
Abstract
Chronic obstructive pulmonary disease (COPD) is projected to be the third leading cause of death by 2020. Early detection and screening may alter the course and prognosis associated with lung disease. We investigated the effectiveness of a voluntary public lung function screening program and factors that had a predictive value for asymptomatic COPD in Xi’an, China. Pulmonary function testing (PFT) was conducted on volunteers recruited from four community centers in Xi’an, China, between July and August 2012. Participants underwent three forced vital capacity maneuvers. The maneuver with the best forced expiratory volume in first second was retained. Participants filled out a medical history and environmental exposure survey before undergoing the PFT. Patients who self-reported lung disease on the health survey were excluded from the analysis. Logistical regression was used to determine associations with airway obstruction. A total of 803 volunteers participated in this study, and 33 subjects were excluded as the participants did not meet the requirements of PFT. Of the 770 volunteers, 44 participants had been diagnosed with chronic respiratory diseases previously, and 144 participants (18.7%) met COPD criteria. Four hundred forty-four participants did not self-report any respiratory symptoms, and the remaining 282 participants self-reported respiratory symptoms. Of the asymptomatic participants, 98 volunteers had PFT results that were consistent with COPD and 68.1% of asymptomatic participants were undiagnosed. A greater percentage of women than men had moderate or severe airway obstruction (p = 0.004).Only smoking status (odds ratio = 2.64, 95% confidence interval 1.20–6.04) was associated with asymptomatic COPD. Voluntary public lung function screening programs in China are likely to identify a large number of undiagnosed, asymptomatic COPD. Smoking status is associated with airway obstruction and a greater percentage of women than men had moderate or severe airway obstruction.
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by a persistent decrease in airflow and shortness of breath. Data from the National Health and Nutrition Examination Survey showed about 15% of US adults aged 40–79 had any airway obstruction, with 9.4% having mild airway obstruction and 5.3% having moderate or severe lung. 1 COPD is projected to be the third leading cause of death by 2020. 2 –5 Its prevalence and consequent burden are expected to rise with rapidly increasing smoking rates in developing countries. This risk factor combined with an aging population accounts for the actual and forecasted rapid growth in chronic obstructive disease.
However, the prevalence of COPD is probably underestimated, since it is not usually diagnosed until it is clinically apparent and moderately advanced. Potentially, most COPD can be prevented by modification or reduction of the main causal risk factor, cigarette smoking, through smoking cessation. 6,7 Additionally, efforts can be made to prevent the rapid progression of disease through screening and early detection of COPD, which generally entails spirometry, targeting of individual symptoms, or a combination. One mechanism for early detection is a voluntary public screening program. An example of voluntary screening is a respiratory therapist setting up a booth at a county fair and offering spirometry to anyone who walks by and is interested. 8
Pulmonary function testing (PFT) has been shown to be a predictor of cardiorespiratory morbidity and mortality. 9 Early stage lung diseases can also be detected by PFT. 10,11 However, compared with screening programs for hypertension and hyperlipidemia, PFT is generally not part of blanket health screening methods. To date, no consensus exists on how, when, and where public screening with spirometry should be implemented. There has been no formal study on the effectiveness of voluntary public screening programs in China. The objective of this study is to investigate the effectiveness of a voluntary public lung function screening program and factors that had a predictive value for asymptomatic COPD in Xi’an, China.
Methods
Subjects
Xi’an is divided into four districts according to administrative region: North, East, South, and West. Two communities in each district were selected for voluntary public screening. The participant inclusion criteria for screening were age between 18 and 80 years and residency in their current community for at least 2 years. Participants provided informed consent and completed a heath questionnaire and PFT evaluation between July and August 2012. Patients who self-reported chronic lung disease on the health survey were excluded from the analysis. This study was approved by the ethic committee from the First Affiliated Hospital of Xi’an Medical University.
Design of questionnaire
Participants filled out a modified ATS-DLD-78 Questionnaire. 12 Survey content includes medical history, blood pressure, chronic lung disease history (defined as interstitial lung disease, COPD, asthma, chronic bronchitis, and bronchiectasis), smoking status, and primary meal preparer (due to exposure risk).
Pulmonary function test
Forced vital capacity (FVC) and forced expiratory volume in first second (FEV1) were measured by portable spirometer (Spirobank, GTM, Medical International Research, Rome, Italy). Participants underwent three FVC maneuvers, and the maneuver with the best FEV1 was retained. Efforts that were incomplete or in which the patient coughed were excluded. PFTs were performed by staff certified in PFT administration.
Definition and severity of COPD
Based on lung function values obtained from a pre-bronchodilator spirometry examination, airway obstruction was defined as an FEV1 to FVC ratio less than 0.7. 13 Mild airway obstruction was defined as an FEV1 greater than 70% predicted among those with airway obstruction. Moderate or severe airway obstruction was defined as an FEV1 less than or equal to 70% predicted among those with airway obstruction. 13 All predicted values were based on the Knutson prediction model. 14
Statistic method
The data were analyzed using JMPTM version 10 (SAS Inc., Cary, North Carolina, USA) and GraphPad Prism™ version 5.0 (GraphPad Software Inc, San Diego, California, USA). Fisher’s exact test or χ 2 was used for the analysis of categorical variables. The analysis of variance test was utilized to compare measurement variables. Logistic regression was used to further analyze the factors between normal and COPD. Results are reported as mean ± standard error of mean, with p < 0.05 was considered statistically significant.
Results
A total of 803 (Figure 1) volunteers participated in this study, of which 33 subjects were excluded as the participants did not meet the requirements of PFT. Of the 770 volunteers, 44 participants had been previously diagnosed with chronic respiratory diseases, and 144 participants (18.7%) met the COPD criteria. Four hundred and forty-four participants did not self-report respiratory symptoms, and 282 participants self-reported respiratory symptoms. Of the asymptomatic participants, 98 volunteers had PFT results that were consistent with COPD and 68.1% of asymptomatic participants had previously undiagnosed airway obstruction (Figure 2).

An overall flow diagram of this study.

Prevalence of chronic airway obstruction and relative undiagnosed.
The primary characteristics of asymptomatic and symptomatic participants are respectively summarized in Tables 1 and 2. The results show that a greater percentage of asymptomatic than symptomatic participants had airway obstruction. The symptomatic participants were more likely to smoke than asymptomatic subjects.
Summary statistics and comparison of characteristics between genders in asymptomatic participants.
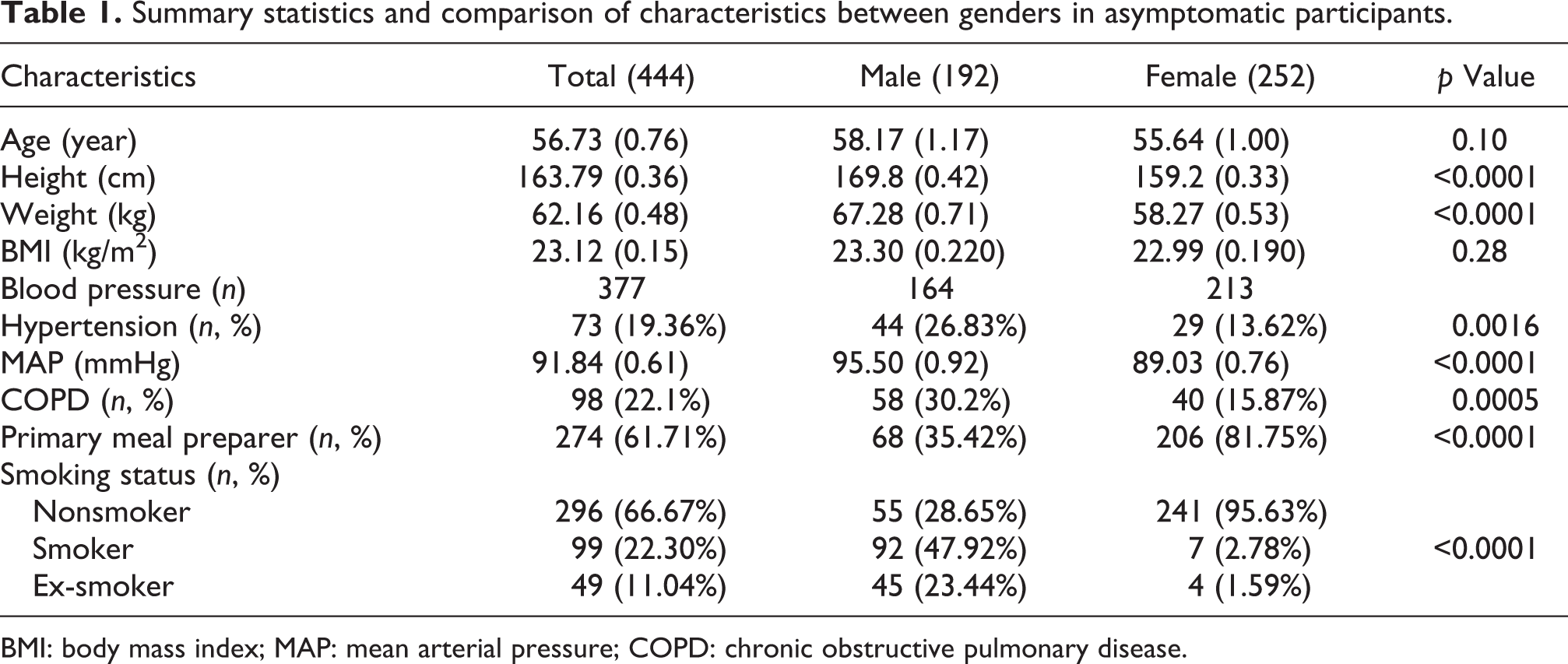
BMI: body mass index; MAP: mean arterial pressure; COPD: chronic obstructive pulmonary disease.
Summary statistics and comparison of characteristics between genders in symptomatic participants.

BMI: body mass index; MAP: mean arterial pressure; COPD: chronic obstructive pulmonary disease.
The variables between normal and asymptomatic COPD groups were compared to identify the risk factors. Table 3 presents age, gender, height, weight, body mass index (BMI), smoking status, primary meal preparer, and blood pressure between two groups. Significant differences in age (p = 0.004), gender (p = 0.0005), height (p = 0.0043), BMI (p = 0.02), smoking status (p < 0.0001), and systolic blood pressure (SBP; p = 0.019) were found between normal and asymptomatic COPD groups. However, significant difference in all other indices was not detected.
Summary statistics and comparison of characteristics between normal and asymptomatic COPD.

MAP: mean arterial pressure; BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; COPD: chronic obstructive pulmonary disease.
To further analyze the risky factors, asymptomatic COPD subjects were divided into the mild group and moderate or severe group according to lung function. The distributions of age, gender, BMI, height, weight, and SBP between two groups are shown in Table 4. Significant difference in gender (p = 0.004) between two groups was found. Difference in age, height, weight, BMI, SBP, and smoking status were not significant.
Summary statistics and comparison of characteristics between severities of COPD.
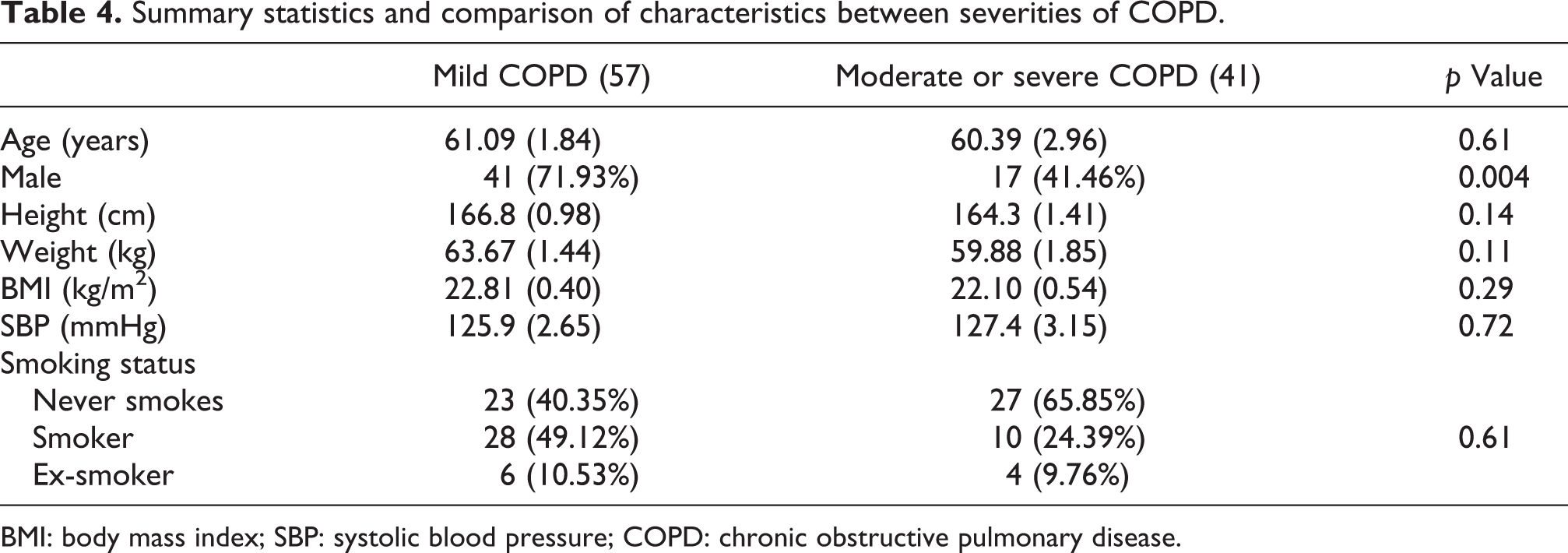
BMI: body mass index; SBP: systolic blood pressure; COPD: chronic obstructive pulmonary disease.
Logistic regression was used to determine associations with COPD. From Table 5, it is clear that only smoking status (odds ratio = 2.64, 95% confidence interval 1.20–6.04) was significantly associated with asymptomatic COPD. Age, gender, height, weight, BMI, and SBP were not significantly associated with airway obstruction.
Logistic regression of factors associated with asymptomatic COPD.

OR: odds ratio; CI: confidence interval; BMI: body mass index; SBP: systolic blood pressure; COPD: chronic obstructive pulmonary disease.
Discussion
Chronic obstructive lung disease is a substantial burden in China. Early detection and diagnosis may alter the course and prognosis. Our study demonstrated that 18.7% of adults who voluntarily participated in a public screening program in Xi’an had airway obstruction and over two-thirds (68.1%) of asymptomatic participants who had no airway obstruction were undiagnosed. Only smoking status was associated with asymptomatic COPD and more females than males had moderate or severe airway obstruction. Therefore, our findings suggest that simply using a voluntary public lung function screening program in China, and allowing participants to self-select, may be an effective approach to ensuring high yield detection of undiagnosed COPD.
Spirometry is a reliable, simple, noninvasive, safe, and inexpensive method for early detection and diagnosis of chronic respiratory disease, especially in asthma and COPD. Many studies 15 –18 in different countries have shown that underdiagnosis of COPD was substantial ranging from 5% to 60%. Our study showed 68.1% of participants had airway obstruction that was undiagnosed, suggesting the need for further follow-up. A greater percentage of asymptomatic than symptomatic participants had airway obstruction in our study. Symptomatic subjects are more prone to be detected at early stage. Thus, it is more important to screen the asymptomatic subjects earlier.
Cigarette smoke and air pollution are the two main causes of respiratory diseases in China. It is estimated that the prevalence of cigarette smoking was 60.2% among men and 6.9% among women in China. 19 This result is similar to our findings of 71.3% and 4.4%, respectively. Only smoking status was associated with impaired lung function in our study. Smoking harms airways with less than 2 mm internal diameter, 20 so it is significantly associated with airway obstruction. China is among the countries with the worst air quality. Researchers have also investigated the long-term effects of ambient air pollution on lung function with most finding adverse effects, such as accelerated decline of FVC, FEV1, and maximum midexpiratory flow. 9
Previous studies have suggested the emission from fuel sources could damage lung function. 21,22 However, our study failed to show an association between the primary meal preparer and COPD in this volunteer population. In addition, we found no significant relation between height, weight, BMI, SBP, and COPD.
More women than men had moderate or severe airway obstruction though a greater percentage of men than women were cigarette smokers in our study. Since 2000, the number of women dying from COPD has exceeded the number of men dying from the disease. 23 Some studies 24,25 have suggested that women are more susceptible than men to the effects of tobacco smoke. Asthma prevalence rates are higher in women than in men between the ages of puberty and menopause. 26,27 Menstrual cycle variations in pulmonary function and airway hyperresponsiveness have been well documented. 28,29 Females also appear to exhibit more severe airway hyperresponsiveness and more severe asthma than males. 30,31 Airway hyperresponsiveness is one of the main features of asthma and is also a major risk factor for accelerated lung function decline and hence the development of COPD. However, the precise mechanism is not yet clear and it should be further studied.
The high rate of undiagnosed airway obstruction in our population is likely to be multifactorial. Limited access to health care may result in a lower rate of previously diagnosed lung disease. Annual per capita government expenditure on health care in China in 2011 according to World Health Organization information statistics is US$237, which is only 1/20th of the United States. 32 It is likely that people who held some concern about their health status, particularly their breathing, were more inclined to participate in our voluntary testing. It is the opinion of these authors that such “self” selection may actually prove beneficial when considering the development of public screening programs in China for lung disease. Furthermore, it cannot be fully ruled out that some patients who self-reported not having lung disease, may have, at some time been diagnosed with lung disease, but refused to report it, or did not have a high enough health literacy to understand or remember their diagnosis. However, further studies are needed to address the actual prevalence of airway obstruction in Xi’an.
Conclusion
Voluntary public lung function screening programs in China are likely to identify a large number of undiagnosed asymptomatic people with COPD. Smoking status is associated with airway obstruction and more females than males had moderate or severe airway obstruction.
Footnotes
Acknowledgments
The authors express gratitude to the study participants and research personnel for their involvement in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by funds from the Education Department of Shaanxi Provincial Government (11JK0707).