
Abstract
The aims of the study were to evaluate the responsiveness of Hospital Anxiety and Depression Scale-Anxiety (HADS-A) subscale and HADS-Depression (HADS-D) subscale to pulmonary rehabilitation (PR) in patients with bronchiectasis compared to a matched group of patients with chronic obstructive pulmonary disease (COPD) and provide estimates of the minimal clinically important difference (MCID) of HADS-A and HADS-D in bronchiectasis. Patients with bronchiectasis and at least mild anxiety or depression (HADS-A ≥ 8 or/and HADS-D ≥ 8), as well as a propensity score-matched control group of patients with COPD, underwent an 8-week outpatient PR programme (two supervised sessions per week). Within- and between-group changes were calculated in response to PR. Anchor- and distribution-based methods were used to estimate the MCID. HADS-A and HADS-D improved in response to PR in both patients with bronchiectasis and those with COPD (median (25th, 75th centile)/mean (95% confidence interval) change: HADS-A change: bronchiectasis −2 (−5, 0), COPD −2 (−4, 0); p = 0.43 and HADS-D change: bronchiectasis −2 (−2 to −1), COPD −2 (−3 to −2); p = 0.16). Using 26 estimates, the MCID for HADS-A and HADS-D was −2 points. HADS-A and HADS-D are responsive to PR in patients with bronchiectasis and symptoms of mood disorder, with an MCID estimate of −2 points.
Keywords
Introduction
Bronchiectasis is characterised by abnormal and permanent bronchial dilation and symptoms of dyspnoea, productive cough and recurrent chest infections. 1 Mental illness, such as anxiety and depression, affect a significant proportion of patients with bronchiectasis 2 with prevalence estimates ranging from 31% to 55% and 14% to 34% for anxiety and depression, respectively. 2 –5 Assessment and management is important in bronchiectasis as high levels of anxiety and depression are associated with lower health-related quality of life. 5
Pulmonary rehabilitation (PR) is recommended for patients with this disease 1,6,7 as it is associated with improvements in exercise capacity 8 –12 and health-related quality of life, 8,10 –12 reduced exacerbation rates and prolonged time to first exacerbation. 8 In other chronic respiratory diseases, for example, chronic obstructive pulmonary disease (COPD), PR is also associated with a reduction in symptoms of anxiety and depression. 13 However, to date, there is limited data on the effects of PR on anxiety and depression in patients with bronchiectasis, particularly in those with existing psychological comorbidity. 8
The Hospital Anxiety and Depression Scale (HADS) is a self-administered questionnaire used to screen for the presence of mood disorder. 14 It consists of two subscales: HADS-Anxiety (HADS-A) and HADS-Depression (HADS-D). For both subscales, a score of 0–7 is considered in the normal range, 8–10 is suggestive of mood disorder and a score ≥11 indicates probable mood disorder. 15 The HADS is widely used as an outcome measure in PR studies. 16 The minimal clinically important difference (MCID) of HADS in bronchiectasis has not been described.
The primary aim of this study was to determine the responsiveness of HADS-A and HADS-D to PR in patients with bronchiectasis and increased symptoms of anxiety and depression, and to compare these responses with those observed in a matched group of COPD patients undergoing the same PR programme. The secondary aim of the study was to provide MCID estimates for HADS subscales in patients with bronchiectasis.
Methods
Study participants
Participants with bronchiectasis were prospectively recruited from the Harefield PR Unit (UK) between September 2012 and April 2017 and were participating in studies approved by London-Camberwell St. Giles (11/LO/1780) and London-Central (13/LO/1161) Research Ethics Committees and registered on clinicaltrials.gov (NCT01649193, NCT02261337). All participants provided written informed consent to participate in these studies.
Inclusion criteria were: (1) a primary diagnosis of non-cystic fibrosis bronchiectasis, determined by a respiratory physician from the Royal Brompton and Harefield NHS Foundation Trust, with supporting evidence from thin-section computed tomography of bronchial dilatation (internal airway lumen greater than adjacent pulmonary artery; absence of tapering; airway visibility within 1 cm of pleural surface) 17 (experimental group) or COPD, according to GOLD guidelines (control group); (2) HADS-A and/or HADS-D score ≥8 (this cut-off is suggestive of the presence of a mood disorder) 15 ; (3) ability to walk 5 m; (4) referred for PR in line with the British Thoracic Society Quality Standards for PR 18 ; and (5) ability to provide informed consent. Participants were excluded if they had significant co-morbidities that were the primary limitation to walking (e.g. lower limb amputation) or conditions that made exercise unsafe (e.g. unstable ischaemic heart disease). In the bronchiectasis group, to avoid possible contamination with coexisting COPD, patients with a coexisting diagnosis of COPD or a self-reported smoking history of ≥10 pack-years were excluded.
Study design
In this matched observational cohort study, patients in the experimental and control groups were enrolled in an 8-week outpatient PR programme at Harefield Hospital as described previously. 19 Of note, the education programme included a session on psychological wellbeing delivered by a clinical psychologist (described in the Online Supplement). Completion of PR was defined as attending a minimum of eight sessions (50%) and the post-PR assessment.
Anthropometry, spirometry, Medical Research Council (MRC) Dyspnoea score, Incremental Shuttle Walk (ISW) test, HADS and Chronic Respiratory Questionnaire (CRQ) were completed in the weeks before and after the PR programme. Participants were also asked to respond to the following question: ‘How do you feel your overall condition has changed after rehabilitation?’ using a five-point Global Rating of Change Questionnaire (GRCQ). The scale ranged from ‘1: I feel much better’ to ‘5: I feel much worse’.
Patients with bronchiectasis were propensity score-matched 1:1 20 with a control group of patients with COPD, accounting for age, gender, forced expiratory volume in one second (FEV1) per cent predicted, MRC Dyspnoea score, ISW and HADS.
Statistical analysis
Responses to PR were analysed and presented separately for those with HADS-A ≥8 and HADS-D ≥8 with the same analysis methods used for both subscales. Estimation of the MCID was calculated in the bronchiectasis cohort only. Only data from patients that completed PR were included in the analyses.
The baseline characteristics were presented as mean (standard deviation) or median (25th, 75th centile) for continuous data and number (per cent) for categorical data. Paired t-test (or Wilcoxon Signed Rank test for non-parametric data) was used to compare within-group response to PR and two-sample t-test (or Mann–Whitney U test for non-parametric data) for between-group response to PR. The relationship between change in HADS subscale score and change in other outcome measures (ISW, CRQ, MRC) was assessed using Pearson’s Correlation Co-efficient (or Spearman’s Rank-Order Correlation for non-parametric data).
MCID analysis
Multiple anchor- and distribution-based approaches were used to estimate the MCID of HADS subscales. The a priori criteria for determining the validity of an external anchor were a statistically significant correlation (p < 0.05) and a correlation coefficient >0.3 between the subscale and the external anchor. 21 For external anchors fulfilling these criteria, linear regression was used to estimate a change in HADS subscale score based on the MCID for each anchor, for example, MRC: −1, ISW: 47.5 m, CRQ-Dyspnoea: 2.5, CRQ-Fatigue: 2, CRQ-Emotion: 3.5, CRQ-Mastery: 2 and CRQ-Total: 10. Additionally, receiver operating characteristic (ROC) curves were used to identify the change in HADS subscale cut-off with equal sensitivity and specificity that best discriminated between those who did and did not achieve the MCID of the external anchor. 22 The MCID was also estimated using the mean change in HADS subscale in patients who reported ‘2: I feel a little better’ on the GRCQ following PR. 23 The distribution-based methods used to estimate the MCID of HADS-A and HADS-D were Cohen’s effect size (half of the standard deviation of change 24 ) and the Empirical rule effect size (0.08 × 6 × standard deviation of change 24 ). Data analyses were performed using GraphPad Prism 7 (GraphPad Software, La Jolla, California, USA) and SPSS version 24 (IBM, New York, USA). Statistical significance was considered at p < 0.05.
Results
HADS-A: Baseline characteristics and response to PR
In total, 86 patients fulfilled the inclusion criteria for the HADS-A analysis, of which 62 (70%) completed PR. Only two were on existing medication for their mood disorder. Data was analysed from a matched control group of 62 patients with COPD and HADS-A ≥8 that completed PR during the same period. Baseline characteristics are presented in Table 1. The two groups were successfully matched at baseline and the only between-group differences were a lower smoking prevalence and pack-year history as well as a higher FEV1/FVC ratio and number of hospitalisations in the bronchiectasis cohort.
Baseline characteristics of patients with bronchiectasis (n = 62) and COPD (n = 62) with HADS-A ≥8.a

BMI: body mass index; CRQ: Chronic Respiratory Questionnaire; FEV1: forced expiratory volume in one second; FVC: forced vital capacity; HADS: Hospital Anxiety and Depression Scale; ISW: Incremental Shuttle Walk test; MRC: Medical Research Council; COPD: chronic obstructive pulmonary disease; HADS-A: Hospital Anxiety and Depression Scale-Anxiety.
a Continuous data reported as mean (standard deviation) or median (25th, 75th centile) and categorical data reported as number (per cent).
Table 2 presents the response to PR. Significant improvements in HADS, MRC, ISW and CRQ were observed in both groups. The magnitude of change observed were similar to or exceeded the commonly accepted MCID of HADS, ISW and CRQ in COPD. Of note, 45% of the bronchiectasis group shifted to a normal anxiety state (HADS-A < 8) after PR. No significant between-group differences were observed in change in MRC, ISW or CRQ. Furthermore, a similar proportion of patients in the bronchiectasis (97%) and COPD (94%) groups reported feeling ‘much better’ or ‘a little better’ following PR.
Response to pulmonary rehabilitation in participants with bronchiectasis and HADS-A ≥ 8 (n = 62) compared to participants with COPD and HADS-A ≥8 (n = 62).a

BMI: body mass index; CRQ: Chronic Respiratory Questionnaire; GRCQ: Global Rating of Change Questionnaire; HADS: Hospital Anxiety and Depression Scale; ISW: Incremental Shuttle Walk test; MRC: Medical Research Council; COPD: chronic obstructive pulmonary disease; HADS-A: Hospital Anxiety and Depression Scale-Anxiety.
a Baseline data reported as mean (standard deviation) or median (25th, 75th centile) unless otherwise stated. Response to pulmonary rehabilitation data reported as mean (lower 95% confidence interval to upper 95% confidence interval) change or median (25th, 75th centile) change.
HADS-A: MCID estimation in bronchiectasis
The correlation between change in HADS-A and change in CRQ-Emotion (r value; p value: −0.42; <0.01), CRQ-Mastery (−0.40; <0.01) and CRQ-Total (−0.50; <0.001) met the a priori criteria for determining the validity of an external anchor (r > 0.3 and p < 0.05), and consequently these variables were used in the anchor-based methods to determine the HADS-A MCID. There was no significant correlation between change in HADS-A and change in MRC, ISW, CRQ-Dyspnoea or CRQ-Fatigue.
The MCID estimates for HADS-A in patients with bronchiectasis and symptoms of anxiety calculated using linear regression and ROC plots ranged from −3 to −2 (see Table S1 in the Online Supplement). For those who reported feeling ‘a little better’ on the GRCQ, the mean change in HADS-A was −2. Using distribution-based methods the MCID estimate calculated with Cohen’s effect size and the Empirical rule effect size was −2. Giving equal weighting to each method of MCID estimation, the mean (range) MCID for HADS-A was −2 (−4 to −1).
HADS-D: Baseline characteristics and response to PR
A total of 68 patients fulfilled the inclusion criteria for the HADS-D analysis, of which 50 (74%) completed PR. Only three were on existing medication for their mood disorder. Data were analysed from a matched control group of 50 patients with COPD and HADS-D ≥8 that completed PR during the same period. Baseline characteristics are described in Table 3. Similar to HADS-A, the two groups were successfully matched and the only between-group differences at baseline were a lower smoking prevalence, pack-year history and number of hospitalisations in the bronchiectasis group.
Baseline characteristics of patients with bronchiectasis (n = 50) and COPD (n = 50) with HADS-D ≥8.a

BMI: body mass index; CRQ: Chronic Respiratory Questionnaire; FEV1: forced expiratory volume in one second; FVC: forced vital capacity; HADS: Hospital Anxiety and Depression Scale; ISW: Incremental Shuttle Walk test; MRC: Medical Research Council; COPD: chronic obstructive pulmonary disease; HADS-D: Hospital Anxiety and Depression Scale-Depression.
a Continuous data reported as mean (standard deviation) or median (25th, 75th centile) and categorical data reported as number (per cent).
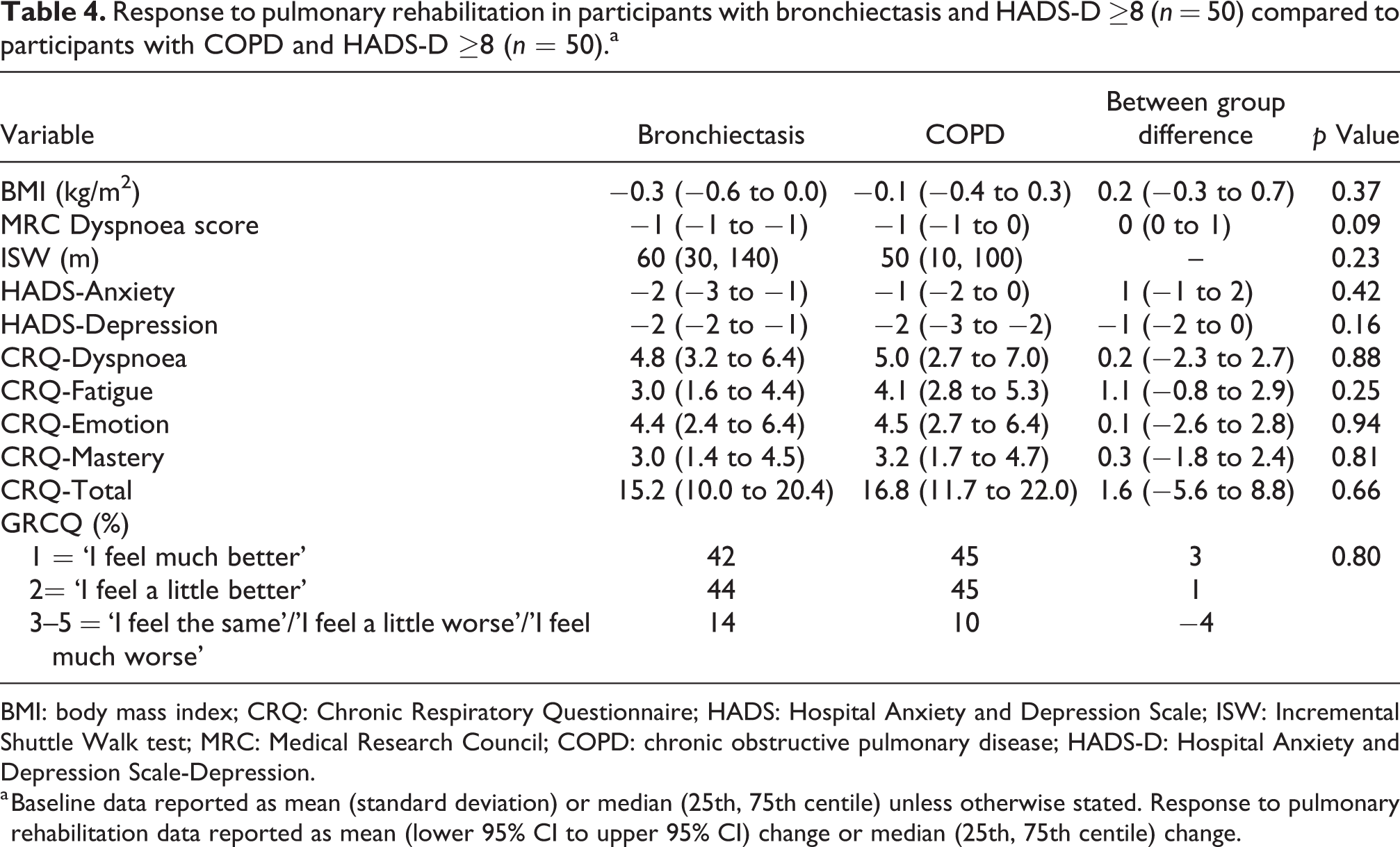
Table 4 demonstrates the response to PR. Significant within-group improvements in HADS, MRC, ISW and CRQ were observed in both groups with the MCID of these variables achieved or exceeded in all cases. A total of 40% of the bronchiectasis group shifted to a normal depression state (HADS-D < 8) after PR. Furthermore, there were no significant between-group differences and 86% and 90% of bronchiectasis and COPD patients, respectively, reported feeling ‘a little’ or ‘much better’ following PR.
Response to pulmonary rehabilitation in participants with bronchiectasis and HADS-D ≥8 (n = 50) compared to participants with COPD and HADS-D ≥8 (n = 50).a
BMI: body mass index; CRQ: Chronic Respiratory Questionnaire; HADS: Hospital Anxiety and Depression Scale; ISW: Incremental Shuttle Walk test; MRC: Medical Research Council; COPD: chronic obstructive pulmonary disease; HADS-D: Hospital Anxiety and Depression Scale-Depression.
a Baseline data reported as mean (standard deviation) or median (25th, 75th centile) unless otherwise stated. Response to pulmonary rehabilitation data reported as mean (lower 95% CI to upper 95% CI) change or median (25th, 75th centile) change.
HADS-D: MCID estimation in bronchiectasis
The correlation between change in HADS-D and change in ISW (r value; p value: −0.38; 0.01), CRQ-Dyspnoea (−0.41; <0.01), CRQ-Fatigue (−0.41; 0.01), CRQ-Emotion (−0.42; <0.01), CRQ-Mastery (−0.40; <0.01) and CRQ-Total (−0.50; <0.001) met the a priori criteria for determining the validity of an external anchor (r > 0.3 and p < 0.05) and were used to determine the HADS-D MCID in the anchor-based analyses. There was no significant correlation between change in HADS-D and change in MRC Dyspnoea score.
The MCID estimates for HADS-D in patients with bronchiectasis, and symptoms of depression calculated using linear regression and ROC plots ranged from −2 to −1 (see Table S2 in the Online Supplement). For those who reported feeling ‘a little better’ on the GRCQ, the mean change in HADS-D was −1. The MCID estimates were −2 and −1 for Cohen’s effect size and Empirical rule effect size, respectively. Giving equal weighting to each method of MCID calculation, the mean (range) MCID estimate for HADS-D was −2 (−3 to 1).
Dual symptoms of mood disorder in bronchiectasis
In the HADS-A cohort, 36 (58%) of patients who scored ≥8 HADS-A also scored ≥8 HADS-D. Similarly, in the HADS-D group, 36 (72%) of patients who scored ≥8 HADS-D also scored ≥8 HADS-A. The response to PR in these patients with dual symptoms of anxiety and depression was similar to those with symptoms of anxiety only (≥8 HADS-A and <8 HADS-D; n = 26) or depression only (≥8 HADS-D and <8 on HADS-A; n = 14). These data are outlined in Tables S3 and S4 in the Online Supplement. Furthermore, the MCID in the sub-groups of patients with dual symptoms of mood disorder was similar to the estimates in those with a single mood disorder symptom.
Discussion
This is the first study to establish that HADS is responsive to PR in patients with bronchiectasis and probable anxiety or depression. We also demonstrated that the magnitude of HADS response to PR in patients with bronchiectasis was similar to that observed in a matched COPD cohort. Mean MCID estimates of HADS-A and HADS-D in bronchiectasis were −2.
Comparison to previous studies
HADS is a self-administered questionnaire used to screen for mood disorder 14 and is widely used in PR. 16,25 Previous studies have shown that HADS is reliable, 14 valid 14,15 and responsive to intervention 26 –30 in other chronic respiratory diseases. In COPD, MCID estimates range from −1.8 to −1.3 for HADS-A and −1.7 to −1.4 for HADS-D. 26,28 However, limited data exist on the responsiveness of HADS in patients with bronchiectasis.
To the best of our knowledge, only one study has explored the effects of an exercise-training programme on HADS in bronchiectasis. 8 Lee et al. compared the effects of an 8-week exercise programme and airway clearance technique review to airway clearance technique review alone. 8 The authors were unable to show that symptoms of mood disorder improved with either intervention. However, the patients had low levels of psychological symptom burden at baseline (mean HADS-A < 5, HADS-D < 4). 8 In contrast, we purposefully enriched our study with patients at risk of anxiety and depression (inclusion criteria: HADS ≥ 8), and consequently demonstrated a more marked improvement with PR.
Another explanation for the contrasting HADS responses between the current study and the study by Lee et al. include differences between the interventions. Whereas Lee et al.8 used an intervention largely focused around exercise-training, our intervention incorporated an education/self-management component, in line with the recommendations of the British Thoracic Society guidelines. 6 This included a structured education session on psychological wellbeing by a clinical psychologist. PR is a complex, multi-component intervention, and it is plausible that non-exercise components or a synergy between exercise and education had a more substantial effect upon psychological symptom burden than exercise-training alone.
The magnitude of improvement in HADS scores observed in our bronchiectasis and COPD cohorts were similar, and in turn, comparable to previously published data in PR interventions in patients with COPD and interstitial lung disease (ILD) (range of mean changes in HADS-A: COPD: −2.0 to −1.7 13,26,28 , ILD: −2.0 to −1.6 27,29 and range of mean changes in HADS-D: COPD: −2.4 to −1.7 13,26,28 , ILD: −2.0 to −1.0 27,29 ). This provides a degree of reassurance about the validity and generalisability of the results of our study.
Although HADS MCID has not been published in patients with bronchiectasis, MCID estimates have been reported in COPD undergoing PR 26 and a 3-week inpatient respiratory rehabilitation programme. 28 These estimates were comparable to our study (MCID range: HADS-A: our study −2, COPD studies −1.8 to −1.3 26,28 and HADS-D: our study −2, COPD studies −1.7 to −1.4). 26,28 However, it was not possible to compare the uncertainty in the magnitude of MCID estimates of our data with previously published studies as confidence intervals were not available. The 95% confidence interval range for HADS-A and HADS-D MCID estimates was −4 to 1 and −3 to 1, respectively. This suggests some uncertainty in the precision of the MCID estimate and future larger studies are needed.
Strengths
There are several strengths to this prospective study. It provides new knowledge on the psychometric properties of HADS in patients with bronchiectasis and symptoms of mood disorder by demonstrating its responsiveness to intervention and providing MCID estimates. The capacity of an outcome measure to detect improvement is an important aspect of concurrent validity and is necessary for data interpretation in clinical and research settings. 21 This is facilitated by the MCID which enables the assessor to understand the clinical significance of data and forms an important part of the evidence required by regulatory agencies for approval for use in clinical trials. These properties are essential traits in an outcome measure and accordingly HADS has potential as a measure of mood disorder in patients with bronchiectasis.
Another strength was the careful identification of patients with bronchiectasis alone, with exclusion of coexisting COPD or those with significant smoking pack-year history. The control group were carefully matched patients with COPD using a formal validated statistical technique (propensity score matching) to minimise imbalance in key covariates between the groups.
Limitations
There were some limitations to our study. First, as participants were symptomatic outpatients referred to PR, our findings require corroboration in other settings and bronchiectasis populations. Second, due to the nature of the study investigating change in HADS, we performed a completer analysis (i.e. those completing PR with both before and after PR data). We are unable to generalise our findings to patients with bronchiectasis who fail to be referred for or fail to complete PR as well as those with bronchiectasis and other coexisting respiratory diseases. Third, because we enriched our population with a fixed inclusion cut-off in HADS score, there is a risk that we overestimated the effect size due to regression to the mean. However, we had a control group of patients with COPD and the changes in HADS, and our MICD estimates were similar to previously published values in COPD, 26,28 providing some reassurance on the validity of our results. Furthermore, for the calculation of the MCID, we used anchors that have a well-established MCID and so we believe that the risk of regression to the mean is partly mitigated. We intentionally chose to only include patients with probable anxiety or depression as our estimates might be underestimated otherwise (i.e. someone without depression is unlikely to become less depressed with pulmonary rehabilitation). It felt more logical and relevant to clinicians to report the effects of PR in patients with probable anxiety or depression.
Fourth, very few patients reported that they deteriorated; accordingly, these data estimate the MCID for improvement only. Further studies are required to assess whether patients perceive deterioration to a similar degree as improvement. Finally, as this was a short-term study, we were unable to comment on the long-term impact of PR on anxiety and depression, and we were unable to quantify whether participants received other treatments for mood disorder (e.g. medications and cognitive behavioural therapy) outside of the PR programme.
Significance of findings
This study demonstrates that the HADS is responsive to PR in patients with bronchiectasis and symptoms of anxiety or depression. We also provide the first estimates of the MCID for HADS-A and HADS-D in patients with bronchiectasis. This may be particularly useful in future clinical trials in patients with bronchiectasis, especially where a measure of anxiety or depression is being considered as an endpoint. For example, HADS was the primary endpoint in a recent randomised controlled trial of cognitive behavioural therapy versus self-help leaflets in patients with COPD. 31
In conclusion, HADS is responsive to PR in patients with bronchiectasis and symptoms of mood disorder, with a mean MCID estimate of −2 points for each subscale.
Supplemental material
Supplemental Material, HADS_MCID_online_supplement_clean_FINAL - Anxiety and depression in bronchiectasis: Response to pulmonary rehabilitation and minimal clinically important difference of the Hospital Anxiety and Depression Scale
Supplemental Material, HADS_MCID_online_supplement_clean_FINAL for Anxiety and depression in bronchiectasis: Response to pulmonary rehabilitation and minimal clinically important difference of the Hospital Anxiety and Depression Scale by Stephanie C Wynne, Suhani Patel, Ruth E Barker, Sarah E Jones, Jessica A Walsh, Samantha SC Kon, Julius Cairn, Michael R Loebinger, Robert Wilson, William D-C Man and Claire M Nolan in Chronic Respiratory Disease
Footnotes
Acknowledgements
The authors would like to express their gratitude to the patients who participated in this research and to Harefield Pulmonary Rehabilitation Unit for their role in delivering the interventions and help with data collection.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: CMN and JAW are supported by a NIHR Research for Patient Benefit Grant (PB-PG-0816-20022); SP is supported by a British Lung Foundation IPF Project Grant (IPFPG17-15); REB is supported by a NIHR Clinical Doctoral Research Fellowship (CDRF-2017-03-018); SJ is supported by a NIHR Doctoral Research Fellowship (DRF-2015-08-004); ML has received personal fees outside of this work from Bayer, Griffols, Astra Zeneca, Polyphor and Raptor; WM reports grants from National Institute for Health Research, during the conduct of the study; grants from Pfizer, non-financial support from GSK, personal fees from Mundipharma, personal fees from Novartis, personal fees from Jazz Pharmaceuticals, outside the submitted work.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.