
Abstract
Pulmonary rehabilitation (PR) can improve aerobic exercise capacity, health-related quality of life and dyspnoea in patients with chronic obstructive pulmonary disease (COPD). Recent studies have suggested that exercise training may improve blood pressure and arterial stiffness, albeit in small highly selected cohorts. The aim of the study was to establish whether supervised outpatient or unsupervised home PR can reduce peripheral blood pressure. Resting blood pressure was measured in 418 patients with COPD before and after outpatient PR, supervised by a hospital-based team (HOSP). Seventy-four patients with COPD undergoing an unsupervised home-based programme acted as a comparator group (HOME). Despite significant improvements in mean (95% confidence interval) exercise capacity in the HOSP group (56 (50–60) m, p < 0.001) and HOME group (30 (17–42) m, p < 0.001) systolic blood pressure (SBP), diastolic blood pressure (DBP) and mean arterial blood pressure (MAP) did not change in either the HOSP (SBP: p = 0.47; DBP: p = 0.06; MAP: p = 0.38) or HOME group (SBP: p = 0.67; DBP: p = 0.38; MAP: p = 0.76). Planned subgroup analysis of HOSP patients with known hypertension and/or cardiovascular disease showed no impact of PR upon blood pressure. PR is unlikely to reduce blood pressure, and by implication, makes a mechanism of action in which arterial stiffness is reduced, less likely.
Keywords
Introduction
Pulmonary rehabilitation (PR) has multiple benefits for patients with chronic obstructive pulmonary disease (COPD), including improvements in aerobic exercise capacity, health-related quality of life and dyspnoea. 1 Cardiovascular comorbidity is common in COPD 2 and a potential benefit of PR is the reduction of cardiovascular risk. This is supported by data demonstrating the benefits of exercise training on arterial stiffness and blood pressure in different populations, including those with coronary artery disease. 3 In patients with COPD, there has been conflicting data with some reporting a reduction in pulse wave velocity (PWV; as a surrogate marker of arterial stiffness) and blood pressure with exercise training, 4,5 albeit in small highly selective cohorts, whilst Vanfleteren and colleagues 6 demonstrated no changes in aortic PWV or centrally and peripherally measured blood pressure in those completing a forty-session rehabilitation programme. However these studies were limited by small sample numbers 4,5 or the absence of a comparator group. 6 Furthermore, it is not known whether there is a dose–response effect (i.e. the impact of exercise training on blood pressure is determined by the intensity and volume of training).
The aim of the current study was to determine whether 8 weeks of ‘real world’ supervised outpatient PR can modify blood pressure in patients with COPD. We further hypothesized that the decrease in peripherally measured blood pressure would be significantly more after outpatient PR, supervised by a hospital-based team (HOSP) compared with unsupervised home-based rehabilitation (HOME).
Materials and methods
The study was approved by the local research ethics committee (London–Camberwell St Giles 11/LO/1780). Inclusion criteria included age over 35, a diagnosis of COPD, 7 capability of walking 5 m independently and a Medical Research Council dyspnoea score of 2 or above. 8 Exclusion criteria included unstable cardiac condition that precluded from safe exercise. Unlike previous studies, this was a ‘real-world cohort and patients with ischaemic heart disease, cardiac failure, diabetes mellitus, malignancy, inflammatory or metabolic conditions, those using oral corticosteroids, or disease modifying medications 4,5 were not excluded.
Participants were recruited from assessment clinics at Harefield Hospital, Middlesex, UK. The active intervention was an outpatient multi-disciplinary PR programme that was supervised by a HOSP team. The programme comprised two supervised exercise/education sessions per week for 8 weeks, in line with the British Thoracic Society (BTS) PR guidelines. 1 Each session lasted for 2 hours, and 16 sessions were offered to each participant. Aerobic exercise intensity was set at 60–80% of peak oxygen consumption (VO2 peak) estimated from the initial incremental shuttle walk (ISW) and increased according to attainment of ‘moderate’ to ‘somewhat severe’ breathlessness (3–4) on the Borg breathlessness scale. 9 Resistance training involved individualized weight selection and all major muscle groups and consisted of 2–4 sets of 10–15 repetitions per exercise, with progression occurring when all sets with the selected weight were completed.
The comparator group (HOME) was recruited from respiratory clinics and comprised of patients with COPD who declined outpatient PR due to transport issues or work/family commitments. All underwent an initial 1 hour assessment with a specialist respiratory physiotherapist demonstrating home-based exercises, and then given an individualized, written home exercise programme, supplemented by weekly telephone calls. Further details of the home exercise programme are available in the online Supplement (S1).
Measurements
Peripheral blood pressure was measured at rest (after patients were seated for at least 15 minutes) in accordance with the British Hypertension Society and National Institute for Health and Care Excellence guideline using an approved Omron 7051T monitor. 10,11 Other outcome measurements (performed after blood pressure measurement) included spirometry according to BTS/American Thoracic Society guidelines, 12 the ISW, 13 assessment of 4-m gait speed 14,15 and the self-reported version of the chronic respiratory questionnaire. 16 All outcome measures were repeated after 8 weeks of PR at the end of course assessment.
Statistical analysis
Baseline comparisons between the HOSP and HOME groups were made using unpaired t tests or for non-normally distributed data, Mann-Whitney tests. Pre- and post-rehabilitation data for the HOSP and HOME groups were analysed using paired t tests or for non-normally distributed data, Wilcoxon signed rank tests. Comparison of the response to PR between the HOSP and HOME groups was analysed using unpaired t tests. Planned subgroup analyses included patients with co-existing hypertension and/or cardiovascular disease (n = 128), and those who improved their ISW by more than the established minimum clinically important difference (MCID). 17 To further investigate the impact of baseline patient characteristics on the response of blood pressure to PR, backwards stepwise linear regression analysis for the HOSP group was performed taking into account forced expiratory volume in 1 second percent predicted, age, weight, body mass index, systolic blood pressure (SBP), antihypertensive medications, anti-lipid medications, and known diagnosis of cardiovascular disease or hypertension.
Chi squared or Fishers’ exact tests were used to determined differences in proportions of baseline characteristics between the groups. Some of these data have been published in abstract form. 18 Data are presented as mean (standard deviation) or median (25th, 75th percentiles). Statistical significance was defined at p < 0.05 for all tests.
Results
Of the 507 patients with COPD referred for PR during the recruitment period, complete pre- and post-rehabilitation data were available in 418 patients with COPD undergoing hospital-based (HOSP) supervised rehabilitation (82% completion). Seventy-four of 122 patients completed the home exercise programme (61% completion). Baseline characteristics of the HOSP and HOME groups are summarised in Table 1. The groups were well-matched for proportion with existing cardiovascular disease and resting baseline SBP, diastolic blood pressure (DBP) and mean arterial pressure (MAP); however the HOME group had lower exercise capacity at baseline. There was also no significant difference in baseline blood pressures in the HOSP non-completers (n = 89) compared with the patients who finished the course (mean difference (95% confidence interval (CI)) SBP: −3.7 (−8.3 to 0.9) mmHg, p = 0.12; (DBP): −1.3 (−4.1 to 1.4) mmHg, p = 0.34).
Baseline characteristics of the patients undergoing unsupervised home exercise (HOME) and supervised hospital-based (HOSP) pulmonary rehabilitation.a
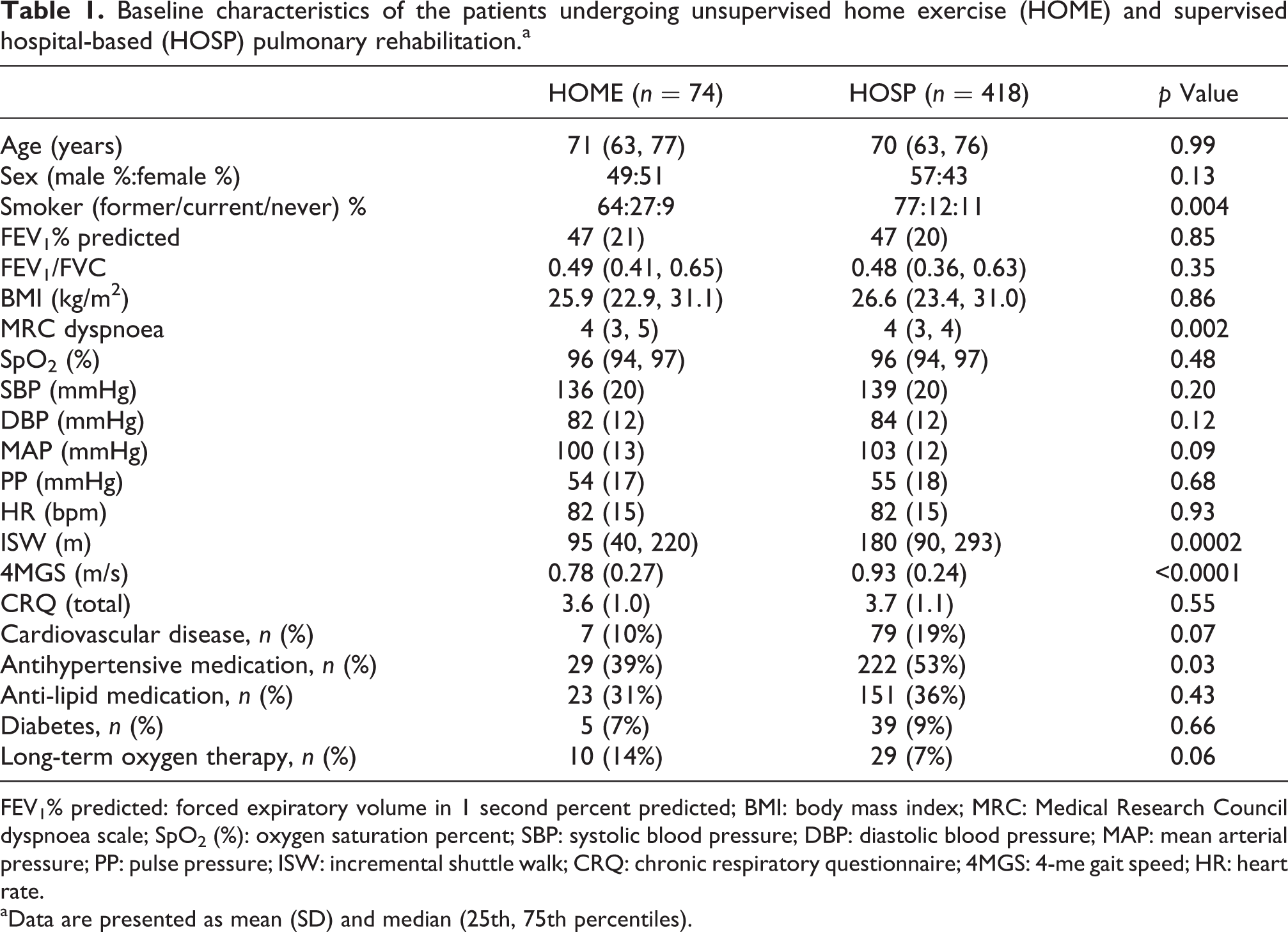
FEV1% predicted: forced expiratory volume in 1 second percent predicted; BMI: body mass index; MRC: Medical Research Council dyspnoea scale; SpO2 (%): oxygen saturation percent; SBP: systolic blood pressure; DBP: diastolic blood pressure; MAP: mean arterial pressure; PP: pulse pressure; ISW: incremental shuttle walk; CRQ: chronic respiratory questionnaire; 4MGS: 4-me gait speed; HR: heart rate.
aData are presented as mean (SD) and median (25th, 75th percentiles).
Table 2 demonstrates change in outcome measures and blood pressure for the HOSP and HOME groups. There were improvements in exercise capacity in both groups, with significantly greater changes observed in the HOSP group compared with the HOME group of patients (mean difference (95% CI) ISW 27 (11 to 42) m, p = 0.001). However no changes were seen in peripheral SBP, DBP or MAP in either group, although a small significant decrease in heart rate was noted for the HOSP group (Table 2). In the HOSP patients with a previous physician diagnosis of hypertension and/or cardiovascular disease (n = 128, 31%), a small but statistically significant increase was seen in mean (95% CI) SBP (3.5 (0.1 to 6.9), p = 0.048), but this was not found for DBP (Table 3). On stepwise linear regression analysis, only baseline age and SBP remained independent predictors of SBP change with PR, explaining 52% of the variance (adjusted R 2 = 0.25; standardized beta coefficients: age 0.10 (95% CI: 0.02 to 0.39); SBP −0.53 (95% CI: −0.58 to −0.42).
Response of blood pressure, functional performance and health-related quality of life to hospital-based (HOSP) PR and unsupervised home exercise (HOME).
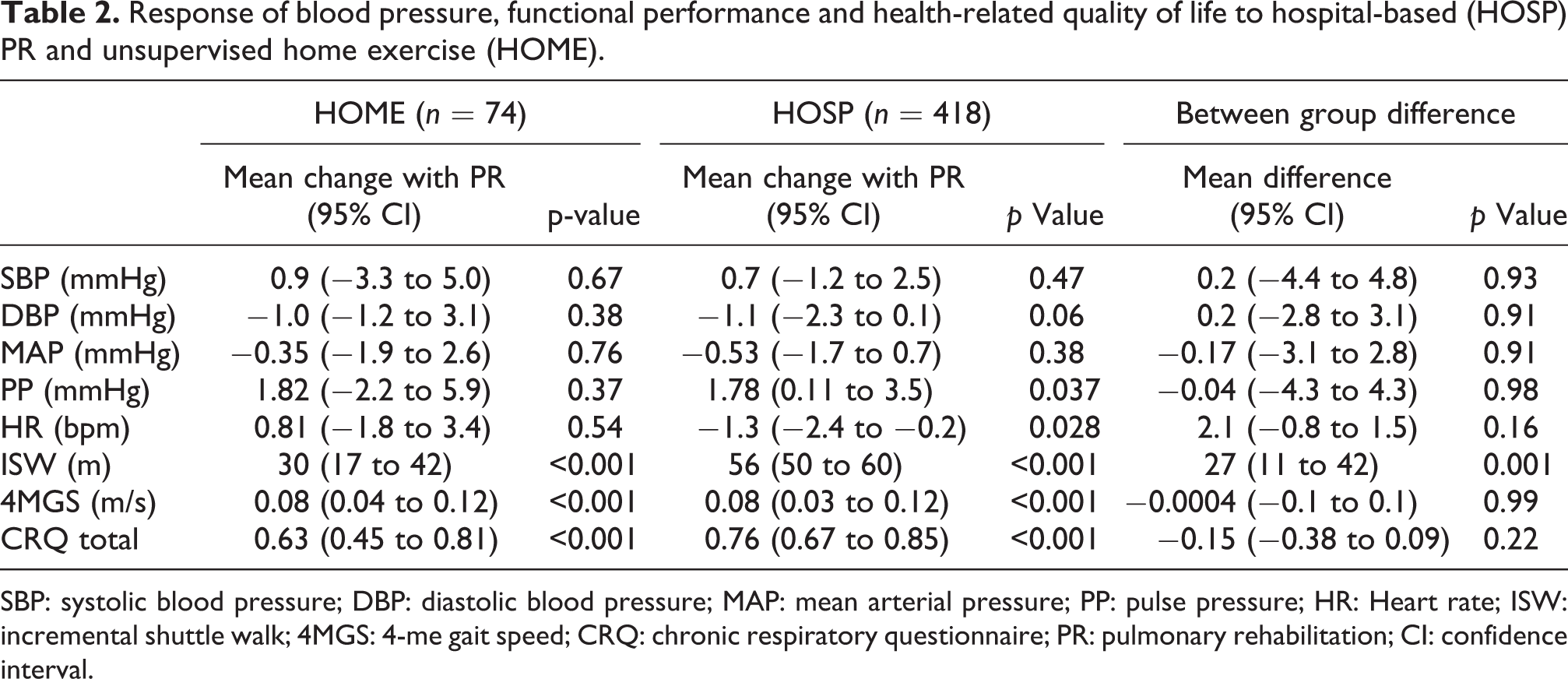
SBP: systolic blood pressure; DBP: diastolic blood pressure; MAP: mean arterial pressure; PP: pulse pressure; HR: Heart rate; ISW: incremental shuttle walk; 4MGS: 4-me gait speed; CRQ: chronic respiratory questionnaire; PR: pulmonary rehabilitation; CI: confidence interval.
Peripheral blood pressure response to hospital-based (HOSP) supervised PR in patients with diagnosed hypertension and/or cardiovascular disease (n = 128).a

SBP: systolic blood pressure; DBP: diastolic blood pressure; MAP: mean arterial pressure; PP: pulse pressure; HR: Heart rate; ISW: incremental shuttle walk; PR: pulmonary rehabilitation; CI: confidence interval.
aData are presented as mean (SD).
Analysis of the HOSP patients (n = 221) who attained the minimum important difference of the ISW distance (ΔISW
Comparison of the response to hospital-based (HOSP) supervised PR in patients who did and did not achieve the MCID of the ISW.a

Δ: delta change; SBP: systolic blood pressure; DBP: diastolic blood pressure; MAP: mean arterial pressure; HR: heart rate; ISW: incremental shuttle walk; PR: pulmonary rehabilitation; MCID: minimum clinically important difference.
aData are presented as median (25th and 75th percentiles).
Discussion
Summary of main findings
In contrast to our hypothesis, the main finding was that despite meaningful improvements in aerobic exercise capacity, peripherally measured SBP, DBP and MAP were unchanged following 8 weeks of supervised outpatient PR. Moreover, patients with known hypertension and/or cardiovascular disease also showed no clinically meaningful reduction in blood pressure with PR. Furthermore, patients with COPD undergoing outpatient supervised PR had blood pressure changes similar to a comparator group of patients undergoing an unsupervised home exercise programme.
Regular aerobic exercise can improve body composition, dyslipidemia, peripheral muscle strength and cardiovascular risk factors such as peripherally measured blood pressure in healthy individuals. Longitudinal studies of physical activity report a reduction of over 30% in cardiovascular risk and all-cause mortality with regular training. 19 After an acute bout of exercise training total peripheral resistance decreases 20 and blood flow is augmented. With longer term exercise training, postulated mechanisms for the reduction of blood pressure include reduced visceral fat, improved sodium elimination due to altered renal function, reduced plasma renin and catecholamine activity and reduced sympathetic and increased parasympathetic tone. 21,22
PR is the cornerstone of management in COPD and is universally recommended in international guidelines. 23,24 A major component includes exercise training and it would be logical to assume that a potential benefit of PR might include reduction of cardiovascular risk factors, particularly given the high prevalence of cardiovascular disease in COPD. Several recent studies have examined the role of exercise training or PR on arterial stiffness and blood pressure in patients with COPD. Vivodtzev and colleagues reported large reductions in SBP and arterial stiffness (as measured by carotid-brachial PWV) following endurance cycling training (5 days a week for 4 weeks). 4 Changes in PWV were correlated with changes in blood pressure. However, this was a small study (ten patients were trained, seven were not trained) of a selective population in a controlled laboratory environment using a training programme that is more intensive than usual and the results may not be generalizable to PR settings. Gale and colleagues investigated the effects of an outpatient-based PR programme comprising three exercise/education sessions per week for 7 weeks, 5 demonstrating significant reductions in aortic PWV (from 9.8 (3.0) m/s to 9.3 (2.7) m/s) and peripheral blood pressure from 138 (20)/83 (9) mmHg to 128 (24)/78 (12) mmHg (all p < 0.05). The magnitude of reduction in blood pressure was extraordinarily high and greater than would be expected by specific antihypertensive drug treatment. 25 Again, this was a small study (n = 22) of highly selected patients. Furthermore, there was a high dropout rate from PR (>30%), and no comparator COPD group with paired blood pressure measurements. Recently, Vanfleteren et al. studied 129 unselected patients completing an interdisciplinary PR programme comprising 40 supervised sessions. In contrast to previous studies, no changes were seen in aortic PWV or peripheral or central systolic, DBP and MAP. This study again did not measure paired arterial stiffness or blood pressures in a comparator group of patients with COPD, and although larger than previous studies was underpowered to detect a small change in blood pressure.
Strengths and limitations
Strengths of our study include the large sample size. We report the effects of PR on blood pressure in over 400 patients – more than twice the combined number of COPD patients previously studied. 4 –6 Unlike previous studies, our sample size was sufficiently large to have at least 80% power to detect a 3.1 mmHg change in SBP – the magnitude of change observed in a systematic review of exercise training in hypertension. 26 Furthermore, we report the change in blood pressure in a comparator group of 74 patients with COPD following an unsupervised low-intensity home exercise programme – significantly greater than the seven control patients studied by Vivodtzev and colleagues. 4
There were limitations to the study. As it was deemed unethical to deny patients with COPD access to PR, our HOME group comprised patients who declined outpatient supervised PR due to logistical reasons (transport and clash with existing commitments). They were instead provided with a home exercise programme, which was not directly supervised. We did not make any objective measurement of the individual training schedules (and self-reported exercise training is notoriously unreliable), but given that the change in exercise capacity was significantly smaller in the HOME group compared with the supervised HOSP group, it is reasonable to assume that the volume and intensity of exercise training was significantly less in the HOME group. Given the nature of the HOME group, it was difficult to tightly match for baseline characteristics such as ISW. However, the proportion of patients with coexisting hypertension and cardiovascular disease was similar between HOSP and HOME groups. Moreover, our groups were matched closely at baseline for the primary outcomes, namely SBP/DBP/MAP. Another weakness was that we observed a dropout of approximately 20% from the PR group, which may have inadvertently introduced bias. However, our dropout rate was similar to that of Vanfleteren’s study 6 and better than that observed in the Gale’s study. 5 It could also be argued that the absence of a change in blood pressure was due to insufficient volume of exercise training. However, this pragmatic study was intended to be real-world and the PR programme was organized and provided according to guideline recommendations. 1,27 Mean improvements in exercise capacity and health-related quality of life exceeded the accepted MCID for the ISW and the chronic respiratory disease questionnaire. 17,28 In a previous multicentre study, this programme performed as well as, if not better, than other PR programmes in the United Kingdom. 29 As part of a planned subgroup analysis, we investigated the change in blood pressure in patients showing large improvements in ISW (i.e. those assumed to have higher exercise training volume and intensity), but again saw no signal for blood pressure change. A possible explanation for these findings is the modality of training. Whereas aerobic training seems to have a beneficial effect upon blood pressure, some studies have suggested that resistance training may increase 30 –32 or have a limited effect on arterial stiffness 33–34 with greater decreases in PWV reported with resistance training intensity >60% of one repetition maximum. 35 However, although our PR programme included both resistance and aerobic training, it preferentially targets aerobic exercise capacity for improvement through rhythmic dynamic exercise such as walking, cycling and cross training, in line with most UK programmes.
Implications for clinical practice
In summary, the results of our study corroborate the findings of Vanfleteren et al. 6 Although PR is undoubtedly effective in improving exercise capacity and health-related quality of life, it is unlikely to reduce blood pressure and by implication, makes a mechanism of action in which arterial stiffness is reduced, less likely.
Footnotes
Acknowledgements
This project was undertaken at the NIHR Respiratory Biomedical Research Unit at the Royal Brompton and Harefield NHS Foundation Trust and Imperial College, London. The views expressed in this publication are those of the authors and not necessarily those of the NHS, The National Institute for Health Research nor the Department of Health.
Author contributions
All authors contributed to the design of the study, data collection and writing of the manuscript. JLC, DK and WD-CM conducted analysis of data and preparation of the final manuscript. WD-CM conceived the idea and is the guarantor of the paper, taking responsibility for the integrity of the work as a whole, from inception to publication.
Authors’ note
The authors would like to thank physiotherapists M Curtis, D Dilaver, K Ingram and physiotherapy assistants E Bone, D Carrington and M Ng for providing the pulmonary rehabilitation programme.
Conflict of interest
Professor Polkey reports being a recipient of a grant from the Technology Strategy Board for a project investigating cardiovascular function in COPD, which includes measurement of blood pressure (1.10.11-1.10.13 1101_CRD_MED_IBD_61188). This work was supported by the NIHR Respiratory Biomedical research unit at the Royal Brompton and Harefield NHS Foundation Trust and Imperial College who part fund MIP’s salary. No other author has a conflict of interest with the subject matter of the study.
Funding
JLC and SEJ are wholly funded by the Biomedical Research Unit. SSCK is supported by the Medical Research Council (MRC). WD-CM is supported by a NIHR Clinician Scientist Award, a Medical Research Council (MRC, UK) New Investigator Research Grant, a NIHR Clinical Trials Fellowship and the NIHR Northwest London Collaboration for Leadership in Applied Heath Research and Care (CLAHRC).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.