
Abstract
Background
Although the postbronchodilator FEV1/FVC is the gold standard for diagnosing COPD, it is not easily obtainable due to various reasons. This study aims to investigate whether FEV1/FEV6 may serve as an easily accessible surrogate for FEV1/FVC in detecting airway obstruction and COPD.
Methods
Eligible articles were screened from PubMed, Web of Science and Scopus. The Quality Assessment of Diagnostic Accuracy Studies-2 was applied for quality assessment. The pooled sensitivity, specificity, and area under the curve (AUC) of the summary receiver operating curve were calculated to evaluate the diagnostic performance of FEV1/FEV6 in detecting airway obstruction and COPD and to determine the optimal cutoff value. Sensitivity analyses, subgroup analyses and meta-regression were performed to explore the source of heterogeneity.
Results
With 28 eligible articles and 65,744 subjects, the FEV1/FEV6 ratio showed good diagnostic performance in detecting both airway obstruction (sensitivity: 0.87, specificity: 0.94, AUC 0.95) and COPD (sensitivity: 0.83, specificity: 0.88, AUC 0.91). Further analyses of the optimal cutoff value suggested that an FEV1/FEV6<0.72 was the best criterion for detecting airway obstruction (sensitivity: 0.84, specificity: 0.97, AUC 0.96), whereas an FEV1/FEV6<0.74 was the best criterion for detecting COPD (sensitivity: 0.87, specificity: 0.89, AUC 0.93). The results of subgroup analyses and meta-regression suggested that study design and geographical location may affect the heterogeneity of both sensitivity and specificity in detecting airway obstruction and COPD.
Conclusion
The FEV1/FEV6 may serve as an easily accessible alternative in detecting airway obstruction and COPD. However, application of FEV1/FEV6 may also be constrained by availability and affordability of devices. Further studies are required to determine the best-suited population for FEV1/FEV6 application.
1. Introduction
Chronic obstructive pulmonary disease (COPD) is a heterogeneous lung condition characterized by non-fully reversible airflow obstruction and multiple respiratory symptoms, with a prevalence of 10.3% globally and 8.6% in China.1–3 COPD patients, especially those in low- and middle-income countries, are reported to have unmet needs for diagnostic approaches, such as low availability of standard spirometry and insufficient screening tools. 4 A national cross-sectional study suggested that only 2.6% of COPD patients were aware of their condition in China. 5 Further studies reported an underdiagnosis rate of over 70% in patients with COPD.6,7 As most of the COPD patients were of mild or moderate stage of the disease, underdiagnosis at the population level still exists due to subtle or absent symptoms of patients. 5 Implementing pre-symptomatic screening for airflow limitation and COPD may help address this gap.
Spirometry examination focusing on forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) is regarded as the gold standard for identifying airway obstruction (FEV1/FVC <0.7) and COPD (FEV1/FVC <0.7 post-bronchodilation). 1 However, application of spirometry also faces certain challenges. Since United States Preventive Services Task Force did not recommend routine COPD screening for the general asymptomatic population, there is a need for convenient tests to identify individuals with high risk of COPD. 8 Moreover, meeting quality control for FVC was relatively difficult, especially for older adults with greater risks of airway obstruction, which also calls for a metric less reliant on FVC to identify potential airway obstruction effectively.9,10
Forced expiratory volume in 6 seconds (FEV6) has been regarded as a potential alternative for FVC to address the current challenges of spirometry. 11 FEV6 has been shown to offer the following strengths: (1) With the widespread application of portable spirometry, measuring FEV6 via portable devices became possible, which may improve the convenience of this examination compared to traditional spirometry. 12 ; (2) FEV6 have been shown to exhibit good diagnostic performance. A meta-analysis in 2009 revealed that the FEV1/FEV6 is a valid alternative for the detection of airway obstruction compared with the FEV1/FVC. 13 However, there are also concerns over the efficacy of FEV1/FEV6, especially for patients with mild airway obstruction. 14 Moreover, the previous meta-analysis did not summarize the performance of FEV1/FEV6 in COPD. Therefore, as studies accumulated in the past 15 years, we conducted this meta-analysis to update the diagnostic accuracy of FEV1/FEV6 in detecting airway obstruction and COPD. Additionally, as the optimal cutoff value of FEV1/FEV6 remains unclear in previous meta-analysis, we also explored the best cutoff value for FEV1/FEV6 in detecting airway obstruction and COPD. The optimal cutoff value may be useful in the further standardization of FEV1/FEV6 in clinical practice.
2. Methods
This systematic review and meta-analysis was registered on the INPLASY website (INPLASY202470029) and performed following the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines. 15
2.1. Literature search
A literature search was conducted by two investigators independently in PubMed, Web of Science and Scopus from the inception of the databases to May 2024, and updated in December 2024 and December 2025, respectively. The details of the search strategies are presented in Table S1. References of related systematic reviews were also screened and selected to prevent omissions.
2.2. Inclusion and exclusion criteria
The inclusion criteria of this study were as follows: (1) Diagnostic tests reporting true positive (TP), true negative (TN), false positive (FP) and false negative (FN) results of FEV1/FEV6 in detecting airway obstruction compared with conventional spirometry. (2) Studies with a sample size of over 100. (3) Spirometry examination was performed for participants as the gold standard. Airway obstruction was defined as FEV1/FVC<0.7 or FEV1/FVC<lower limit of normal (LLN), regardless of bronchodilator usage; whereas COPD was defined as postbronchodilator FEV1/FVC<0.7 or FEV1/FVC<LLN. This study applied no restrictions regarding participants’ mean age or population source, with eligibility extended to both general and clinical populations. The exclusion criteria were as follows: (1) Duplicated data from the same database or institution, for which we included only the study with the largest population. 16 (2) Studies not published in English. (3) Review, meta-analysis, editorials, research letters, abstracts and comments. (4) Data from unpublished studies. Two authors independently screened all records and any disagreement was resolved by group discussion.
2.3. Data extraction and quality assessments
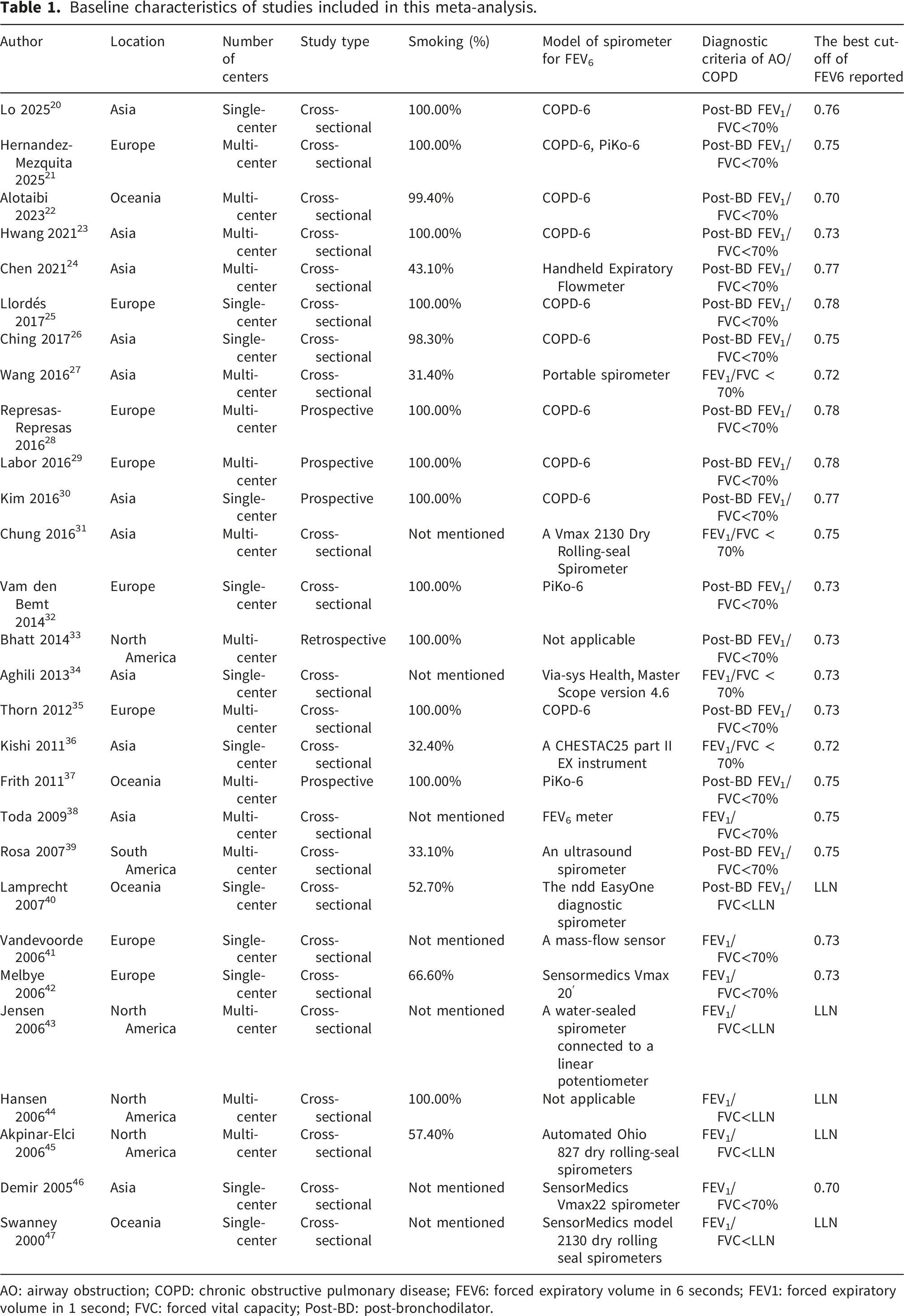
Two authors independently extracted and collected data from each study, and any disagreements were resolved by group discussion. Data extraction mainly focused on the baseline characteristics of eligible studies and the diagnostic performance of FEV1/FEV6. The baseline characteristics included the name of the first author, publication year, continent, number of centers, study direction (prospective or not), proportion of smokers, number of cases and controls, and diagnostic criteria for airway obstruction or COPD. Diagnostic performance included every cutoff value of FEV1/FEV6 along with their diagnostic performance.
To evaluate the quality of eligible diagnostic tests, the Quality Assessment of Diagnostic Accuracy Studies (QUADAS)-2 was applied, which evaluated the risk of bias via four aspects (patient selection, index test, reference standard and flow and timing) and assessed applicability concerns via three aspects (patient selection, index test and reference standard). 17 The Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) was applied to evaluate certainty of evidence (GRADEpro). 18
2.4. Statistical analysis
A meta-analysis of diagnostic accuracy was performed following the suggested guidelines. 19 The sensitivity, specificity, positive likelihood ratio (PLR), negative likelihood ratio (NLR) and diagnostic odds ratio (DOR) were calculated. Summary receiver operating characteristic (sROC) curve analysis was also performed to evaluate the overall diagnostic performance of FEV1/FEV6. We first performed a pooled analysis to identify the overall diagnostic performance of FEV1/FEV6 in identifying airway obstruction and COPD. If the diagnostic performance of more than one cutoff value was reported in the same study, the cutoff value with the best diagnostic performance reported in the study was selected for overall analysis. Then, we summarized studies reporting the diagnostic performance of the same cutoff values from FEV1/FEV6<0.70 to FEV1/FEV6<0.80 and conducted pooled analysis for every cutoff value reported by more than three studies, which may help to identify the best cutoff value of FEV1/FEV6 in identifying airway obstruction and COPD. The heterogeneity of the results was assessed via the I2 statistic and the Q test. A random-effect model was applied if significant heterogeneity was observed (I2>50% or p<0.05); otherwise, a fixed-effect model was applied. Sensitivity analyses were applied to evaluate the stability of results and identify potential outliers. Subgroup analyses and meta-regression were applied to evaluate the potential source of heterogeneity in categorial and continuous variables, respectively. In the subgroup analyses, we investigated whether study sample size, study design, study center, reference standard and geographical location were source of heterogeneity. In the meta-regression, we investigated whether age, smoking, sex, body mass index and spirometry results were source of heterogeneity. Deek’s funnel test was conducted to detect potential publication bias. All the statistical analyses were performed via Stata (Version 16.0) software, and a p value of <0.05 was considered to indicate statistical significance.
2.5. Patient and public involvement statement
Patients and public were not involved.
3. Results
3.1. Study screening and quality assessment
As shown in Figure 1, 2,599 records were identified during the literature search. After removing duplicate results and irrelevant records, 70 articles were selected for full-text screening, and 28 articles with 65,744 subjects (19,244 patients with airway obstruction and 46,500 without) were ultimately identified as eligible.20–47 The baseline characteristics of these eligible articles are shown in Table 1 andTable S2. Results of the quality assessment are shown in Figure S1, suggesting that all studies were of moderate to high quality. Moreover, the patient selection and index test of some studies may introduce risk of bias to study results. All eligible articles were shown to be of moderate to high quality. GRADE score suggested that certainty of evidence was moderate for FEV1/FEV6 in detecting airway obstruction, and low for detecting COPD (Figure S2-3). Flow chart of study selection. Baseline characteristics of studies included in this meta-analysis. AO: airway obstruction; COPD: chronic obstructive pulmonary disease; FEV6: forced expiratory volume in 6 seconds; FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity; Post-BD: post-bronchodilator.
3.2. Overall diagnostic performance of FEV1/FEV6
Among the 28 eligible articles reporting FEV1/FEV6 in airway obstruction, the sensitivity ranged from 0.71--0.97, and the specificity ranged from 0.67--1.00. The pooled sensitivity and specificity of the FEV1/FEV6 ratio reached 0.87 (95% CI 0.83, 0.90; I2=96.92%, p<0.01) and 0.94 (95% CI 0.90, 0.97; I2=98.49%, p<0.01), respectively (Figure 2(a) and Figure S4). The sROC curve suggested that the area under the curve (AUC) reached 0.95 (95% CI 0.92, 0.96) (Figure 2(A)). The PLR, NLR and DOR reached 15.6 (95% CI 8.9, 27.2), 0.14 (95% CI 0.11, 0.18) and 113.0 (95% CI 56.0, 227.0), respectively. Diagnostic accuracy of FEV1/FEV6 in detecting airway obstruction and COPD. (a): sROC curve of EFV1/FEV6 in detecting airway obstruction; (b): sROC curve of FEV1/FEV6 in detecting COPD. COPD: chronic obstructive pulmonary disease; sROC: summary receiver operating characteristic.
Sixteen articles reported the performance of FEV1/FEV6 in detecting COPD,20–26,28–30,32,33,35,37,39,40 with a sensitivity range of 0.71--0.93 and a specificity range of 0.67--0.99. The pooled sensitivity and specificity reached 0.83 (95% CI 0.79, 0.87; I2=97.10%, p<0.01) and 0.88 (95% CI 0.81, 0.93; I2=98.26%, p<0.01), respectively (Figure 2(B) and Figure S5). The sROC curve showed an AUC of 0.91 (95% CI 0.88, 0.93) (Figure 2(b)). The PLR, NLR, and DOR were 6.9 (95% CI 4.4, 10.9), 0.19 (95% CI 0.15, 0.25), and 36.0 (95% CI 20.0, 64.0), respectively.
3.3. Optimal cutoff value of FEV1/FEV6
Diagnostic accuracy of FEV1/FEV6 using different cut-off values in detecting airway obstruction.

NLR: Negative likelihood ratio; PLR: Positive likelihood ratio; DOR: diagnostic odds ratio.
The best cutoff value was presented in
Diagnostic accuracy of FEV1/FEV6 using different cut-off values in detecting COPD.
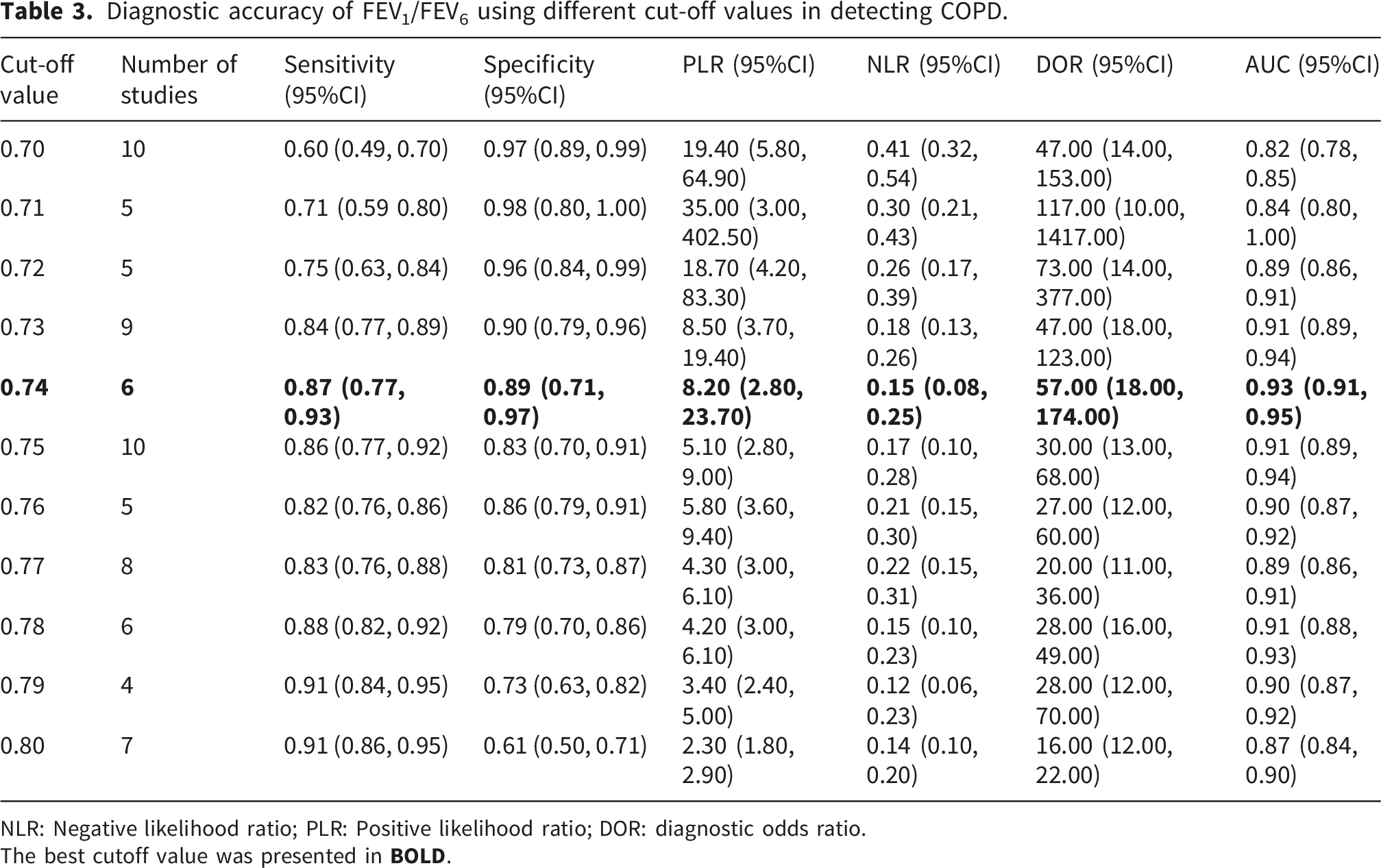
NLR: Negative likelihood ratio; PLR: Positive likelihood ratio; DOR: diagnostic odds ratio.
The best cutoff value was presented in
3.4. Sensitivity analyses, subgroup analyses and meta-regression
Subgroup analysis and meta-regression of categorial variables.

Significant results were shown in
Summary: Study design, reference standard and geographical location significantly affected the heterogeneity of FEV1/FEV6 for AO in terms of sensitivity and specificity. Study design and geographical location significantly affected the heterogeneity of FEV1/FEV6 for COPD in terms of sensitivity and specificity.
Meta-regression of continuous variables.

COPD: chronic obstructive pulmonary disease; BMI: body mass index; FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity.
Summary: Smoking rate affected the heterogeneity of airway obstruction and COPD in terms of specificity, and FEV1% affected the heterogeneity of COPD in terms of sensitivity.
3.5. Publication bias
The results of Deek’s funnel plot asymmetry tests were shown in Figures S23-24. Although no publication bias was observed in studies for airway obstruction (p=0.10), significant publication bias was observed in studies for COPD (p<0.01).
4. Discussion
With a total of 28 article sources, this systematic review and meta-analysis suggested that the FEV1/FEV6, achieved by a simple handheld device, has good diagnostic performance in detecting both airway obstruction and COPD with different optimal cutoff value. Compared with FEV1/FVC, FEV1/FEV6 was more easily-available for general population, and more technically acceptable for patients with severe COPD, which may serve as a more available surrogate in primary screening.
Selecting an appropriate cutoff value for FEV1/FEV6 is also important for optimizing its diagnostic performance. Conventional spirometry examination uses an FEV1/FVC<0.7 as the gold standard for airway obstruction. 48 As the value of FEV6 was lower than that of FVC, the cutoff value should be increased to reach a similar diagnostic performance to the gold standard. Currently, multiple cutoff values have been used in studies on FEV1/FEV6, each with its own advantages and disadvantages. However, the optimal cutoff value of FEV1/FEV6 requires further investigation. The results of this meta-analysis suggested that an FEV1/FEV6<0.72 reached the best diagnostic performance in detecting airway obstruction, whereas an FEV1/FEV6<0.74 reached the best performance in detecting COPD. The possible reasons for the different optimal cutoff values may be that patients with bronchodilator-confirmed COPD were associated with larger proportion of expiratory volumes after the first 6 seconds, the effects of which should be adjusted by a larger cutoff value. For some participants with airway obstruction, their obstruction may be mild and reversible, which was less affected by this effect. Moreover, according to the standardization guideline of spirometry, expiration should continue until an expiratory plateau is reached, or if not achievable, should be reproducible and maintained for at least 15 seconds.21,49 In patients with severe airway obstruction, expiration often continues for 15 seconds. Compared with FEV6, the expiratory volume from the 9 more seconds was large enough to affect the diagnosis of airway obstruction, suggesting that performance of FEV1/FEV6 may also depend on the severity of diseases.21,49
Additionally, although the FEV1/FEV6 ratio has good diagnostic performance in detecting airway obstruction and COPD, the significant heterogeneity of these results cannot be ignored. The results of subgroup analyses and meta-regression suggested that study design (prospective or retrospective) and geographical location (European and non-European) were sources of heterogeneity affecting both sensitivity and specificity. As retrospective studies may increase the risk of potential bias while the number of prospective studies is relatively small, more prospective studies are needed to verify the results. 50 For studies conducted in different geographical locations, factors such as different races, clinician proficiencies and types of equipment may contribute to heterogeneous results. 51 FEV1% was also a potential source of heterogeneity according to the results of the meta-regression, which may imply that the severity of COPD may also affect the diagnostic performance of FEV1/FEV6. Moreover, the studies included were published from 2000--2025 and were performed with diverse clinician proficiencies, which may also serve as a potential reason for significant heterogeneity. 52
COPD screening approaches primarily target high-risk populations, particularly current/former smokers and individuals with occupational exposures. For potential approaches for COPD screening, the diagnostic performance of COPD screening questionnaires has also been reported in many studies. A meta-analysis reported that the COPD screening tool questionnaire reached a sensitivity of 0.66 and a specificity of 0.86 in detecting COPD patients in the general population. 53 A study in a Chinese population suggested that the Lung Function Questionnaire, with an AUC value of 0.785, was superior to five other COPD screening questionnaires in the Chinese population. 54 These studies suggested that despite being simple and easily accessible, these questionnaires were not sufficient to identify potential COPD patients accurately. Therefore, further studies should focus on a combination of screening questionnaires and portable spirometry to maximize diagnostic accuracy. A comparative study suggested that a combination of a COPD screening questionnaire and peak flow meter screening may become the optimal screening tool for COPD. 55 A further simulation modeling study revealed that the application of both portable spirometry and COPD screening questionnaires was cost effective and beneficial for improving population health outcomes. 56 Compared with previous studies, this meta-analysis suggested that FEV1/FEV6, also achieved by portable spirometry, can also be considered an alternative to portable spirometry in primary care settings, thereby reducing the burden of COPD in the long term. If the initial screening yields positive results, patients will be referred for standard pulmonary function tests to verify COPD presence. However, although the above approaches may identify patients suspicious of COPD in their early stage, they are also restricted by multiple factors including suboptimal efficacy and quality control.
This study has the following strengths. With a relatively large number of eligible studies and rigorous investigations of the optimal cutoff value, results of this meta-analysis became more robust. The application of sensitivity analyses, subgroup analyses and meta-regression were also helpful for investigation of heterogeneity. The limitations of this meta-analysis should also be discussed. (1) Significant heterogeneity was observed in our results, which can be only partly explained by subgroup analyses and meta-regression. (2) Publication bias was observed in studies reporting the diagnostic performance of FEV1/FEV6 in detecting COPD. These limitations may increase the risk of potential bias and affect the reliability of the study results. (3) Application of portable devices of FEV1/FEV6 may still be constrained by issues of accessibility and affordability, and diagnostic performance of FEV1/FEV6 necessitates further evaluation in future studies. (4) Only studies in English were enrolled in this meta-analysis, which may increase the risk of missing relevant non-English studies. (5) Although eligible studies were of moderate to high quality in this meta-analysis, some studies still have concerns over the aspects of patient selection and index test, which may increase the risk of bias. (6) Lastly, portable screeners for FEV1/FEV6 does not replace spirometry as you are unable to measure the quality of the patient effort and flow curves. Conventional spirometry for FEV1/FVC is still the cornerstone of COPD diagnosis.
There are also some issues that worth further investigations. First of all, the performance of FEV1/FEV6 in specific groups of population, such as African, Hispanics or people in the high-risk occupations, was still unknown. Moreover, whether FEV1/FEV6 exhibit similar performance among patients with varying degrees of respiratory symptoms remained inadequately understood. Additionally, can we improve the performance of FEV1/FEV6 by combining it with other self-reported screening questionnaire? Further studies of FEV1/FEV6 are still needed to address this issue.
5. Conclusion
The FEV1/FEV6 may serve as an easily achieved surrogate for detecting airway obstruction and COPD, with the best cutoff values of 0.72 and 0.74, respectively. The above findings have provided additional evidence of the robustness of FEV1/FEV6 as a valuable indicator of respiratory health, which may become a strong addition to be applied in the primary care settings. However, application of FEV1/FEV6 was still constrained by multiple factors, and its diagnostic performance warranted further evaluation.
Supplemental material
Supplemental Material - Diagnostic performance of FEV1/FEV6 in detecting airway obstruction and chronic obstructive pulmonary disease: A systematic review and meta-analysis
Supplemental Material for Diagnostic performance of FEV1/FEV6 in detecting airway obstruction and chronic obstructive pulmonary disease: A systematic review and meta-analysis by Dongru Du, Sike He, Jiangyue Qin, Hao Wang, Lijuan Gao, Mei Chen, Xiaohua Li, Zhenni Chen, Fengming Luo, Yongchun Shen in Chronic Respiratory Disease.
Supplemental material
Supplemental Material - Diagnostic performance of FEV1/FEV6 in detecting airway obstruction and chronic obstructive pulmonary disease: A systematic review and meta-analysis
Supplemental Material for Diagnostic performance of FEV1/FEV6 in detecting airway obstruction and chronic obstructive pulmonary disease: A systematic review and meta-analysis by Dongru Du, Sike He, Jiangyue Qin, Hao Wang, Lijuan Gao, Mei Chen, Xiaohua Li, Zhenni Chen, Fengming Luo, Yongchun Shen in Chronic Respiratory Disease.
Footnotes
Acknowledgements
In 2009, Dr. Huahao Shen and his colleagues published a meta-analysis to summarize the diagnostic value of FEV1/FEV6 in detecting airway obstruction. This is an updated meta-analysis based on Dr Shen’s achievement, and is also a memory for Dr. Huahao Shen, who passed away on April 2024.
Consent for publication
All authors have reviewed the current version of this manuscript and agreed for publication.
Author’s contributions
DD, SH and JQ: Conceptualization, Methodology, Software, Formal analysis and Writing - original draft. HW and LJ: Data curation and Software. MC, XL and ZC: Methodology and Software. FL and YS: Conceptualization, Funding acquisition, Resources, Supervision and Writing - review & editing. DD, SH and JQ contributed equally to this work. YS is the guarantor of this work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (W2511097, 82170046, 82470062, and 82300050) and the Sichuan Key Research and Development Program (2024NSFSC1522 and 2024YFFK0279). These funding agencies were not involved in designing the study, collecting or analyzing the data, writing the manuscript, or making decisions related to publication.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data in this work were available from the corresponding authors with reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.