hospitalizations, reduced quality of life and may cause death.
In adults with asthma, exacerbations are a major cause of morbidity. 28 Exacerbations are most common in uncontrolled asthma and can be triggered by pathogen (e.g. virus and/or bacteria), allergen or occupational exposures, stress or sub-optimal adherence to preventer medications. 29 Epidemics of severe asthma exacerbations can also be triggered by major environmental events, such as wildfire smoke or thunderstorm events, which trigger high levels of respirable pollen allergens. 30,31
In COPD, exacerbations are typically triggered by infections (viral or bacterial) or air pollutant exposure. COPD exacerbations commonly lead to hospitalization, accelerated lung function decline, poor health status and increased mortality. 32 In fact, in COPD, the mortality risk at 1 year following a hospitalization for an acute exacerbation is approximately 25%, 33,34 which is greater than the mortality risk of someone hospitalized for an acute myocardial infarction. 35
Exacerbations are also a cardinal feature of bronchiectasis, where they are associated with more severe disease and chronic colonization of the airway with pathogenic bacteria such as Pseudomonas aeruginosa. 36 Despite exacerbations being a feature of the natural history of this disease, these events are not without consequence. In a prospective cohort study of 608 patients with bronchiectasis Chalmers et al. reported that patients with three or more exacerbations per year have double the mortality rate of those who do not experience exacerbations (hazard ratio 2.03 (95% confidence interval 1.02–4.03)). In addition to the associated mortality risk, acute exacerbations in bronchiectasis also significantly impact HRQoL. 37
These data confirm that acute exacerbations of airway disease are common occurrences with significant consequences. Exacerbations are associated with increased decline in lung function, poor quality of life and increased mortality. The avoidance of attacks in chronic airway disease is therefore imperative, a point highlighted in the recent Lancet commission on asthma, which called for zero tolerance of attacks, with an emphasis on precision medicine rather than a one-size-fits-all approach to treatment and secondary prevention. They also call for an abandonment of the terms exacerbations and flare ups, in favour of attacks, in an effort to change our weak responses to these sentinel events. 1 Precision medicine requires measurement of biomarkers to determine individual treatable traits, and when applied in the context of exacerbation prevention, it is hoped that this will identify at-risk patients and perhaps empower patients in their treatment decisions towards the commitment to individualized life-long prophylactic treatment. 1
While strategies to optimize long-term management of chronic airway disease have steadily improved, approaches that limit the impact of acute exacerbations have lagged. We do know however that in asthma, COPD and bronchiectasis, the best predictor of future attacks is the history of a previous one. 37 –39 Identifying this trait in patients and focusing on avoidance of exacerbations through individualized and effective treatments, adherence, self-management strategies and education, public health messages, and new drug discovery and development is a way to move forward in secondary prevention strategies.
Treatable traits: An emerging approach for chronic airway disease management
The concept of treatable traits in airway diseases has developed over the last decade following recognition that asthma and COPD are complex syndromes which require individualized assessment, investigation and treatment. 5,6,40 The treatable trait strategy was initially proposed in 2016, 5 building on previous work that proposed multidimensional assessment and treatment approaches for individual respiratory diseases, for example, in asthma. 6 Subsequent international workshops have been convened to seek expert consensus on how to apply and progress a treatable traits strategy for clinical management. 4,7 While proposed for management in stable disease, the principles of treatable traits easily fit within management of acute exacerbations. Notably assessment of traits in stable disease can also identify important predictors of future attacks and hence identify treatment targets for exacerbation prevention. However, while this has been proposed, 38 it has not yet been tested in efficacy studies.
The treatable traits strategy incorporates a number of elements. Inherent to its approach is a multidimensional assessment of each individual patient to determine which traits exist in that patient. Traits are categorized into the three domains of pulmonary traits, extra-pulmonary traits and behaviours/lifestyle risk factors of airway diseases (Figure 1). Multidimensional assessment can be used to identify the range of traits within an individual and involves a clinical history and examination, an evaluation of risk factors, and measurement of spirometry, FeNO and blood eosinophils. Following this, if the probability of airway disease is high, irrespective of the disease label, assessment of treatable traits followed by individualized management is recommended. 5 The Treatable traits strategy aims to support an individualized and targeted treatment approach, which is broadly applicable independent of disease diagnosis. This is in contrast to current guideline-based recommendations that are disease specific.
A treatable trait can be defined as a therapeutic target identified by phenotypes or endotypes through a validated biomarker. 5 The biomarker is not necessarily a specific molecule but also includes findings from other assessment techniques such as imaging, lung function or patient-reported outcome measures. 7 In the treatable traits paradigm, these are referred to as trait identification markers (TIMs). 7
Important to the treatable traits approach is the recognition that a given patient is likely to have multiple traits, and that each of these traits is important. In a population of patients with stable obstructive airway disease who underwent a multidimensional assessment of traits, we reported that the mean (SD) number of traits identified was 11.3 (2.5). Furthermore, each additional trait identified was associated with a clinically important decrement in HRQoL. 41 The temporal stability of traits in patients with chronic airway disease is not known, and we expect that traits will differ during different stages of the disease course. This is particularly important if the treatable traits strategy is to be applied during acute attacks.
To be considered a candidate treatable trait there are three characteristics that must be fulfilled. A trait must (1) have clinical relevance, (2) be identifiable and measurable and (3) be treatable (Figure 1). 7
Personalized medicine has been defined as an approach where treatments are targeted to the needs of individual patients on the basis of genetic, biomarker, phenotypic, or psychosocial characteristics that distinguish a given patient. 42 Essential in this definition is the goal of improving clinical outcomes for individual patients and minimizing unnecessary side effects for those less likely to have a response to a particular treatment. 42 The treatable traits strategy is a vehicle for the implementation of such an approach as it importantly recognizes that chronic airway diseases are heterogeneous, multisystem diseases that require patients to be active participants in their disease management. Proposed traits that are relevant to exacerbations of chronic airway diseases are presented in Table 1.
Treatable traits relevant to exacerbations of chronic airway diseases.

VCD: vocal cord dysfunction; COPD: chronic obstructive pulmonary disease; AECOPD: acute exacerbation of COPD.
a Research setting.
A further aspect of treatable traits is the possibility of using a ‘label-free’ approach to airway disease management. This approach recognizes the similarities in the different obstructive airway diseases, and their significant overlap. This means that an individual may have diagnostic features of more than one disease. This has been explicitly described in asthma and COPD, where the asthma-COPD overlap syndrome has been extensively studied. 43 However, it is also recognized that bronchiectasis can overlap with asthma and/or COPD. 44 Since acute attacks are a feature of each of the obstructive airway diseases, there may be value in using a label-free approach in assessing and managing these events.
Applying a treatable traits approach to exacerbations of chronic airway disease
Many potential treatable traits have been proposed in the treatable trait strategy. In the 2016 proposal by Agusti et al., there were 31 traits presented. 5 In the Lancet commission on asthma, which also recommends the treatable traits approach, there were 14 traits identified, 1 and in the multidimensional assessment and individualized management of asthma in the elderly, Gibson et al. proposed 22 traits. 6 As previously stated, these were considered in stable disease; however, many traits either predict future exacerbation or have relevance during acute exacerbations.
To date there are no randomised controlled trials (RCTs) in acute exacerbations that have applied a broad treatable traits approach to identify relevance of multiple individual traits to disease outcomes or that evaluate how to prioritize assessment and treatments. RCTs of the treatable traits approach are needed. In a proof of concept study, McDonald et al. applied a multidimensional assessment and individualized management targeted to identified traits in a stable COPD population. The intervention resulted in major improvements in health status (14 unit improvement in the St. George Respiratory Questionnaire for the intervention group versus 2.2 unit for the control), and biological outcomes (high -sensitvity C-Reative Protien (hsCRP), sputum eosinophils and neutrophil counts). While there were trends for fewer exacerbations this was not significant, although the numbers were small (N = 34). 45 Other studies have tested interventions that target a specific trait, with positive effects. The inflammometry studies of Green et al., 46 Jayaram et al. 47 and Powell et al. 48 are good examples of treatment targeted to the T2 inflammation pathway, that is, using sputum eosinophil counts or FeNO to identify the trait and direct treatment decisions accordingly. When treatment was titrated according to these biomarkers, attacks were reduced by at least 40%. These studies show support for the treatable traits approach in a stable population. They demonstrate that a treatable traits approach can be used as secondary prevention of attacks in asthma and COPD. These promising results identify a need for more research, with the acute care setting being relevant.
A range of treatable traits have been linked to exacerbations in asthma, COPD and bronchiectasis. In asthma, a 2019 study that evaluated patients with severe asthma and a non-severe comparison group with well controlled asthma from the Australasian Severe Asthma Wed-based Database reported 24 traits that could be identified.
38
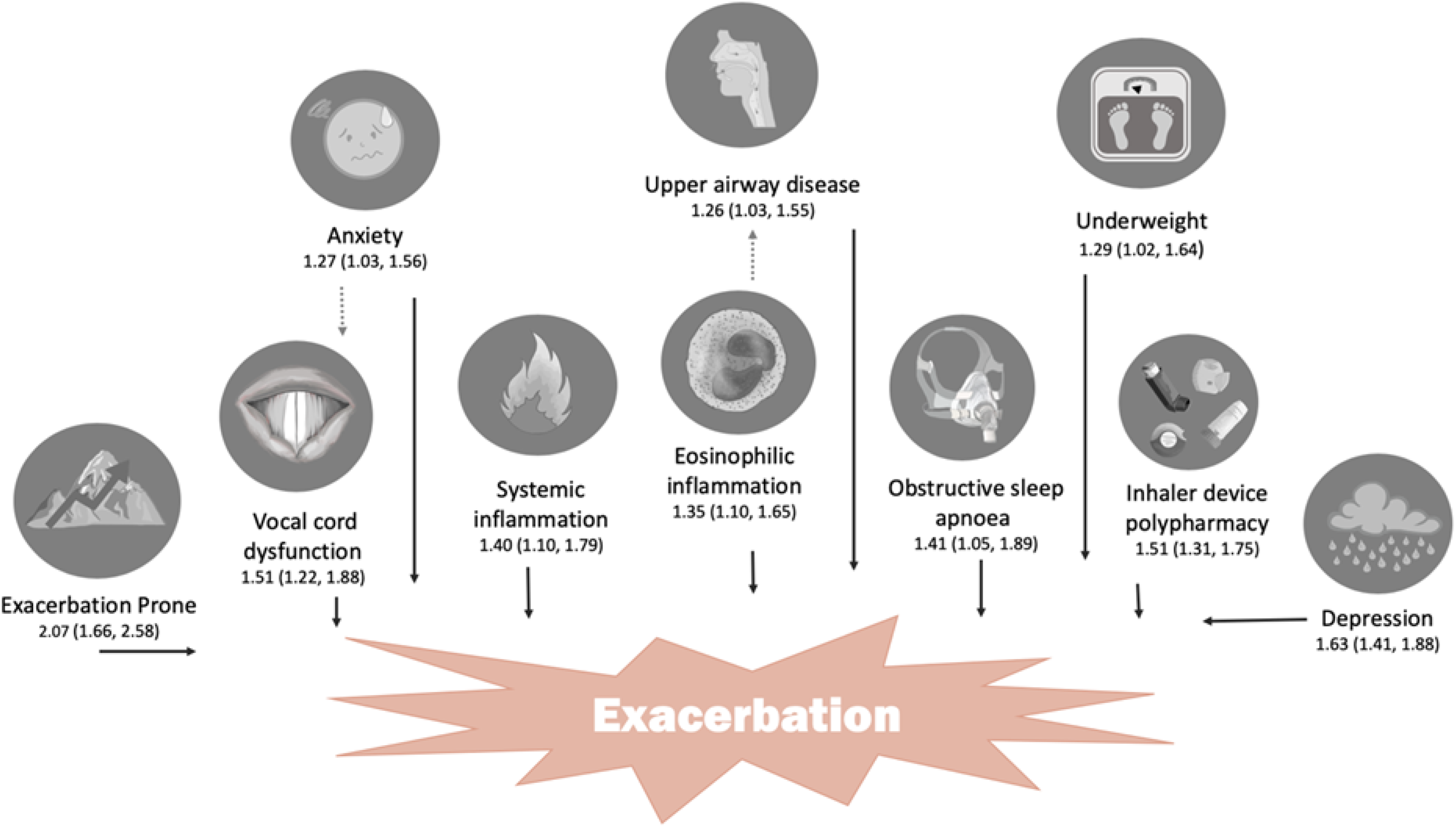
In this study, participants underwent a baseline assessment and were followed up prospectively every 6 months for up to 2 years. Using negative binomial regression analysis, 10 traits that predicted future exacerbation risk were identified. The biggest predictor of future attack was being exacerbation prone. Other traits that predicted future exacerbation in asthma were depression, inhaler device polypharmacy, vocal cord dysfunction (VCD), obstructive sleep apnoea (OSA), eosinophilic inflammation, anxiety, systemic inflammation, upper airway disease and being underweight (Figure 2).
38
Targeting treatment to such traits with the highest risk profile may reduce exacerbation frequency and severity in an asthma setting, but this approach is yet to be evaluated. Treatable traits that predict future attacks in asthma. Source: Reproduced with permission of the © ERS 2019: European Respiratory Journal 53 (5) 1802058; DOI:10.1183/13993003.02058-2018 Published 9 May 2019. Adapted with permission Repirology.
38
The Evaluation of COPD Longitudinally to Identify Predictive Seconary End-points (ECLIPSE) study identified COPD phenotypes specifically relevant to acute exacerbations. 49,50 A ‘frequent exacerbation’ population, which was not dependent on disease severity, was predicted by previous exacerbation history and associated with impaired health status, history of gastro-oesphageal reflux disease and increased white blood cell counts. 39 A further study identified subtypes termed severe respiratory COPD (at elevated risk of severe exacerbations), moderate respiratory COPD and systemic COPD. 51 Elevated eosinophilic inflammation was associated with increased risk of severe exacerbations among people with COPD in the general population. 52 Further biomarkers that predicted exacerbation risk include C-reactive protein (CRP) and procalcitonin. 50
Treatable traits in acute exacerbations
Acute exacerbations of airway disease are complex and heterogeneous events. Studies that investigate the heterogeneity of acute exacerbations identify several distinct traits. A study of patients with acute exacerbations of COPD in hospital used imaging and diagnostic biomarker assessment to characterize patients and suggested that elevated CRP levels may indicate pneumonia, while elevated NT-proBNP may indicate cardiac dysfunction. 53 A further attempt to phenotype COPD patients using molecular microbiological techniques identified bacteria- and virus-positive groups or pathogen-negative patient groups. 54 Among this population already in hospital with an acute exacerbation of COPD, the bacteria-positive subgroup had the best prognosis and the pathogen-negative group had the worst prognosis. 54
More recently, Prins et al. reported the results of an RCT where CRP was used as a biomarker to direct antibiotic treatment in patients admitted to hospital with an acute exacerbation of COPD. Patients were randomized to receive biomarker directed antibiotic treatment if CRP was ≥50 mg/L (n = 101) or guideline-based antibiotic treatment according to patient reported symptoms (n = 119). Fewer antibiotics were prescribed in the CRP guided group (31.7% vs. 46.2%, p = 0.028; adjusted odds ratio (OR) 0.178 [95% CI 0.077–0.411], p = 0.029). There were no differences in 30-day treatment failures or time to first exacerbation. This novel study provides support for biomarker-driven antibiotic treatment targeting a treatable trait during acute exacerbations. 55
In a study by Bafadhel et al. who sought to characterize acute exacerbation clusters in a group of 145 outpatients with COPD experiencing 183 exacerbations, the clusters identified were bacterial-, viral-, or eosinophilic-predominant, and a fourth, ‘pauci-inflammatory’ (associated with limited changes in the inflammatory profile). 56 These clusters were otherwise clinically indistinguishable and thus highlight the importance of identifying individualized traits to deliver personalized treatments. Bafadhel et al. extended this work by investigating the utility of peripheral blood eosinophils to direct oral corticosteroid treatment during acute exacerbations of COPD. In an RCT comparing biomarker-directed treatment of acute COPD exacerbations compared to standard care 164 participants were recruited; 55 and 54 patients allocated to the biomarker-driven treatment and standard care groups, respectively. The primary outcome of non-inferiority of health status in the standard therapy and biomarker-directed groups after 2 weeks of treatment was achieved (Chronic Respiratory Questionnaire mean score change, 0.8 vs. 1.1; mean difference, 0.3 [95% CI: 0.0–0.6], p = 0.05). Further, there were more treatment failures in the standard care group versus the biomarker directed group and no differences in FEV1 or % improvement in a visual analogue scale. 57 This study suggests targeted corticosteroid treatment of acute exacerbations is safe and has potential to reduce harm in patients characterized with the treatable trait of eosinophilia. It is important to note, however, that this study was conducted in patients with exacerbations managed in the outpatient setting.
Another RCT that involved hospitalized patients with acute COPD exacerbations tested a biomarker driven approach to systemic corticosteroid administration during the exacerbation. Patients were randomized to either eosinophil-guided therapy (n = 159) or standard therapy with systemic corticosteroids (n = 159). The biomarker driven treatment approach was not inferior to standard care for the primary outcome of days alive and out of hospital within 14 days after recruitment (mean 8.9 days [95% CI: 8.3–9.6]) in the eosinophil-guided group versus (9·3 days [8.7–9.9]) in the control group (absolute difference −0·4 [95% CI:−1.3 to 0.5]; p = 0.34). Further there were no differences in treatment failures at 30 days. Systemic corticosteroid exposure, however, was less in the eosinophil-guided group compared to control (2 days (IQR: 1.0–3.0) vs. 5 days (5.0–5.0); p < 0.0001). 58 Again, this study suggests that biomarker-driven treatment targeting a treatable trait may reduce harm by minimizing unnecessary treatment and their associated adverse effects.
Further studies involving hospitalized patients are indicated. A recent study conducted by MacDonald et al. examined the relevance of blood eosinophil counts in patients hospitalized due to acute exacerbations of COPD, 59 demonstrating a strong link between increased eosinophil counts and a reduced presence of infection (CRP≥ 20mg/L or PCR positive). Interestingly, this is one of the first studies in this patient group to highlight the importance of abnormally low eosinophil counts (eosinopenia), which was associated in both the derivation (retrospective) and the validation (prospective) cohorts with poorer clinical outcomes such as longer length of stay and 1-year mortality compared to those with normal or higher levels of eosinophils. The observational nature of this study, however, precludes confirmation of causality by an ‘infective’ phenotype.
Recognizing the potential benefits of phenotyping COPD exacerbations MacDonald et al. have proposed a novel approach to phenotyping during hospitalizations for acute exacerbations of COPD. This approach attempts to describe the aetiologies of acute exacerbations in COPD using the acronym ABCDEFGX in an effort to focus clinician attention on relevant management issues, which can otherwise be known as ‘traits’, both during the admission and at follow up. 60 The traits proposed in this acronym includes Airway viral infection, Bacterial infection, Coinfection, Depression/anxiety, pulmonary Embolism, cardiac Failure (or failure of lung integrity – pneumothorax), General environment and X (unknown). 60 The authors went on to apply this characterization in a pilot study of 52 patients admitted to hospital with an acute exacerbation of COPD. They identified multiple exacerbation phenotypes and also identified a population at risk of longer hospital length of stay, that being patients who were co-infected with both a bacterial pathogen and virus. 61
Applying a treatable traits approach during the hospitalization
Patients admitted to hospital with an acute exacerbation, irrespective of their chronic airway disease are at risk of future exacerbation, protracted recovery, 3,62 –64 impaired health status and death. 35 The events are frightening for patients and create disruption to people’s lives. As such the impacts go beyond the days in hospital and the individual. Other family members and their livelihood are also affected. 65 Data also suggest that after a hospitalization patients do not return to their prior baseline health status. 66,67 Identification of treatable traits within the hospital setting for patients with acute respiratory exacerbations can facilitate more accurate identification of exacerbation aetiology, risk factors and targeted management during and following the period of hospitalization. The treatable trait concept, at its very essence, is ‘label-free’, conferring equal relevance to diseases such as asthma, COPD and bronchiectasis. The traits are clinically important, and the period of hospitalisation may facilitate more ready access to test procedures (TIMs) facilitating their identification and initiation of treatment. We propose that a treatable traits strategy can be applied during this acute phase of illness and can aid in recovery and exacerbation prevention. We have identified the traits proposed in the 2016 publication by Agusti et al. 5 that are most relevant in predicting acute exacerbations and have suggested TIMs for each trait, and the recommended treatment (Table 1). To maximize efficiency and provide best practice care, implementation of the treatable traits strategy requires multidisciplinary team approaches. It is important to acknowledge, however, that this is a proposal and data to specifically validate such an approach in the inpatient setting are indicated.
In addition to the treatable traits proposed in earlier work, we have also identified potential new traits of particular relevance to acute exacerbations, including frailty and impaired physical function.
Frailty
Frailty is most commonly defined as an accumulation of physiological deficits across multiple interrelated systems that results in both concurrent functional limitations and vulnerability to new stressors.
68
Within respiratory medicine, frailty may be conceptualized as a driving factor underpinning some observations of heightened accelerations in functional decline and protracted recovery from acute respiratory exacerbations (Figure 3). In COPD, where most of the limited respiratory data has arisen, frailty has been shown to be more common in people with greater age, disease severity, dyspnoea and co-morbidity burden. Having frailty is not a normal part of healthy ageing and is associated with an increased risk of falls, hospitalizations and disability.
69
–72
While evaluation of frailty is not yet advocated within respiratory medicine guidelines, its prevalence has been estimated as occurring in up to 19% of people with stable COPD,
73
which is almost double that of the general adult community (10%).
68
Episodes of acute illness increase one’s susceptibility to having frailty. Recent data suggest that frailty may be present in over 40% of inpatients with AECOPD and independently increase the risk of 90-day respiratory-related readmission or death.
74
Theoretical model highlighting the impact of frailty and acute respiratory exacerbations (red lightning bolts) on acceleration of disability in people with chronic respiratory disease. Source: Reprinted with permission of the American Thoracic Society. Copyright © 2019 American Thoracic Society: Singer, JP, Lederer DJ & Baldwin MR (2016), Frailty in pulmonary and critical care. Ann Am Thorac Soc, 13(8), 1394–1404. The Annals of the American Thoracic Society is an official Journal of the American Thoracic Society.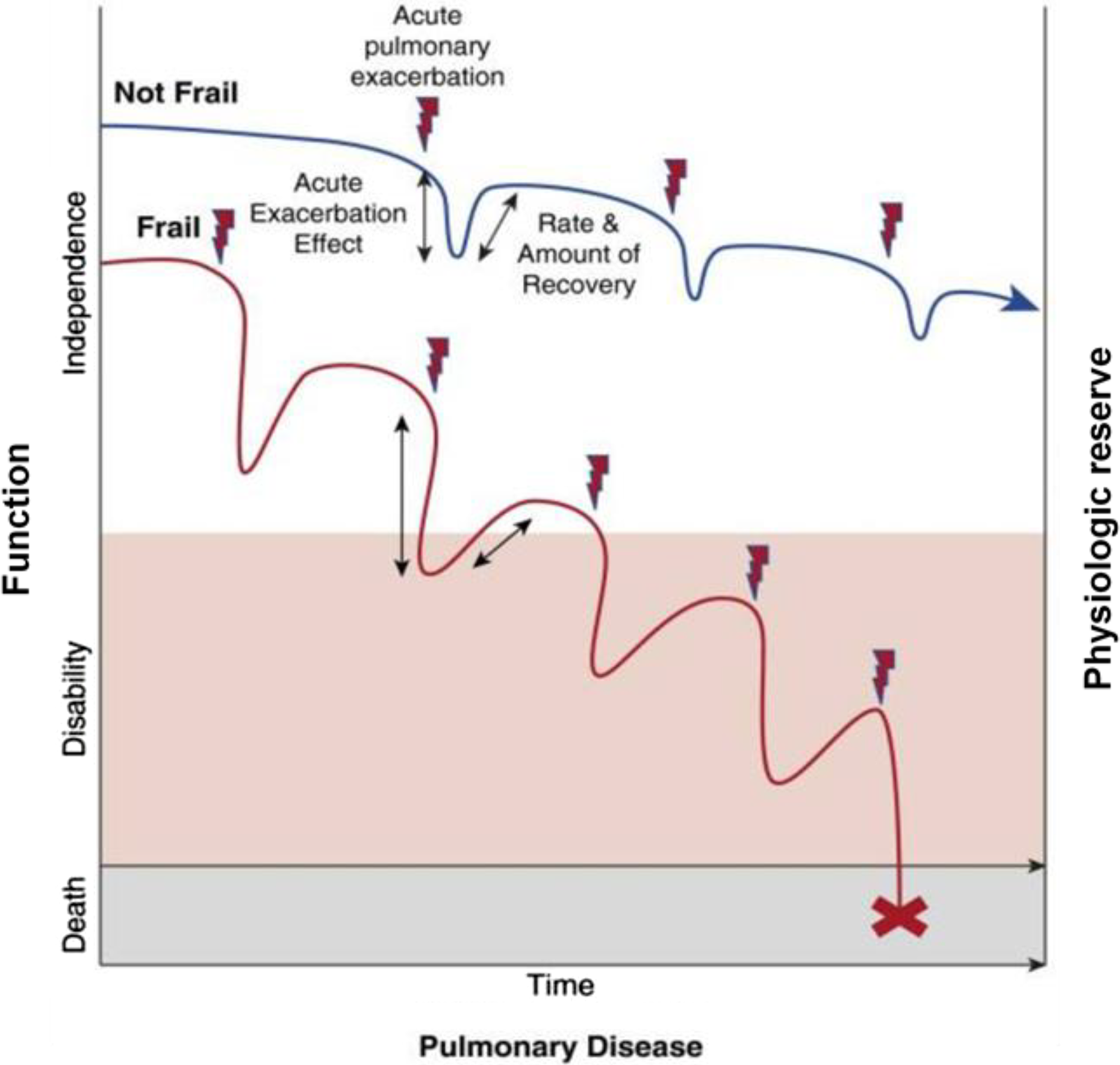
Impaired physical function
Impaired physical function is a trait that can be conceptually distinguished by pathophysiological muscle dysfunction (e.g. low muscle strength or mass, sarcopenia) and/or sub-optimal functional performance (exercise intolerance, physical inactivity/sedentary behavior). Each may occur in isolation or as an interaction with others. Various physiological and behavioural mechanisms may underpin the presence of this trait during acute respiratory exacerbations. These may include factors related to airway or systemic inflammation, systemic corticosteroid use, malnutrition or physical inactivity). 75 Confirmatory evidence to identify such factors at the clinician–patient interface during acute respiratory exacerbations is, however, rare.
Trait identification markers related to impaired physical function may take various forms such as objective evaluation of muscle strength or mass, physical tests of functional performance (e.g. field walking tests, gait speed, chair-stand tests), assessment of physical activity (objective or subjective) or questionnaire-based evaluations of activities of daily living (e.g. Katz index). As no single test represents the full breadth of physical function impairments, multiple testing appears advisable. Composite metrics such as the short performance physical battery (which includes evaluation of gait speed, chair-stand performance and balance) 76 may offer appeal to address multiple domains in a timely manner. No preference should be given to one aspect of impaired physical function over another. Subjective reports of behaviors such as physical activity levels are known to lack accuracy compared to objective measures. A physical examination (i.e. direct observation and recording of performance) by a suitably trained professional is therefore essential to accurately evaluate this trait. Examples of trait identification markers related to impaired physical function are outlined further in Table 1. It is important to note that, unlike some other traits (e.g. pulmonary traits), various forms of rehabilitation are most commonly utilized to manage impairments of physical function. This means the time of an acute respiratory exacerbation is a potentially suitable opportunity to detect this trait, however, treatment of this trait will largely take place at a time after discharge from hospital.
Conclusions
Acute exacerbations frequently occur in chronic airway diseases. These events cause dire and long-lasting effects. The need to minimize exacerbations and effectively treat these events if they occur is urgent. This requires innovative approaches to recognizing traits that predict future exacerbations and testing interventions that prevent exacerbations, beyond our armamentarium of current and often ineffective approaches. Personalized approaches to treating exacerbations are also needed. The treatable traits strategy is an approach that recognises clinically important, identifiable and treatable characteristics of disease. It uses biomarkers to identify traits and applies targeted and personalized interventions for the identified traits. Applying this approach in the prevention and treatment of acute exacerbations of airway diseases could potentially advance management and lead to improved patient and economic outcomes. Future research in the acute setting evaluating biomarkers and treatable traits approaches is a current research priority.
Footnotes
Acknowledgements
The authors wish to acknowledge Dr Steven Maltby for his assistance with the literature search, and Dr Tegan Grace for assistance with formatting.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: VMM has participated in educational symposia funded by GlaxoSmithKline, AstraZeneca and Menarini and has participated advisory boards for GlaxoSmithKline, AstraZeneca and Menarini. PGG holds an NHMRC Practitioner Fellowship, has participated in educational symposia funded by AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline and Novartis, and has participated in studies funded by GlaxoSmithKline and AstraZeneca. CO was the recipient of a Lung Foundation Australia/Boehringer-Ingelheim COPD Research Fellowship (2017-18), but reports no conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.