
Abstract
Sexual dysfunction is a common problem in chronic obstructive pulmonary disease (COPD). We aimed to assess the presence of erectile dysfunction (ED) in COPD patients. Ninety-three outpatients who had been diagnosed as COPD and followed in Bolvadin State Hospital, Afyon, Turkey, were included in the study. All patients underwent pulmonary function tests and arterial blood gas analysis. They completed International Physical Activity Questionnaire (IPAQ), Medical Research Council (MRC) Dyspnea Scale, Short Form 36-item Scale (SF-36), and International Index of Erectile Function (IIEF) Questionnaire. The mean age of 10 (10.8%) mild, 46 (49.5%) moderate, 28 (30.1%) severe, and 9 (9.7%) very severe COPD patients was 61.4 ± 9.8 years. Varying degrees of ED were detected in 67.7% of COPD patients. All patients with hypoxemia had ED. IPAQ score and all SF-36 parameters were low in patients with ED, while MRC score was high. Forced expiratory volume in one second, forced vital capacity, partial pressure of oxygen in blood, oxygen (O2) saturation, IPAQ score, and role-physical parameters were statistically low in ED patients (p = 0.04, 0.02, <0.01, <0.01, 0.02, and 0.04, respectively); MRC score was statistically higher in patients with ED (p = 0.02). Patients with moderate and severe ED had statistically lower score of mental health (p < 0.01 and p = 0.02, respectively). There was a positive correlation between IIEF score and IPAQ scores (p < 0.01), MRC scores (p = 0.01), general health (p < 0.01), role-physical (p < 0.01), role-emotional (p < 0.01), physical functioning (p < 0.01), and mental health (p < 0.01) parameters in SF-36. ED is frequently seen in COPD patients. Hypoxemia, smoking, and limitation of physical activity are thought to be associated with ED in COPD as mechanisms. Quality of life and the functional capacity are negatively affected with the presence of ED. It is important for a physician to question the sexual functions in patients with COPD. The presence of ED may be routinely considered in the daily practice of pulmonologists in COPD patients.
Introductıon
Since chronic obstructive pulmonary disease (COPD) is a chronic disease of middle-aged or older people, comorbidities are frequently seen. With decreasing sexual interest, testosterone levels and sexual function by aging, and the presence of chronic illnesses, erectile dysfunction (ED) is one of these comorbid diseases.
ED is a frequent type of sexual dysfunction among mature and aging men, which is characterized by the inability to have an erection during sexual activity. A broad-based public study (Massachusetts Male Aging Study) revealed an ED prevalence as high as 52% in males between the fourth and seventh decade of life. 1 Dunn et al. demonstrated that 34% of males (mean age 50) within the general population complained about sexual problems and the most common complaint was ED. 2 Both studies showed that ED prevalence increases with age.
The mechanism of ED is not exactly clarified in COPD, but there are some potential risk factors. Decreased functional capacity due to hypoxemia is specified to be the main reason for ED. 3 Chronic systemic inflamation, decrease in testesterone level, aging, psychosocial problems, and decrease of physical activity are seemed to be other risks for ED in COPD. 4
The quality of life (QoL) generally diminishes in COPD as the disease progresses. 5 Besides, ED is also another reason for the decrease in QoL of both the male and the female partners. Sexual dysfunction also affects the QoL negatively in COPD patients. 6
There are only a few studies about prevalence of ED in patients with COPD until now. These studies reported higher rate of ED in COPD patients compared with normal population. 4,7
We have undertaken a study to examine the presence of ED in COPD patients and relationship between ED and characteristics of COPD.
Materials and methods
Ninety-three outpatients who had been diagnosed with COPD, according to Global Initiative for Chronic Lung Disease criteria, 8 and followed in Bolvadin State Hospital, Afyon, Turkey, were included in the study between June and December 2012. Permission was taken from the ethics comitee of the institution. Written informed consent was obtained from all of the patients.
The patients with the diagnosis of a pulmonary pathology other than COPD, diabetes mellitus, malignancy COPD exacerbations within past 3 months and low mental status were excluded.
Medical history of the patients was taken. Demographics, clinical symptoms, the history of smoking habit (as pack-years), and comorbidities were recorded. The time of the diagnosis of COPD was learnt and recorded from database of the hospital.
Pulmonary assessment included pulmonary function tests and arterial blood gas analysis. All patients underwent standard spirometry, and forced expiratory volume in 1 second (FEV1), forced vital capacity (FVC), and FEV1/FVC were determined with spirometry (spirolab III S/N A23-053, Rome, Italy). The stages of COPD were determined as mild (FEV1 >80%), moderate (FEV1 50–80%), severe (FEV1 30–50%), and very severe (FEV1 <30%), according to Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria. 8 Arterial blood gas analysis, which was obtained from the radial artery, was performed at rest and in a sitting position.
The patients completed Short Form 36-item (SF-36) Questionnaire Scale, International Physical Activity Questionnaire (IPAQ), Medical Research Council (MRC) Dyspnea Scale, and International Index of Erectile Function (IIEF) Questionnaire.
The SF-36 is an instrument for measuring health-related QoL in patients with COPD. 9,10 The SF-36 evaluates QoL related to physical and mental health with questions ranging from 0 to 100 points. It is a useful survey to use in clinical practice and investigations about COPD, which has also been used for the assessment of sexual health in previous studies. 11
Measurement of physical activity was done using the IPAQ, which shows the level of physical activity. 12 Participants were asked to report the total minutes over the last 7 days spent on moderate and vigorous-intensity physical activity, walking physical activity, and inactivity. The following values continued to be used for the analysis of IPAQ data: walking = 3.3 metabolic equivalents (METs), moderate physical activity = 4.0 METs, vigorous physical activity = 8.0 METs, and total physical activity MET (minutes/week) = sum of walking + moderate + vigorous MET (minutes/week) scores.
MRC Dyspnea Scale assesses whether there is any limitation in walking considered with a normal person.The questionnaire consists of six questions about breathlessness (see Appendix 1).
Erectile function and severity of ED were assessed according to National Institutes of Health criteria with IIEF Questionnaire, which is widely used in epidemiologic and clinical studies. 13 The questions about erection confidence, erection firmness, maintenance ability, maintenance frequency, and satisfaction form the IIEF Questionnaire. Each item is scored on a five-point scale; low score represents poorer sexual status and higher scores indicate better sexual function. ED status was classified into four categories as none (IIEF-5 score 22–25), mild (17–21), moderate (12–16), and severe (5–11). IIEF scores were calculated and reported by a scale of 5–25. The questions 11 and 12 of IIEF, which are indicating the sexual desire, were evaluated seperately. The IIEF questionnaire was validated in the Turkish language. 14
In addition to data obtained from IIEF, patients were evaluated with hormone levels, which can have an influence on erectile function. Blood serum levels of testosterone, free testosterone, luteinizing hormone, follicle stimulating hormone, estradiol, and prolactin were measured in early morning between 8 a.m. and 10 a.m. Patients with any imbalance in these hormones were excluded from the study. All patients were physically examined and patients with any urogenital abnormality were excluded as well. Patients without a chance to have a regular sexual relationship were not included in the study.
Statistical analyses were performed with SPSS® version 13.0. The nonparametric Kruskal–Wallis test was applied for multiple comparisons when Mann–Whitney U test was used for comparison between groups. The Pearson correlation was used to investigate the relationship between sexual function and parameters of COPD. Multivariate analysis of variance was also performed between all variables.
Results
A total of 93 COPD patients had a mean age of 61.4 ± 9.8, varying between 36 and 84. Patient demographics are shown in Table 1.
Demographics and characteristics of COPD.
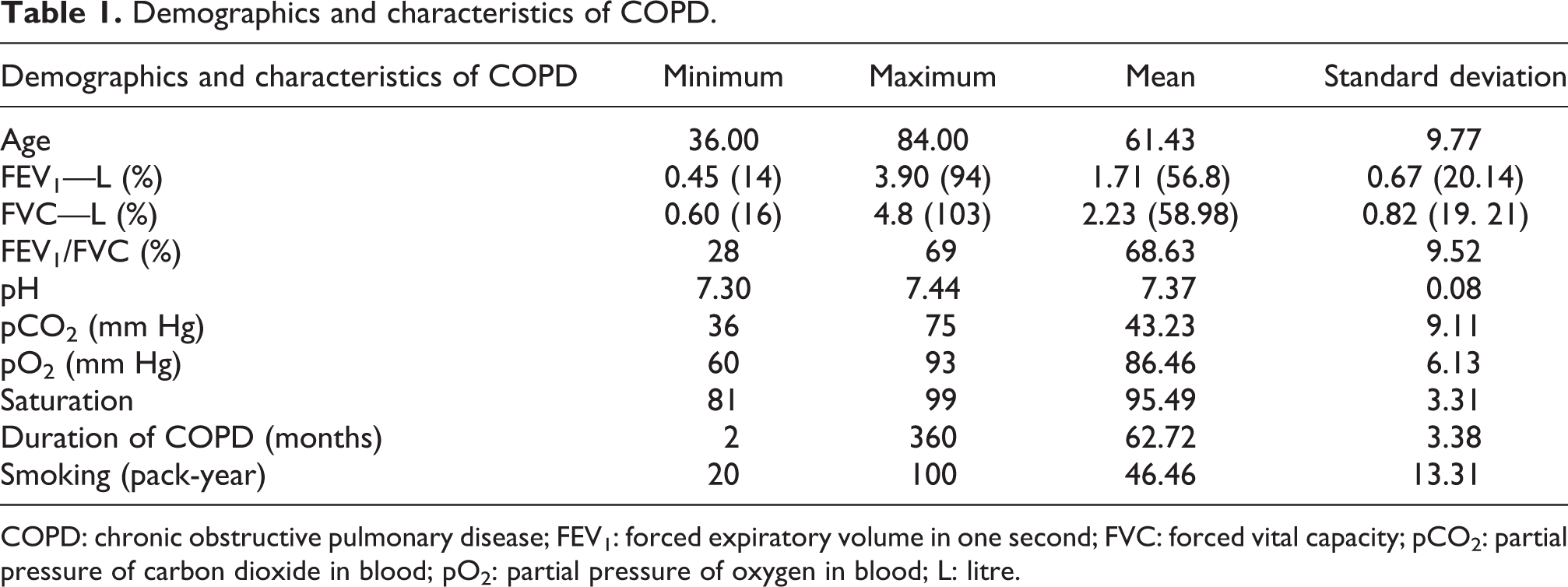
COPD: chronic obstructive pulmonary disease; FEV1: forced expiratory volume in one second; FVC: forced vital capacity; pCO2: partial pressure of carbon dioxide in blood; pO2: partial pressure of oxygen in blood; L: litre.
All the patients had been a current smoker or an ex-smoker. Forty-three (46.2%) patients were still smoking, while 50 (53.8%) participants had quit smoking. There were 37 (39.8%) patients who had at least one comorbidity. Hypertension (16%–17.2%) and coronary artery disease (13%–13.9%) were the most common comorbidities.
The mean duration of COPD was found as 56.8 ± 7.9 months in all patients. There were 10 (10.8%) mild, 46(49.5%) moderate, 28 (30.1%) severe, and 9 (9.7%) very severe patients according to GOLD criteria. 6 The mean FEV1 value of patients was 1.71 ± 0.67 (56.88 ± 20.14%), FVC was 2.23 ± 0.83 (58.98 ± 19.21%), and FEV1/FVC was 68.65 ± 9.47%. Partial pressure of O2 in blood (PaO2) was 86.46 ± 6.13 and partial pressure of carbon dioxide in blood was 43.23 ± 9.11 mm Hg. Pulmonary function test and arterial blood gas parameters are shown in Table 1.
Varying degrees of ED were detected in 63 (67.7%) COPD patients. According to IIEF, 11 there were 22 (34.9%) mild, 15 (23.8%) moderate, and 26 (41.3%) severe type of ED (Table 2). Mean ED score for IIEF was found to be 17.5 ± 9.4. There was ED in 88.9% of very severe COPD patients. There was no relationship between the stage of COPD and the presence of ED (p = 0.47). The rate of sexual desire was 59.1% in our study.
ED status in COPD patients.

COPD: chronic obstructive pulmonary disease; ED: erectile dysfunction.
Correlation analysis of scores of IIEF is shown in Table 3. IIEF score was negatively correlated with pack-years of cigarette smoking and age. There was a positive correlation between IIEF score and PaO2, IPAQ and MRC scores, general health, role-physical, role-emotional, physical functioning, and mental health parameters in SF-36.
Correlation analysis of IIEF scores in parameters of COPD patients.

COPD: chronic obstructive pulmonary disease; IIEF: International Index of Erectile Function; FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity; pCO2: partial pressure of carbon dioxide in blood; pO2: partial pressure of oxygen in blood; IPAQ: International Physical Activity Questionnaire; MRC: Medical Research Council; L: litre.
ap < 0.05: statistically different between groups.
IPAQ score and all SF-36 parameters were found to be low in patients with ED, while MRC score was high. FEV1, FVC, PaO2, O2 saturation, IPAQ score, and role-physical parameters were statistically low in ED patients (p = 0.04, 0.02, <0.01, <0.01, 0.02, and 0.04, respectively); MRC score was statistically higher in patients with ED (p = 0.02; Table 4). Patients with moderate and severe ED had statistically lower score of mental health (p < 0.01 and p = 0.02, respectively).
The mean values of parameters in COPD according to the presence of ED.

COPD: chronic obstructive pulmonary disease; FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity; ED: erectile dysfunction; pO2: partial pressure of oxygen in blood; IPAQ: International Physical Activity Questionnaire; MRC: Medical Research Council; L: litre.
ap < 0.05: statistically different between groups.
There was statistical significant difference between means of differences of MRC, IPAQ, and some SF-36 parameters (physical functioning, general health, and mental health) according to status and stage of ED (Table 5). The means of IPAQ and SF-36 parameters were increasing from the group of no ED to severe ED when it was opposite at MRC scores.
Multivariate analysis of variance comparing means of UFAA, MRC, and SF-36 parameters according to the presence and stages of ED.

ED: erectile dysfunction; MRC: Medical Research Council; SF-36: Short Form 36-item Questionnaire Scale; UFAA: Uluslararası Fiziksel Aktivite Anketi.
ap < 0.05: statistically different between groups.
Discussion
Sexuality is a lifelong necessity in order to pursue human well-being. 4 Factors including aging and generally poor health can cause diminished sexual activity, libido, and ED. Male sexual dysfunction, including ED, diminished libido, and abnormal ejaculation becomes a common problem for men over 50 affecting approximately one-third of male population. 15 Physical and psychological problems, leading to morbidity, and medications can affect the sexual life of the patients.
ED is a common and multifactorial disorder with prevalence approximately between 5% and 20%, 16 which may vary according to age, up to 30%–50%. 1,2 ED is known to be more frequent with the presence of diseases, increasing its morbidity. COPD is one of these diseases, which seems to be a predictor of ED mostly in older patients. The prevalence of ED in COPD patients was found to be 67.7% in our study, which is similar with other studies. 3,4 This high prevalence of ED in COPD makes it an important and unignorable problem for COPD patients.
Unfortunately, sexual dysfunction is not generally questioned by physicians. On the other hand, one study showed that COPD patients did not commonly share their sexual problems with their physicians. 15 It was reported that the physicians usually focused on bronchospasm, respiratory failure, and infections in COPD patients; sexual problems have recieved less attention. 17
The main cause and mechanism of ED in COPD are still unclear. Hypoxemia is reported as an important factor for ED in some studies.
18
The reduction in nitric oxide (NO) synthase activity with increasing vasoconstruction
19
and the presence of dyspnea were found as main reasons of sexual dysfunction in COPD due to hypoxemia. Erections are hemodynamic events caused by penile arteries dilatation and smooth muscle fiber relaxation, which are the results of neurological, neurochemical, and endocrine mechanisms. The relaxation of corpus cavernosum smooth muscles is due to a nonadrenergic–noncholinergic nervous system mediated by NO. NO is a gas that diffuses into target tissues, where it activates guanylate cyclase and catalyzes the formation of cyclic guanosine-3′,5′-monophosphate (cGMP) from guanosine-5′-triphosphate. cGMP initiates a cascade of intracellular events and reduces intracellular calcium, which leads to relaxation of penis smooth muscles.
20
NO synthesis is mediated by NO synthetase, which requires both
Low functional capacity has also been thought to be associated with ED in COPD. Fletcher and Martin specified that decreasing functional capacity is posivitely correlated with sexual dysfunctions. 21 Köseoğlu et al. reported that ED severity increased with increasing COPD severity representing low functional capacity. 3 Our results revealed a low functional capacity in ED patients. Besides, we determined ED in 89% of very severe COPD patients. These results show the importance of examining sexual dysfunction in male COPD patients, especially in the very severe COPD subgroup.
Another risk factor for ED in COPD is found to be smoking. Our study demonstrated a negative correlation between the IIEF score and smoking amount (pack-year). Smoking was found to be an independent correlation for ED in COPD. 22 Thus, smoking cessation may reduce the chance of developing ED.
Our study revealed a positive correlation between IIEF score and MRC scores. Many COPD patients can avoid sexual activity because of the dyspnea associated with this activity. 23 Sexual dysfunction in COPD generally coincides with the progression of pulmonary symptoms. 20 It is thought that the presence of dyspnea, which is also associated with the limitation in physical activity, may also be related with the lack of sexual activity.
Physical activity is known to be a predictor factor for normal erectile function. Many studies demonstrated that physical activity decreased the risk of ED and improved sexual functions among those with established ED. 24,25 Maio et al. showed that physical activity was the only independent variable for normal erection and higher sexual satisfaction. 26 Reduced physical activity is frequently seen in patients with COPD. 27 Our results revealed a positive correlation between IIEF score and IPAQ score, which means that the limitation of physical activity may also diminish the sexual activities in COPD patients.
All SF-36 domains were found to be low in patients with ED in our study. COPD patients are confronted with reduced QoL generally caused by dyspnea and systemic effects such as skeletal muscle dysfunction and comorbidities. 28 The strong association between sexual dysfunction and impaired QoL makes ED a major QoL issue. 29 Sexual dysfunctions, including ED, were also found to impact negatively the QoL of those with COPD in studies. 6 As ED is an important parameter that can affect QoL, it is important to question about sexual functions in COPD patients, which may help us to predict the QoL.
Our study showed a high prevalence of ED in COPD. Since sexual dysfunctions are generally neglected in COPD patients, it is so important to ask about impotance in patients with COPD.
Conclusion
Sexual dysfunction is a common problem in COPD patients. Hypoxemia, smoking, and the limitation of physical activity are thought to be the mechanisms associated with ED in COPD. The presence of ED negatively affects the functional capacity and QoL in COPD.
It is important for a physician to question the sexual functions in patients with COPD. Smoking cessation, increased physical activities, and prevention of hypoxemia may help sexual functions. The presence of ED may be routinely considered in the daily practice of pulmonologists in COPD patients.
Footnotes
Appendix 1
MRC Scale
30
0: no dyspnea; 1: slight dyspnea (shortness of breath when hurrying on the level or walking up a slight hill); 2: moderate dyspnea (walks slower than people of the same age on the level because of breathlessness); 3: moderately severe dyspnea (stops because of breathlessness when walking at own pace on the level); 4: severe dyspnea (stops for breath after walking about 100 yards or after a few minutes on the level); 5: very severe dyspnea (too breathless to leave the house or breathless when dressing or undressing).
Authors’ Note
Authors OT and IU contributed to literature search, data collection, study design, data analysis, manuscript preparation, and manuscript review and PAT contributed to manuscript preparation and manuscript review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.