
Abstract
Pulmonary rehabilitation (PR), following an acute exacerbation of chronic obstructive pulmonary disease (COPD), has been found effective in some studies in reducing readmission rates as and has recently been recommended by the PR guidelines. However, very recent reports suggested that PR is not feasible after a hospital admission for a COPD exacerbation. The objective of this study is to investigate the knowledge gap on the underlying reasons for nonparticipation in PR in the posthospitalization period. We qualitatively analyzed the responses of 531 patients hospitalized for a COPD exacerbation who were not interested in participating in either PR (home or center based) or physical activity monitoring program after being discharged from the hospital. The responses were coded thematically, and independent reviewers compiled the raw data into themes. The characteristics of the 531 subjects (45% male) who declined the intervention are as follows: age was 70 ± 10 years, mean forced expiratory volume in one second (FEV1%) predicted 40 ± 16, and age, dyspnea, and airflow obstruction index 6.0 ± 1.6 (scale 0–10). The themes for not attending include lack of interest (39%), the perception of “being too ill or frail or disabled” (24%), the perception of being “too busy or having too much to do” (11%), distance or the need of travel (11%), commitment issues (7%), comorbidities (6%), and lack of social support (2%). We identified barriers for PR or just physical activity programs after a hospitalization that may affect implementation of such programs. Implementing posthospitalizations program in COPD may require patient engagement and mindful and compassionate professionals who may individualize program components to focus specific deficits and particularly patients’ preferences.
Introduction
Supervised pulmonary rehabilitation (PR), following an acute exacerbation of chronic obstructive pulmonary disease (COPD), has been found to be successful in reducing readmission rates as well as eliciting benefits in terms of patient’s functional capacity and health status. 1 –4 For that reason, it has been proposed as an intervention in the posthospitalization period and has recently been recommended by the PR guidelines. 5
However, very recent reports suggested that PR cannot be implemented after a hospital admission for a COPD exacerbation 6,7 since only 9% of patients that are able to complete PR after a hospitalization.
There is a knowledge gap exploring the underlying reasons for nonparticipation in PR in the posthospitalization period.
This report aims to summarize the reasons for nonparticipation in posthospitalization physical activity programs including PR from large COPD cohort of patients hospitalized for an exacerbation.
Methods
The study sample includes 712 subjects who were hospitalized in a tertiary care institution (Mayo Clinic or Health Partners Regions) for a COPD exacerbation. All approached patients in this study had a signed research authorization.
Electronic medical record sniffers were built to facilitate greater efficiency in the screening process for not missing out cases. 8 Eligible patients were approached in their hospital rooms or by follow-up telephone calls after declining a research study that involved two active arms (physical activity intervention), namely, either PR (home or hospital based) plus health coaching (arm 1) or physical activity monitoring with feedback (arm 2). Both interventions were free of charge.
Patients who indicated they were not interested in participating were then asked whether they would be willing to share why they felt that way to identify patient perceptions which influenced their decisions to not participate in the proposed “free” interventions that require only one visit in person but otherwise was telephonic based. The study coordinators would record the patient’s own words in the recruitment log, such as “this sounds like it is too much for me,” “I have a lot going on with family issues right now,” or “I just can’t see myself doing this,” for example. The list of reasons why participants did not want to participate was coded thematically by three independent team members who reviewed the complied raw data and coded the responses using a thematic list translating them into themes. Coder themes and allocations were then compared, and all disagreements in themes allocations were discussed until a consensus was reached on the most appropriate code to capture the patients’ words. 9,10
Demographic information was collected in the approached patients, including pulmonary function test. Dyspnea was measured using the modified Medical Research Council (mMRC) dyspnea scale. 11 Age, dyspnea, and airflow obstruction (ADO) index score was calculated for each patient.
Results
In total, 877 patients were eligible, as they have been hospitalized for a COPD exacerbation and 772 were approached (Figure 1). Of these, 531 patients were not interested in the proposed interventions, PR or physical activity monitoring (Figure 1) and were then approached for this study qualitatively.

CONSORT diagram.
The characteristics of the 531 subjects (45% male) who declined the intervention are as follows: age was 70 ± 10 years, mean forced expiratory volume in one second percentage (FEV1%) predicted 40 ± 16, and ADO index 6.0 ± 1.6 (scale 0–10).
The FEV1% predicted, age, mMRC dyspnea score, and composite ADO index of the individuals who declined the proposed interventions and hence part of this study were not different from the characteristics of recruited patients (p = not significant).
Reasons for declining the intervention are shown in Figure 2.
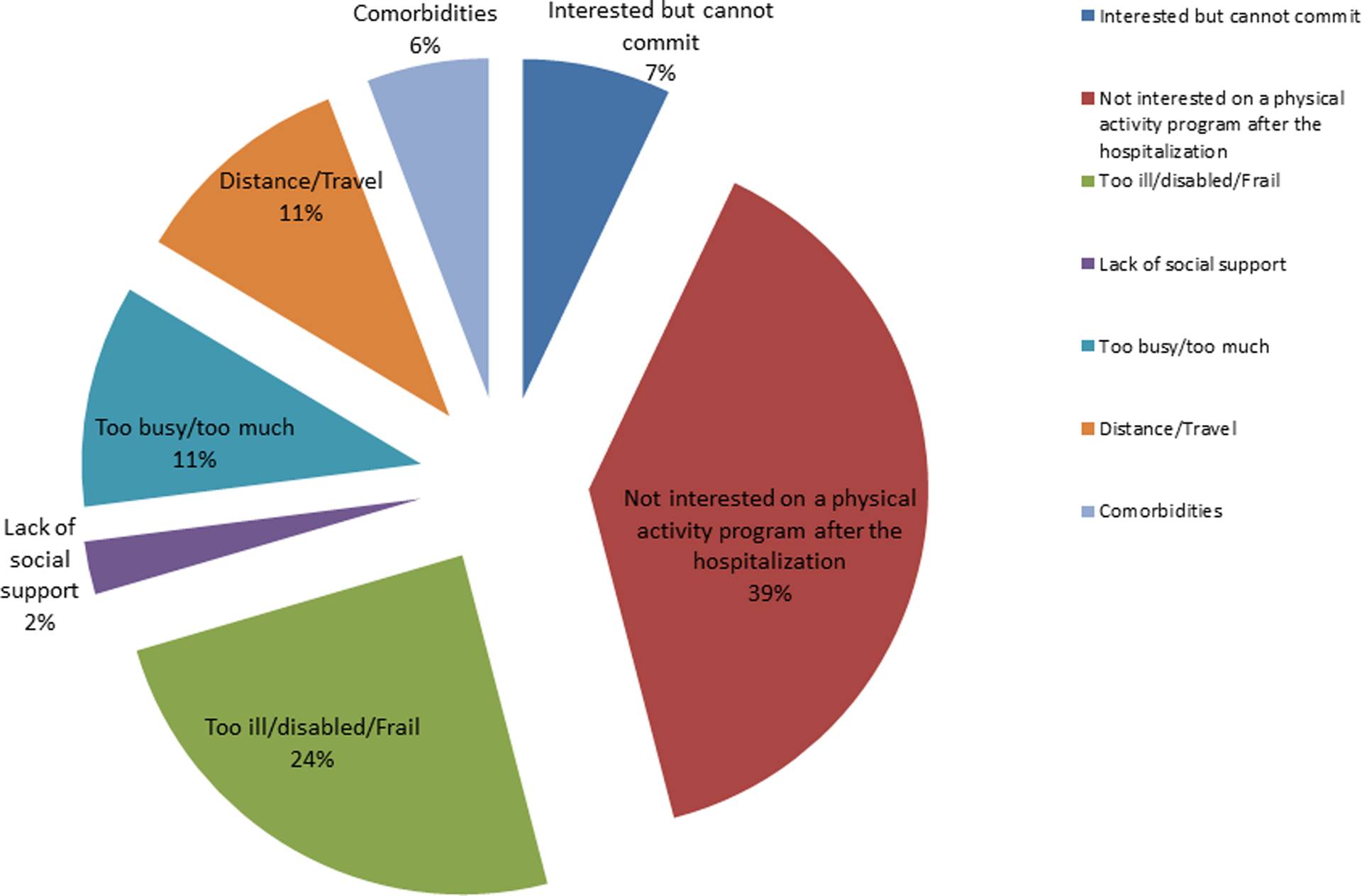
Patient’s reasons for declining pulmonary rehabilitation or physical activity monitoring after a hospitalization for a COPD-exacerbation. COPD: chronic obstructive pulmonary disease.
Discussion
Supervised PR after a hospital admission for COPD exacerbation has been reported as beneficial for readmissions and meaningful outcomes in COPD 1,3,4 ; however, many patients do not get to attend PR. 6,12 This report aims to increase our understanding in a hot topic for reasons why patients may turn down or are reluctant to consider PR or a physical activity intervention in the immediate period after a hospitalization for COPD exacerbation. Insights from this report may be seminal to “craft” post-hospitalization interventions that aim to prevent readmissions and improve quality of life.
One quarter of the individuals approached felt too sick or frail for any activity-related intervention (Figure 2). To our knowledge, this report represents the first evidence to ascertain this fact. A previous report has suggested that PR programs are possibly not adjusted to meet the needs of frail patients in the post-exacerbation period, which results in and poor attendance. 7 The latter is demonstrated in the attrition observed from referral to attendance at PR programs and the small patient numbers in post-exacerbation research studies. 13 Based on our results, we believe that in many cases, the initiation of palliative care may be appropriate to at least be considered 14 (particularly in patients who respond saying that they are too frail or sick). The assessment of frailty by measuring gait speed, 15,16 for example, may be informative to support a palliative route.
We found that more than one-third of the individuals (39%) who declined physical intervention felt plainly not interested to even discuss the options of PR or an activity monitoring program. This group of patients may correspond to the group of “disengaged” COPD patients as described in a very recent study that explore “phenotypes” of patients who suffered hospitalized exacerbations. 7 The attitude or confidence of the individuals to engage in the own care may have everything to do with poor outcomes in COPD as suggested in a recent study by Bucknall et al. 17 in which individuals who were confident to self-initiate and action plan for exacerbation had less readmission to the hospital. Perhaps knowing which patients belong to the “disengaged phenotype” 7 is an important assessment at discharge from the hospital. Alternatively, the lack of interest may represent a distressed patient as another described phenotype of hospitalized COPD patients, that is, patients with higher emotional characteristics and more severe symptoms of anxiety and depression. 7 Being mindful of heightened emotional states by acknowledging patients’ distress is likely to promote therapeutic alliance and future adherence. In this randomized study, we offered a much lighter touch intervention as an alternative to rehabilitation by just monitoring physical activity and providing feedback; still many participants declined. While it can be speculated whether the research process hindered patients to embrace the proposed physical activity interventions, the majority of patients who declined perceived themselves as “not interested” indicating that the proposed interventions did not apply to their situation. It is plausible that arriving to the “right” intervention (for each individual patient) may come after establishing rapport with the patient through a provider who can meet the patient interests and needs.
A recent report suggested that patients who declined PR after an exacerbation are many times tormented by shame and stigmatization that translates in lower self-worth, a condition associated with reduced help seeking and isolation. 18 The latter sensitize participants toward their interactions with health-care professionals who many times show a critical and judgmental attitude which may increase avoidant behaviors, such as refusal of PR. 18 There is a current therapeutic initiative for these kind of patients, that is, mindfulness-based interventions. 19 Mindfulness encourages patients to accept their feelings and disengage from the content of distressing thoughts by focusing on simple goal-based actions like breathing awareness, just walking or wholeheartedly devoting to simple tasks. Mindfulness interventions have been proved effective in asthma 20 and alone or when used in combination with “acceptance and commitment therapy” 21 may offer a more promising and less immediately threatening treatment alternative to PR.
About 11% of the patients who declined felt that there was too much “going on” at the moment suggesting that individuals after a hospitalization are basically too “overwhelmed or too busy to consider anything”. Analysis of the answers of this group included individuals who were already working full- or part-time and others who were too busy with medical appointments.
We were surprised to find the prevalence (7%) of people interested but cannot commit. Analysis of this subgroup indicated the presence of addictions particularly alcohol abuse and depression. Behavioral counseling is perhaps more indicated (more that exercise) as the most appropriate rehabilitation in this group of individuals.
While distance to the PR site is important in most studies for not attending PR, 7,22 it was a lower barrier (11%) in this study since the option for home exercise required almost no travel.
Finally 6% of the approached patients reported “other comorbidities need more attention” as a reason for declining a physical activity program. That group represents the recently reported systemic disease COPD phenotype. 23
Previous reports support some of our findings, namely, factors related to perception of being ill (too sick from our coding) such as age, oxygen therapy, and frailty and factors related to comorbidities and social factors like living alone were reported associated with declining PR. 24,25
Study limitations
We approached patients for PR or physical activity monitoring under the umbrella of a research study. The latter may have impacted patients for participation in research versus a clinical, nonresearch setting. However, the large number of patients interviewed and the similarity of the themes mentioned in previous published works provide validity to this report. We acknowledge also as limitation that responses could have a population-dependent nature (mid west region of the United States), but we feel that the commonsensical nature of the themes make them generalizable.
Customizing the type of intervention in the posthospitalization period is of paramount importance, given the different phenotypes that are being now identified and recognized in COPD. 23 Conventional PR and even simple physical activity programs are certainly not for everybody after a hospital stay, that is, we believe that this is a great example of an effective therapy that is difficult to be implemented and disseminated.
Future interventions for preventing rehospitalizations in COPD will require tailored programs that can vary from very comprehensive to extremely simple. The search for the right intervention is far from being settled. It is plausible that arriving to the right intervention (for each individual patient) may come after establishing rapport with the patient through a provider who can meet the patient interests and needs. PR itself in the posthospitalization period carries conflicting results, while supervised conventional PR has been reported to effective, 1 – 4 a very recent randomized and well-powered study of early rehabilitation started in the hospital and followed by home training supervised by phone demonstrated no effect on rehospitalization or 12-month outcomes. 26 Interestingly, a simple walking program (no education, just supervised walking) has recently been confirmed in a randomized study as an effective intervention to improve quality of life and exercise capacity. 27
The evidence seems to indicate that meaningful supervision (the one that lead to patient engagement) is a critical factor in any intervention to achieve success. We postulate that the state of mind of the health professional discussing posthospitalization care has a critical role on the success implementing them. When introducing such programs, professionals need to embrace compassion and understanding, given the sensitivities of the patients to and facilitate open collaborative discussion that may represent the breakthrough to facilitate uptake of physical activity programs. Motivational interviewing represents an excellent framework for those conversations with severe COPD patients. 26
Finally, psychological assessment and frailty measures, like gait speed, 15 may be critical at the time of discharge for prognostication and to individualize interventions that may address specific deficits and particularly patients characteristics and interests. Palliative care and mindfulness programs may represent other options of rehabilitation for frail or emotionally affected patients. Hospital admission creates a unique opportunity to engage the patient in his/her trajectory, for example, right there may be the key for delivering programs which may be successful. Learning from the “experts” (the patients) can inform the crafting of interventions that can be eventually implemented.
Footnotes
Authors’ Note
The article was concepted and designed by RB. He also carried out analysis and interpretation of data, drafting the article, and final approval of the version to be published. Authors MW, PN, and CM were involved in interpretation of data and revising it critically for important intellectual content.
Conflict of interest
The authors declared no conflicts of interest.
Funding
This work was supported by a grant (grant no: 1R01CA163293-01 to RB) from the National Heart, Lung and Blood Institute, National Institutes of Health, USA. Clinical trial registration no: NCT01058486; primary source of funding: NIH – NHLBI 5R01HL094680-05.