
Abstract
Fatigue is a symptom commonly diagnosed in cancers and in many other chronic debilitating diseases and is one of the main therapeutic targets for various pharmacologic and non-pharmacologic interventions. However, in chronic obstructive pulmonary disease (COPD), this symptom, which can be considered as the main extrapulmonary clinical feature of the disease, can impact significantly on the health-related quality of life of the patients. The aims of this review are to discuss the issues related to fatigue assessment in COPD and to highlight the importance of this symptom in this setting based on the data retrieved from articles published between 1987 through August 2014 available on MEDLINE database. Fatigue can be measured by various scales or questionnaires that are designed for generic purposes or for COPD-related purposes but is still underdiagnosed and undertreated. This is due to the fact that its clinical and prognostic relevance are not appropriately acknowledged. The early identification of fatigue clinical descriptors from patients’ reports could help with better management of this symptom.
Introduction
Fatigue is the most common symptom experienced by cancer patients and a common symptom encountered in both acute and chronic illnesses but its impact is considered to be deeper in chronic conditions. 1,2 Many controversies have surrounded the definition of this symptom, and many years ago, some authors even argued that fatigue might be considered as a syndrome and not as a symptom. However, nowadays fatigue is recognized universally as a complex syndrome with both physical and psychological features whereas the chronic fatigue syndrome is currently a well-defined entity in terms of clinical manifestations and diagnosis. 3,4
Chronic obstructive pulmonary disease (COPD) is an inflammatory disease of the lungs mainly related to smoking in which fatigue is the main extrapulmonary symptom. It is often underreported by the patient and underrecognized by the health-care professionals, and this leads to an increase in its impact on the health status, especially in the most advanced stages of the disease.
This situation might be also due in part to the fact that currently the management of this disease is rather focused on the respiratory symptoms and to a lesser extent on the “general” symptoms such as fatigue. Another explanation might be represented by the fact that sometimes dyspnea or the shortness of breath is mistakenly interpreted as fatigue and that consequently the therapeutic approaches used can only marginally reduce the severity of this symptom.
However, in COPD, fatigue if not treated appropriately can have a significantly negative impact on the prognosis of the underlying disease.
The aims of this narrative review were to discuss the main aspects related to measuring the fatigue and highlight the importance of this symptom in COPD patients. The literature reviewed was retrieved from MEDLINE, which was searched using the terms “fatigue” and “COPD” from 1987 through August 2014, and the draft was prepared taking into account the other specific recommendations of a recent guidance paper. 5
Fatigue as a symptom of COPD: Descriptors
Fatigue was initially recognized as an individual symptom in oncological conditions but still its definition was rather vague. Subsequently, fatigue was also recognized in other non-oncological diseases, being of particular clinical significance mostly in chronic diseases such as COPD.
However, its clinical definition has been rather unclear, and there were many attempts to set a conceptual framework for this symptom. In 1996, Ream and Richardson defined fatigue as being “a subjective and unpleasant symptom which incorporates total body feelings ranging from tiredness to exhaustion creating an unrelenting overall condition which interferes with individuals’ ability to function to their normal capacity.” 6
Subsequently, the same team of authors analyzed the potential attributes of fatigue in two populations of patients those with cancer and those with chronic obstructive airways diseases (i.e. COPD, bronchiectasis, and asthma). In these patients, five types of descriptive attributes related to fatigue were identified (see Table 1). 7 Unlike the cancer patients, the descriptors of fatigue related to chronic lung diseases were found to be less severe in terms of sensation and impact, for example, the perceived physical fatigue in cancer patient was described by a general sensation of malaise and exhaustion, associated with aching pains in the limbs, whereas in COPD patients this was described mostly in relationship with muscular force exhaustion as if following a strenuous exercise period and with no malaise. 7 The mental-related fatigue was generally described as impaired concentration, lack of motivation, and of enjoyment of the personal life. The impact of fatigue on the daily functioning was also found to be deeper in cancer patients than in COPD patients, while the latter category not mentioning a significant impact of fatigue on daily hobbies or past times like reading or walking around. COPD patients described a more significant impact of fatigue on the daily routine activities, whereas cancer patients reported this impact as being lighter due to the fact that they adjusted to this new symptom by performing those activities which least caused fatigue and by giving up to those eliciting a more severe symptom. In both categories of patients, the emotional impairment caused by the perception of this new symptom was experienced and testified by these patients, and in COPD, for example, emotional distress was found to be more significant in patients with a more active life prior to the disease-related fatigue installed. These patients also had a more constant emotional distress as compared to cancer patients who experienced it on rather transitory basis and related to the chemotherapy courses. 7
Fatigue attributes identified in two populations of patients (oncological diseases and chronic obstructive airways disease). 1
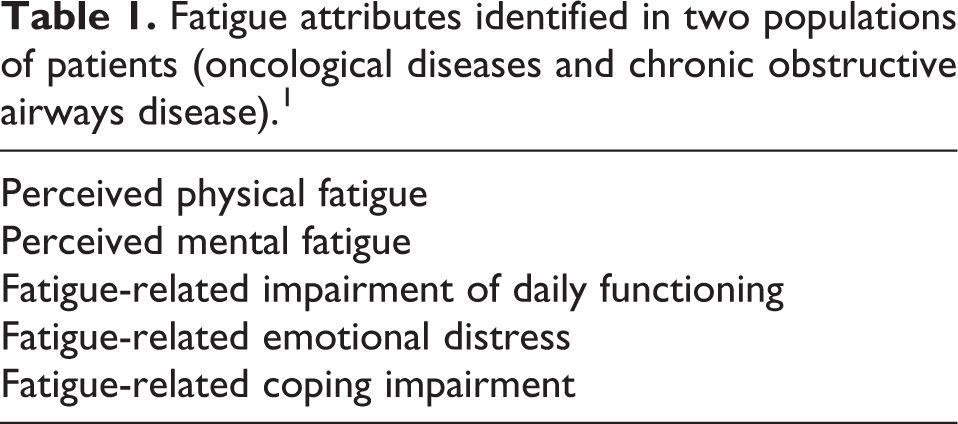
Coping was also found to be negatively affected by fatigue, where patients in both groups describing feelings of overwhelmingness and of lack of control of their own lives due to fatigue. 7
Alike in the cases of other chronic diseases in which fatigue was demonstrated to be a prominent symptom, in COPD patients, this was found to correlate with the overall disease severity as measured with the severity of the airways obstruction. Furthermore, various dimensions of fatigue were found to correlate significantly with other features of COPD such as impaired exercise capacity (physical fatigue), mental fatigue with depression, disease impact, or quality of life. 1
In a more recent study performed in a more selected population of COPD patients with various Global Initiative for Chronic Obstructive Lung Disease stages of disease, who were asked to describe the way they perceive fatigue, it was shown that these patients felt motivated to reconcile with the fatigue, the presence of this symptom being seen as a natural feature of their lung disease. Some of them also tried to understand this symptom and its causes, some of them preferred not to acknowledge the presence of fatigue because they felt they would not receive the expected explanations from health care or because they felt their social interactions would be impaired. The fact that fatigue took control of their lives and negatively influenced their daily activities was also recognized by these patients, and the feelings of anger or hopelessness associated with the gradual increase of this symptom were also described. The presence of fatigue made them to readjust their daily activities and to increase the number and the duration of the pauses between activities. 8
Generic scales used to measure fatigue in COPD
Fatigue is generally measured with three main types of instruments, namely, unidimensional symptom scales, multidimensional scales/questionnaires, and health-related quality of life questionnaires containing specific domains for fatigue. Most of these instruments can be labeled as “generic” because they have been used in various diseases including cancer but there are some newer questionnaires such as chronic respiratory disease questionnaire or such as the Manchester COPD fatigue scale, which circumvent the measurement of fatigue to the specific setting of chronic lung disease respectively to that of COPD.
Unidimensional scales
Unidimensional scales used to measure fatigue include numerical rating scales and unidimensional questionnaires.
Numerical rating scale for fatigue is a simple tool to assess the severity of this symptom in the daily practice. By the means of this scale, the severity of fatigue can be graded from 0 (no symptom) to 10 (most severe symptom), and in this way, the dynamics of the symptom under designated therapeutic interventions can be followed up easily by both patients or medical professionals. This approach is commonly used in oncology and in palliation.
Visual analog scales (VAS) for fatigue are often confounded with numerical rating scales most probably due to the fact that their grading systems are similar. VAS can be another simple tool to assess fatigue in COPD patients because it is simple to handle and easy to administer across patients with various educational levels.
However, in COPD, the number of reports using such instruments is very limited and for example in a study evaluating the correlation between fatigue and systemic inflammation, a Borg VAS scale was used to evaluate fatigue before and after exercise testing. 9
Apart from individual symptom scales such as that above mentioned, there are multi-symptom numerical scales such as Edmonton Symptom Assessment System (ESAS), which is an essential tool to assess the symptom burden in palliative care. This is a 10-symptom scale with 9 definite domains for pain, dyspnea, nausea, anxiety, depression, fatigue (tiredness), appetite, well-being, drowsiness, and 1 blank scale for another additional symptom in case it is reported by the patient. It was developed within the framework of the Regional Palliative Care Program in Edmonton Alberta. 10
ESAS has been extensively used in various types of cancer in its original form and it was found to be an useful tool to assess the severity of the fatigue in cancer patients, for example, in a sample of 1397 patients consecutively referred to radiotherapy, ESAS was demonstrated to be an useful tool to screen for the fatigue irrespective of the type of cancer included in the analysis. 11 Furthermore, for this tool, the minimal clinically important differences (MCIDs) for both improvement and worsening for the nine symptoms were recently calculated and these confirmed the very good potential of this simple tool to monitor their course over time, that is, in the sample analyzed, pain and fatigue were the most prominent symptoms, with the mean score for fatigue being, for example, 4.8. The MCID for fatigue worsening was calculated to be 1.8. 12 In COPD, in particular, there are no reports of ESAS used in this original form to screen for both pulmonary and extrapulmonary symptoms. However, a modified ESAS scale preserving the nine original symptoms but with the 4 instead of 11 grades of severity was used to evaluate the prevalence of the symptoms and how bothersome they were in patients with various types of chronic illnesses including COPD and fatigue was found to be a significant determinant of poorer quality of life, functional disability, or self-perceived health status. 13,14
Another unidimensional scale is represented by the Fatigue Severity Scale (FSS), which is a nine-item scale originally developed to assess fatigue severity in patients with multiple sclerosis and evaluate the fatigue severity in relationship with functional disabilities. 15 In COPD patients, FSS scores were found to correlate with multidimensional severity indexes such as BODE. 16
Such scales are very useful for a qualitative detection of symptoms such as fatigue because they provide rapidly with a score corresponding to a certain degree of the severity of the symptom. However, their main disadvantage is represented by the fact that they can only allow the identification of the symptom and of its severity without being able to offer essential details on other attributes of fatigue.
Multidimensional scales
Unlike the rating scales, which can be considered as unidimensional tools, because they are only able to explore severity of the symptoms, fatigue-specific questionnaires are usually multidimensional and can allow to obtain further information regarding the attributes of the symptom such as duration, frequency, or timing but also can help with evaluating the impact of the symptom on physical, mental, or social daily activities. 17 Table 2 presents an overview of the multidimensional fatigue scales used in COPD patients to date.
Overview of the multidimensional scales commonly used to evaluate fatigue in COPD.

COPD: chronic obstructive pulmonary disease.
Brief Fatigue Inventory
The Brief Fatigue Inventory (BFI) is a nine-item tool developed initially to explore fatigue in cancer patients. It helps to document the severity of fatigue at the moment of the administration, its extremes of severity over a 24-hour period and its impact on the general activity, on the mood status on the social life, and so on. BFI provides a global single score of fatigue, which is considered to be clinically significant if it is at least 7. 18
In patients with COPD, BFI was used in order to assess fatigue and its interrelationships with other symptoms such as dyspnea, anxiety, or depression. BFI scores were found to be directly proportional with mood disturbances (anxiety respectively depression) and with dyspnea. 19
Fatigue Assessment Scale
Fatigue Assessment Scale is a 10-item scale aimed at exploring various dimensions of fatigue such as the ability to perform various activities, mental fitness, and level of energy. 20 It was not used to measure fatigue in COPD but was demonstrated to be a reliable tool in sarcoidosis. 21
Identity–Consequence Fatigue Scale
Identity–Consequence Fatigue Scale is a complex 31-item tool generating five domains (see Table 2). 22 In COPD patients, it was used to demonstrate that fatigue severity was correlated with the level of lung function impairment with the functional status and that a severe fatigue was associated with a significantly higher risk of hospitalizations. 23
Fatigue Impact Scale
Fatigue Impact Scale (FIS) evaluates the impact of this symptom on quality of life and was developed in patients with chronic fatigue syndrome. 24 Despite its length, FIS is one of the most widely used fatigue scales across various chronic pathologies. In COPD patients, it was used to correlate fatigue with quality of life and with the effort tolerance. 25 Currently there is a modified version of the FIS (MFIS) and an abbreviated form of FIS which are used in the disability assessment of patients with multiple sclerosis. 26
Multidimensional Fatigue Inventory
This scale was developed in oncology patients, has 20 items, and generates five domains (see Table 2). 27 Multidimensional Fatigue Inventory (MFI-20) is frequently used in rehabilitation programs to assess the effectiveness of the interventions applied. 28
Fatigue Severity Scale
FSS is a nine-item scale originally developed to assess fatigue severity in patients with multiple sclerosis and evaluate the fatigue severity in relationship with functional disabilities. 15 In COPD patients, FSS scores were found to correlate with multidimensional severity indexes such as BODE. 16
Multidimensional assessment of fatigue
This was developed in rheumatoid arthritis patients and is a revision of the Piper Fatigue Scale, which in turn was developed in oncology. It is focused on detecting its type, the severity, and the distress it produces on the daily activities. In COPD, this scale was found to be useful to demonstrate various corresponding levels of physical activity impairment corresponding to various stages of severity of the perceived fatigue. 29,61
FACIT scale for fatigue
There are two scales for fatigue developed within the Functional Assessment of Chronic Illness Therapy (FACIT) framework, namely, the extended version with 41 items and the short version with 13 items, which were originally developed for cancer-related fatigue but subsequently were applied as such or modified to be more appropriate for other diseases. 30 FACIT-F scale modified for COPD is a relevant example in this respect and is a nine-item scale derived from the original 13-item scale based on the principal component analysis. When applied on a sample of 2107 patients with COPD included in the ECLIPSE (Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints) study, it was demonstrated to be a reliable and valid measure of fatigue and was able to discriminate among patients with various levels of exercise capacity impairment and among patients with various degrees of depression. 31
Health-related quality of life questionnaires
Health-related quality of life questionnaires are instruments that are more complex than the symptom scales and that are used to investigate how the health status interferes with various aspects of the daily life in a generic manner (and they are called generic health-related quality of life questionnaires) or in a specific manner (and they are called disease-specific health-related quality of life questionnaires).
Medical outcomes study SF-36
From the first category, the most commonly used generic questionnaire to assess fatigue is represented by short form 36 (SF-36), which has 36 items generating 8 domain scores, physical functioning, role physical, bodily pain, general health perceptions, vitality, social functioning, role emotional, and mental health. 32
In COPD, SF-36 was widely used to assess health-related quality of life changes as a result of various pharmacological or non-pharmacological interventions. 33 –35 Furthermore, it was used to differentiate various levels of severity of fatigue in COPD patients and found to correlate well with disease-specific questionnaire scores, with exercise capacity impairment and with dyspnea level. 36
PROMIS questionnaires
Patient-Reported Outcome Measurement Information System (PROMIS) questionnaire is a complex generic instrument with 43 items aimed at exploring the quality of life from a global, physical, mental, and social points of view. It generates domains such as pain, fatigue, mood status, and social impact. In COPD, it was recently tested for its psychometric properties in comparison with the Euroqol-5D questionnaire. 37
Chronic Respiratory Disease questionnaire
This disease(s)-specific questionnaire is a 20-item scale generating scores for dyspnea, fatigue, emotional function, and mastery and is one of the most commonly used of the kind tools in the setting of COPD. 38,39
COPD-specific fatigue scales
Manchester COPD fatigue scale
Manchester COPD fatigue scale is a 27-item scale generating three domains, namely, physical, cognitive, and psychosocial, developed by the same team who validated the modified FACIT-F short fatigue scale modified for COPD. This tool was found to correlate well with other fatigue scores measured with instruments such as Borg scale and FACIT-F, with dyspnea scores or with health-related quality of life questionnaires such as St. George’s Respiratory Questionnaire. 40
COPD and asthma fatigue scale
This is another COPD/asthma unidimensional instrument specific for fatigue, which has 12 items and which was developed on a sample of 162 patients with asthma and COPD. The score of this scale was found to correlate well with the scores of health status questionnaire (SGRQ; p < 0.0001) and were found to differ proportionally with disease severity, the number of exacerbations, and health status scores (p ≤ 0.0014). In asthma, the fatigue scores as assessed by this scale were found to correlate significantly with a disease-specific questionnaire scores (Asthma Quality of Life Questionnaire, p < 0.0001) and to exhibit the same variability across various disease-severity stages, various exacerbations rates, and various health status scores (p ≤ 0.0024). 41
Fatigue as a symptom in COPD: Why is it important to measure it in COPD patients?
In COPD, fatigue is not related to only one pathogenic pathway but it is rather the clinical expression of interactions among different such abnormalities. The most commonly encountered but yet poorly studied in this disease are anemia, hypoxemia, and sarcopenia/cachexia. The amount of the limited data regarding the correlation between fatigue on the one hand and each of the abnormalities listed above also explains why they were not identified as predictors of fatigue, this being rather strongly influenced by the physical fitness, mood status, and the degree of lung function impairment.
Despite fatigue is still rather marginally considered from a clinical point of view, its relevance in COPD setting is strongly supported by the fact that this symptom has a prognostic value for both mortality and morbidity of the disease.
Clinical and pathogenic relevance
As fatigue is a complex symptom with both physical and mental dimensions, it is difficult to find only one pathogenic mechanism that can be attributed to this symptom. Furthermore, in COPD there is a complex interplay among multiple pathways and this can explain in part why one pathogenic loop can give birth to several symptoms (i.e. hypoxemia can lead to fatigue, dyspnea, or depression) or why one symptom can be the result of the cross talk among these pathways. Fatigue seem to be the “by-product” of these pathways and seem to interact with other symptoms such as those listed above. By knowing the possible pathogenic mechanisms leading to fatigue in COPD patients, it is hoped that the therapeutic approaches for this symptom can be improved.
Hypoxemia
The interaction between hypoxemia and fatigue is less well studied in COPD but is well documented for the high-altitude hypoxemia. In this latter setting, the physical/muscular fatigue as a result of hypoxemia was documented by various studies. 42
In COPD, on the other hand, several reports demonstrated that in patients with COPD and resting hypoxemia, fatigue severity was reduced on short-term basis by ambulatory oxygen therapy. These effects were also replicated on long-term basis in a randomized controlled study performed again in patients with COPD and severe resting hypoxemia in whom the administration of oxygen therapy improved fatigue whereas the lack of such therapy was associated with a worsening of this over time. 43,44
Systemic inflammation
Fatigue was described as a symptom in chronic or debilitating diseases such as cancer or type 2 diabetes. In both cases, a link between fatigue and systemic inflammation was demonstrated; for example, in breast cancer survivors, fatigue was associated with significantly higher levels of interleukin 1 (IL-1), tumor necrosis factor α (TNF-α) and of their receptors, or of neopterine, whereas in type 2 diabetes C-reactive protein (CRP), IL-6, or TNF-α were the inflammation mediators that were found to correlate with fatigue. 45,46
In COPD, the existence and the complexity of the systemic inflammation has been more recently recognized. This inflammation was demonstrated to be the result of the upregulation of various subsets of lymphocytes (CD8+, natural killer cells, etc.) and can be demonstrated by various biomarkers such as CRP, IL-6, fibrinogen, or TNF-α. 47,48
Such biomarkers were found to correlate significantly with disease mortality and morbidity, this latter being represented by an increased frequency of exacerbations. 49,50
As in the case of other diseases such as those discussed above in which the chronic systemic inflammation plays a major pathogenic role, in COPD, the presence of this type of inflammation might similarly manifest clinically with general symptoms such as fatigue. In fact a recent study evaluating the correlation between symptoms of fatigue and depression and biomarkers of systemic inflammation such as IL-6 or TNF-α found that exertion-related fatigue measured with fatigue Borg scale correlated significantly with the serum levels of TNF-α. 9
Anemia
In cancer, anaemia-related fatigue has been demonstrated by various studies in particular in patients receiving chemotherapy, in whom fatigue scores were found to correlate significantly with anemia severity. That this correlation reflected the pathogenesis of fatigue in these patients was demonstrated by the improvement of the severity of this symptom as a result of erythropoiesis-stimulating therapy. 51
In COPD, the presence of anemia was found to be associated with poor disease prognosis and with an increased severity of dyspnea but an association between this condition and fatigue was inconstantly reported. 52,53
Skeletal muscle loss (sarcopenia) and cachexia
In COPD patients, progressive muscle loss is often described. This is demonstrated to significantly influence the prognosis of the disease in a negative manner by increasing the risk of frequent exacerbations and by enhancing the ventilatory dysfunction, which can lead to hypercapnic respiratory failure. Cachexia is the overall result of a negative energy balance, which can be caused by poor food intake, increased energy expenditure, accelerated protein turnover, systemic inflammation, and persistent hypoxemia. In the case of systemic inflammation, in particular, the higher serum TNF-α levels were found to correlate well with weight loss and in particular with muscle loss in COPD patients with cachexia. 54 –56
Clinical predictors of fatigue in COPD
The attempt to identify predictors of fatigue in COPD patients is of a more recent date. An initial study performed in 107 COPD patients examined the relationship between fatigue as assessed with the FACIT-F scale (see Table 2) and variable relevant for the COPD outcome such as lung function (measured with forced expiratory volume in one second), exacerbation rate, depression, or physical activity (measured with the time spent outdoors), and it was found that fatigue correlated directly with the depression level and annual exacerbations rate and inversely with the time spent outdoors. 57
In another study performed in 130 patients with moderate-to-severe COPD, dyspnea, depression, and sleep quality were identified among the strongest predictors of fatigue in these patients. 58
Most recently a study enrolling 74 patients with COPD and in whom fatigue was measured with the MFI (see below), it was found that depression, muscle strength, and the peripheral oxygen saturation (SpO2) measured at the end of the exercise testing were the most powerful predictors of the general fatigue, whereas depression, lung function, and the exercise capacity were found to best predictors of physical fatigue. Mental fatigue was best predicted by depression and the end exercise SpO2. 59
Fatigue in COPD: Prognostic impact for disease mortality and morbidity
Fatigue despite being an underrecognized symptom in COPD is not lacking impact on the disease prognosis. This is not only demonstrated by quantifying fatigue by the mean of specific scales and then by comparing the obtained values with those of healthy subjects but also by evaluating the association between their severity and the morbidity of the disease (i.e. exacerbations rate) or mortality of the disease.
In the first case, many reports demonstrated that more severe fatigue is associated with more frequent exacerbations. 57
In the second case, fatigue was identified as an independent predictor of mortality in a cohort of 434 patients derived from the OLIN COPD study and in whom fatigue was assessed with FACIT-F questionnaire. 60
Conclusions
In COPD, fatigue is an important though less sought parameter for symptom. Its importance is given on the one hand by the complexity of the potential etiologic factors and on the other hand by its major though underestimated impact on the quality of life of the patients with COPD and on the prognosis of the disease itself.
Given that fatigue becomes clinically evident in the more advanced stages of the disease, this symptom can be seen not only as an indicator of the need for pulmonary rehabilitation but also as an indicator of the need for palliative care. If for the former, the physical fatigue is the most relevant as a target for the intervention, and the latter sees the symptom of fatigue from a physical, psychological, social, and spiritual points of view and aims all these aspects via specialized approaches. The palliative care approach for fatigue in COPD patients is supported by the constant association between the impairment of the physical functioning with that of mental impairments that are significant especially in more aged patients and in patients with chronic hypoxemia.
Currently there are various types of clinical descriptors for fatigue and these can be used in the clinical practice to suspect whether fatigue exists and that it is relevant for the patient.
Once the fatigue is considered to be a symptom worth being further evaluated for the disability it induces to the patient, various scales or questionnaires can be used to quantify it. These tools focus specifically on different dimensions of fatigue and many of them described in this review were also found to be valid instruments in COPD-related fatigue.
These aspects have to be taken into consideration when measuring fatigue in order to best capture the impairments it brings to the daily life and in order to assess its severity. Such an approach would allow to recognize the relevance of this symptom within the larger context of the disease and would allow to tailor better integrated management pathways for patients experiencing it.
Footnotes
Conflict of interest
The authors declared no conflicts of interest.
Funding
This draft was funded by the grant no 29233/20.12.2013 provided by the “Grigore T Popa” University of Medicine and Pharmacy, Iaşi, Romania.