
Abstract
The 6-minute walk distance (6MWD) is one of the most commonly used measures of functional capacity in lung cancer, however, the minimal important difference (MID) has not been established. The aims of this exploratory study are, in lung cancer, to estimate (1) the MID of the 6MWD and (2) relationship between 6MWD, demographic and disease-related factors. Fifty-six participants with stage I–IV lung cancer completed the 6MWD prior to treatment and 10 weeks later. No exercise intervention occurred. Additional measures included European Organization for Research and Treatment of Cancer questionnaire (EORTC-QLQ-C30) and questionnaires assessing function, physical activity and symptoms. MID was calculated using anchor- and distribution-based methods. The mean 6MWD decline in participants classed as deteriorated was 60 m compared with 16 m in participants classed as not-deteriorated (p = 0.01). The receiver operating curve indicated a cut-off value for clinically relevant change to be 42 m (95% confidence interval (CI) 6–75) (area under curve = 0.66, 95% CI 0.51–0.81) or a 9.5% change. Distribution-based methods indicated an MID between 22 m (95% CI 18–26) and 32 m (95% CI 20–42). Higher 6MWD correlated with better function (r = −0.42, p = 0.001), physical activity (r = 0.56, p < 0.005) and dyspnoea (r = −0.44, p = 0.001). The MID for deterioration of the 6MWD in lung cancer is estimated to be between 22 m and 42 m or a change of 9.5%.
Introduction
Lung cancer is associated with high disease burden and physical hardship. 1,2 Impairment in functional capacity and progressive functional decline are prevalent following diagnosis 3 and have the potential to significantly impact the individuals’ health-related quality of life (HRQoL). There is a growing body of evidence supporting the role of exercise training to maximize functional capacity and prevent functional decline in lung cancer, 4,5 however, the clinimetric properties of appropriate outcome measures for such interventions need further refinement. 6
The 6-minute walk distance (6MWD) is a measure of functional capacity. It is a field walking self-paced test that measures the distance an individual can walk over a 25 or 30 m track in 6 min. 7 It is the most widely used non-laboratory test to measure functional capacity in individuals with chronic lung disease, including those with lung cancer and chronic pulmonary obstructive disease (COPD). 6 In lung cancer, a common target of exercise interventional studies is achieving improvement in the 6MWD. 4,5 Similarly, the 6MWD is commonly used by clinicians to objectively map changes (deterioration, improvement or maintenance) in patients’ functional capacity during and following cancer treatment.
The minimal important difference (MID) is the smallest change in an outcome that patients and clinicians consider to be clinically relevant. 8 Change in the 6MWD can be interpreted using the MID, as this provides information on whether the change is clinically meaningful. To date, the MID of the 6MWD in lung cancer has not been reported and therefore, commonly, the values of 25–35 m (determined for the COPD population) are used in lung cancer. 9,10 However, no studies have determined whether the MID established for COPD is generalizable to the lung cancer population. Therefore the aims of this exploratory study are, in lung cancer, to estimate (1) the MID of the 6MWD and (2) the relationship between 6MWD, demographic and disease-related factors.
Methods
Study subjects
Participants were recruited prospectively from three tertiary hospitals in Melbourne, Australia, from December 2008 to October 2012. Patients were eligible to participate if they were English-speaking adults, aged 18 years or over, with newly diagnosed stage I–IV non-small cell lung cancer (NSCLC) and had not started any form of treatment (surgery, chemotherapy or radiotherapy). Exclusion criteria included any musculoskeletal condition or co-morbidities precluding field exercise testing. All sites had ethical approval and written consent was obtained.
Study design
Participants were assessed at two time points, namely, baseline (close to diagnosis and pretreatment) and follow-up (8–10 weeks later, commonly during chemotherapy or radiotherapy). During the time period between testing, standard care at the institutions was followed and not modified. Participants were not offered formal education regarding physical activity or exercise and referral to rehabilitation was not part of usual care at the centres.
Outcome measures
The 6MWD was conducted according to published American Thoracic Society recommendations 7 and participants were given standardized instructions and encouragement during the test. Participants were monitored throughout the test with portable pulse oximetry. At each testing session, duplicate tests were performed for reliability and the greatest 6MWD was used for analyses. 7 In the case where participants declined or where unable to perform a repeat 6MWD within the 1 hour testing session, the first 6MWD was used.
At each time point participants completed the European Organization for Research and Treatment of Cancer questionnaire and lung cancer module (EORTC-QLQ-C30-LC13). 11 This questionnaire assesses HRQoL over the past week. The 30-item core questionnaire includes nine multi-item scales comprised of five functional scales (physical, role, emotional, cognitive and social functioning), three symptom scales (pain, fatigue and nausea/vomiting) and a global health status/quality of life scale and six single-item scales (appetite loss, dyspnoea, diarrhoea, constipation, insomnia and financial impact). 11 The 13-item LC13 supplementary module includes multi- and single-item scales measuring symptoms and treatment side effects specific to lung cancer. 12 Responses to most questions are rated on a four-point Likert-type scale according to occurrence in the past week (not at all, a little, quite a bit and very much). All domain and single-item raw scores are linearly transformed to a scale of 0–100. 13 Higher scores on functional domains and global health status/quality of life scale represent higher functioning and higher HRQoL. Lower scores on symptom domains and single items represent less symptoms. 11,13 The EORTC-QLQ-C30 core questionnaire has strong test–retest reliability for the physical function (PF) domain (r = 0.91) 14 and is responsive to change from pretreatment to during cancer treatment. 11,12
Change in the PF domain of the EORTC-QLQ-C30 core questionnaire was used as an anchor to determine whether participants felt that there had been improvement, deterioration or no change in their PF between time points of testing. Change in the PF domain of five or more points is considered clinically relevant. 15
Additional measures completed at both time points include function, distress and physical activity, for example, function was rated by both the physician and participant using the Eastern Cooperative Oncology Group Performance Status (ECOG-PS). 16 The ECOG-PS is a six-point scale that rates an individual’s level of PF from zero (fully active) to four (bedridden) and five (death). 16 Distress was recorded using the distress thermometer, a modified 11-point visual analogous scale, which asks the participant to rate the distress they have been experiencing over the previous 7 days from 0 (no distress) to 10 (extreme distress). 17 Information regarding the participants’ engagement in physical activity was recorded using the using the Physical Activity Scale for the Elderly (PASE). 18 The PASE asks participants to recall their physical activities from the previous 7 days. Higher scores represent higher levels of physical activity. The maximum score attainable is 400 and the average score for elderly individuals is 103 points. 18
Demographic and medical data were obtained, and co-morbidities were scored with the simplified Colinet co-morbidity score, where higher scores represent worse health status.
Statistical analysis
Data were analysed through Statistical Package for the Social Sciences (SPSS) Windows Version 21.0 (SPSS, Chicago, Illinois, USA). Data were assessed for normality using the Kolmogorov–Smirnov statistic. Descriptive statistics were used to summarize demographic and clinical characteristics and outcome data.
Participants were categorized into two groups (deteriorated and not-deteriorated) based on whether they had a change in the EORTC-QLQ-C30 PF domain between baseline and follow-up testing. Participants were classified as ‘deteriorated’ if they had a decrease in the PF domain of ≥5 points or ‘not-deteriorated’ if they had a decrease in the PF domain of <5 points. 15
Paired t tests were used to determine change in 6MWD, EORTC-QLQ-C30 PF domain and other variables between the two time points of measurement. Pearson’s χ 2 and independent samples’ t tests were used to assess the effects of gender, age (above vs. below 65 years), histological type, cancer stage, treatment type and baseline 6MWD (above vs. below 350 m) on change in 6MWD within the group of participants classed as deteriorated. Pearson correlations were used to assess the bivariate relationship between change in the 6MWD and change in the EORTC PF and other variables. Coefficients were interpreted as follows: little association = 0.00–0.25, fair association = 0.25–0.50, moderate association = 0.50–0.75 and large association = 0.75–1.0. 19 Alpha was set at 0.05 (two tailed) for analyses.
The MID was calculated using both anchor-based and distribution-based methods. For the anchor-based methods, the sensitivity and specificity for change in 6MWD to discriminate between participants who deteriorated versus remained not-deteriorated were calculated. A receiver operating curve was plotted for sensitivity (y-axis) versus 1 − specificity (x-axis) for each of the cut-off values. The optimal cut-off point was found objectively, as the point on the receiver operating curve nearest to the upper left corner of the graph. The 95% confidence interval (CI) for the optimal cut-off point was found using the bootstrap. 20 In each case, 999 bootstrap replicate samples were obtained, by resampling the deteriorated and not-deteriorated samples separately. For each replicate sample, the optimal cut-off point was obtained. The limits of the 95% CI were then taken to be the 2.5th and 97.5th percentiles, respectively, of the 999 cut-off points. Minitab Version 16 and some associated programming were used to carry out the bootstrapping. According to published recommendations, anchor-based estimations can be performed if correlations between change in 6MWD and change in anchors are >0.30, 21 however, correlations >0.50 are required for more robust estimates of the MID. 21
For the distribution-based methods, the standard error of the measurement (SEM) and effect size (ES) were calculated using the following formulas:
Results
Fifty-six participants with lung cancer were studied. Demographic characteristics are shown in Table 1. Twelve participants (21%) had stage I disease, 6 participants (11%) had stage II disease, 27 participants (48%) had stage III disease and 11 participants (20%) had stage IV disease (Table 1). At baseline, the 6MWD ranged from 246 m to 603 m. All participants completed the baseline and follow-up 6MWD; however, three participants were missing EORTC-QLQ-C30 data at follow-up (these three individuals were excluded from the anchor-based estimation of MID). Refer to Supplementary Table S1 for baseline EORTC-QLQ-C30 data.
Baseline demographic and clinical characteristics.

PASE: Physical Activity Scale for the Elderly; 4WF: four-wheel frame; BMI: body mass index; chemo: chemotherapy; IQR: inter-quartile range; M: mean; RT: radiotherapy; SPS: single-point stick; PF: physical function; ECOG: Eastern Cooperative Oncology Group.
aGrouped according to deterioration or not-deterioration in the PF domain score over time. Missing data on repeated PF domain scores for n = 3.
Anchor-based estimation of the minimal importance difference
There was a mean decline in the 6MWD from baseline to follow-up of 43 m (95% CI −60 to −26). The change in 6MWD was highly variable, ranging from a deterioration of 267 m to an improvement of 130 m. At follow-up, the mean (SD) change in percentage of baseline walking distance achieved was −9.9 ± 16% and ranged from −68% (deterioration) to 53% (improvement).
The EORTC-QLQ-C30 PF domain indicated that at follow-up 30 participants (57%) had deteriorated and 23 participants (43%) had not deteriorated (Figure 1). The baseline demographics of these two groups are shown in Table 1. The correlation between change in 6MWD and change in the EORTC-QLQ-C30 PF domain was −0.57 (p < 0.0001; Figure 2). The mean decline in 6MWD in participants classed as deteriorated was 60 m compared with a mean decline of 16 m in participants classed as not-deteriorated (p = 0.01; Figure 1). The mean percentage decline in 6MWD in participants classed as deteriorated was 14% compared with a mean percentage decline of 3% in participants classed as not-deteriorated (p = 0.01). In participants classed as deteriorated, there was no difference in the magnitude of 6MWD decline in terms of gender (p = 0.42), age (p = 0.59), histological type (p = 0.66), cancer stage (p = 0.22) or treatment type (p = 0.23). There was a trend for participants classed as deteriorated, who had baseline 6MWD below 350 m, to experience less decline (in both actual distance and percentage of baseline distance) than those participants classed as deteriorated but had a baseline 6MWD of 350 m or more, although this difference was not statistically significant (mean difference between groups −45 m, 95% CI −108 to −18, p = 0.152).

Change in 6MWD from baseline to follow-up, grouped according to change in EORTC QLQ-C30 PF domain, such as data, means and 95% CIs are shown. 6MWD: 6-minute walk distance; EORTC QLQ-C30: European Organization for Research and Treatment of Cancer questionnaire; CI: confidence interval.
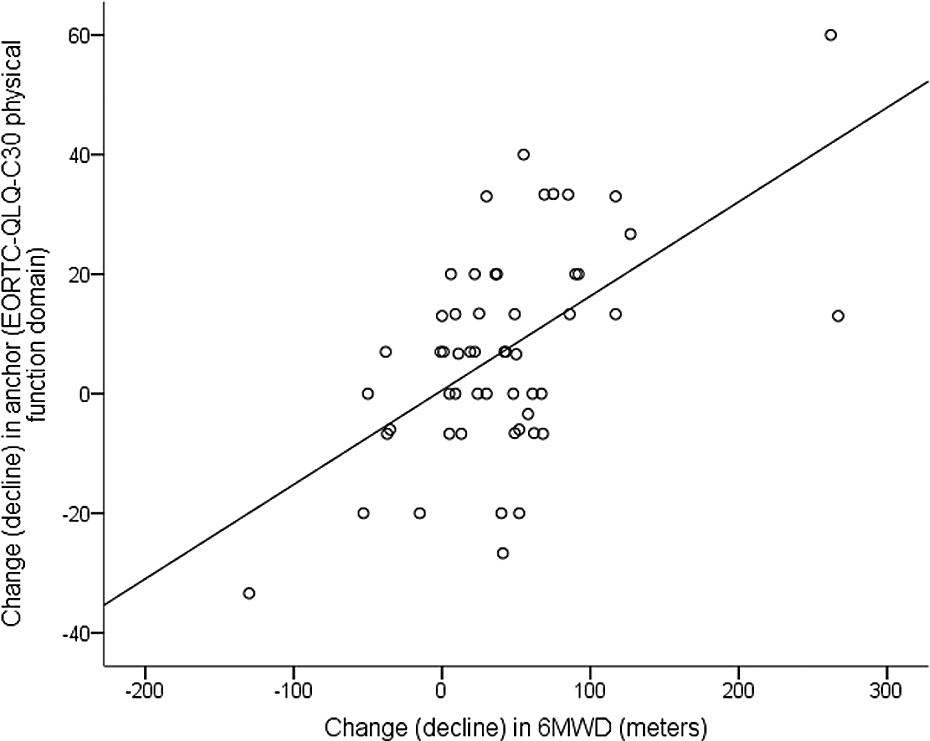
Change in 6MWD and anchor from baseline to follow-up. 6MWD: 6-minute walk distance; EORTC-QLQ-C30, European Organization for the Research and Treatment of Cancer questionnaire.
The receiver operating curve indicated an optimal cut-off value for clinically relevant decline to be 42 m (bootstrap 95% CI 6–75) (area under curve 0.66, 95% CI 0.51–0.81; Figure 3). This represents a sensitivity of 0.53 and specificity of 0.61. The receiver operating curve indicated a cut-off value for clinically relevant decline to be 9.5% of baseline walking distance (area under curve 0.66). This represents a sensitivity of 0.60 and specificity of 0.61.
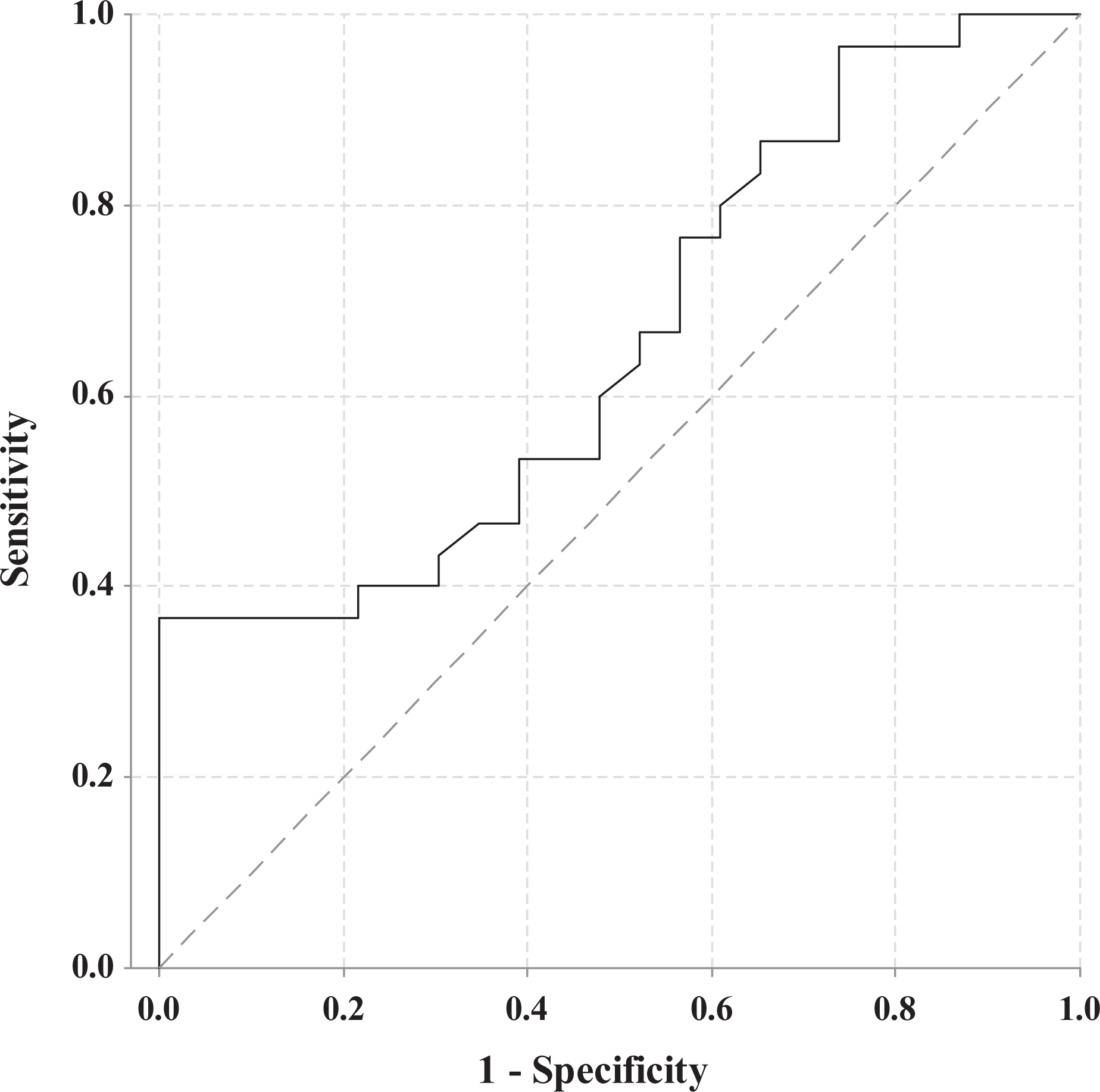
Receiver operating curve of deterioration versus no deterioration in the 6MWD metres. 6MWD: 6-minute walk distance.
Distribution-based estimation of the minimal importance difference
Distribution-based methods indicated an MID between 22 m (bootstrap 95% CI 18–26) and 32 m (bootstrap 95% CI 20–42) using SEM and ES, respectively.
Relationship between 6MWD, demographic and disease-related factors
A greater 6MWD at baseline correlated with better ECOG function (r = −0.42, p = 0.001), better EORTC PF (r = 0.47, p < 0.0005), better cognitive function (r = 0.28, p = 0.43), higher physical activity levels (r = 0.56, p < 0.005) and less dyspnoea (r = −0.44, p = 0.001). There was no relationship between baseline 6MWD and cancer stage, smoking pack-year history or co-morbidities. There was a small relationship between greater deterioration in the 6MWD and worse co-morbidities (r = 0.26, p = 0.049) and greater arm pain (r = 0.34, p = 0.01) at baseline; all other associations with change in the 6MWD were r < 0.25.
Discussion
This exploratory study has estimated the MID for deterioration of the 6MWD in lung cancer to be between 22 m and 42 m, or a change of 9.5%. This finding (22–42 m) is consistent with the MID established in other chronic respiratory disease populations 9,10 and supports the historic use of the 25–35 m MID (established in COPD) to interpret change in the 6MWD in patients with lung cancer.
Direction of change in the 6MWD may have an important influence on the MID. 23 The majority of the literature establishing the MID for the 6MWD in chronic respiratory disease have used interventional study designs that aim to improve patient outcomes. 9,10 Our study is unique in that we used an observational study design, did not provide exercise intervention to participants and monitored clinical deterioration of the participant. Given the significant and rapid physical decline that occurs in lung cancer, even over a period of 10 weeks, 3 we were able to use deterioration in the 6MWD for determination of the MID. A similar strategy was used by Polkey and colleagues 24 who determined an annual deterioration of 30 m in the 6MWD is the MID associated with death in COPD. Very few studies have utilized decline as a measure of MID in patients with chronic respiratory disease. 24,25 Decline is important to patients and may be perceived differently to improvement. 24 Because deterioration may occur gradually and is not anchored in time by a perceived beneficial intervention, it may be that a larger change in functional capacity is required for patients to detect decline compared with improvement. It is well documented that after a cancer diagnosis HRQoL shifts over time, and this response shift is associated with alterations of patients’ personal expectations. However, this study did not find evidence of a reduction in patients’ sensitivity to decline in 6MWD, as our MID estimates were consistent with those from previous studies that evaluated improvement from the COPD literature. 9,10 Further research is required to investigate whether the MID for deterioration in the 6MWD is the same as the MID for improvement in the lung cancer population.
There is controversy within the literature as to which is the best method to determine the MID. Anchor-based estimation of MID utilizes a patient-related anchor, commonly a questionnaire (with an established MID) or a global rating of change scale, to determine whether the patient is clinically changed. In our study, we used the EORTC-QLQ-C30 HRQoL questionnaire that is commonly used in lung cancer exercise trials 5 and has established evidence regarding the MID for the PF domain. 15 The correlation between change in the 6MWD and the anchor (PF domain) was >0.50 informing with confidence that anchor-based analyses were appropriate. 21 Anchor-based approaches are potentially more clinically relevant as the patients’ and or clinicians’ opinion is measured and utilized as an anchor in order to determine whether the patient has actually changed. The disadvantage of this method is that there can be a large amount of individual variation amongst patients 8 and this was the case in the lung cancer cohort in this study. In addition, anchor-based methods cannot account for the measurement error of the test. 8 Distribution-based methods on the other hand utilize statistical analyses to determine the MID using the degree of variability (standard deviation) of the test scores. However distribution-based methods do not take into account whether or not the patient or clinician feel the change is clinically relevant. 26 For the above reasons, we calculated the MID in this study using both anchor- and distribution-based methods and found similar results. Consistencies in anchor-based and distribution-based MIDs for the 6MWD are commonly reported in the chronic respiratory disease literature. 9
Our results provided further evidence that the 6MWD is a useful test in lung cancer. A number of studies have demonstrated the criterion predictive validity of the 6MWD in lung cancer, with reports demonstrating that better performance on the 6MWD is associated with better post-operative outcomes, 27 shorter post-operative length of hospital stay, 28 better post-operative HRQoL 27 and improved survival. 29,30 In stage IV NSCLC, the 6MWD has been shown to predict survival. 29,30 In contrast, there is relatively little information about the construct validity of the 6MWD in lung cancer; our study addresses this literature gap in that we have shown that the 6MWD is moderately associated with symptoms, function and physical activity levels in lung cancer.
Limitations
This study was limited by a small sample size, and the findings are exploratory in nature and need to be confirmed in a larger sample. The study is limited by a heterogeneous group of participants and variability in participant deterioration. The cohort included participants with all stages of lung cancer and a variety of treatment regimens. It is possible that the MID for the 6MWD for individuals with early stage resectable lung cancer may be different to the MID for individuals with advanced palliative disease. Further research is required to investigate whether the 22–42 m MID is stable when more homogenous lung cancer subgroups are studied. External validation of these values is also required.
The MID established with anchor-based methods should be utilized with caution given the fact that the area under the receiver operating curve was less than 0.7, the general cut-off for adequate results and the sensitivity and specificity was low. 19 This may be due to the heterogeneous nature of the cohort studied. In addition, the fact that deterioration was used to estimate the MID rather than improvement may have contributed to the variability of participant change and resulting receiver operating curve. Research is required to determine whether the MID for deterioration is the same as the MID for improvement and hence the MID reported should not be applied for patient improvement until this is confirmed.
This study reports a MID range for lung cancer because of the lack of strong concordance between the distribution-based and anchor-based values. Reliability data for calculation of the MID using distribution-based methods were used from the COPD literature; future research is required to confirm whether the reliability coefficient used is the same for the lung cancer population.
The MID for deterioration of the 6MWD in lung cancer is estimated to be between 22 m and 42 m or a change of 9.5%. This is similar to the MID previously established for other chronic respiratory disease populations. Further external validation is required in a larger cohort.
Footnotes
Acknowledgements
The authors would like to thank Selina Parry, Christine McDonald, Louis Irving, Linda Mileshkin, Meinir Krishnasamy, Andrew Murnane; the staff of the Royal Melbourne Hospital, Peter MacCallum Cancer Centre and Austin Hospital; and the participants for their contribution to the study.
Conflict of interest
The authors declared no conflicts of interest.
Funding
This work was supported in part by the Pat Cosh Trust (grant number 2012). Dr Granger is supported, in part, by a National Health and Medical Research Council Translating Research Into Practice Fellowship, Australia.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.