
Abstract
Pulmonary rehabilitation (PR) is recommended for patients functionally restricted by chronic obstructive pulmonary disease (COPD). However, attendance and adherence to PR remains suboptimal. No previous research has explored COPD patient experiences during the key period from referral to initiation of PR in the United Kingdom. This research aimed to explore the lived experience of COPD patients referred to PR programmes prior to participation. COPD participants were recruited from referrals to two community PR programmes. Semi-structured interviews with COPD participants occurred following PR referral, but prior to programme initiation. Data were analyzed using applied interpretive phenomenology. Twenty-five COPD participants aged 42–90 were interviewed. ‘Uncertainty’ affected participants throughout their lived experience of COPD that negatively impacted illness perceptions, PR perceptions and increased participant’s panic and anger. Participants who perceived COPD less as a chronic condition and more as a cyclical process experienced fewer feelings of panic or anger. The experience of uncertainty was disabling for these COPD participants. Recognition of the role that uncertainty plays in patients with COPD is the first step towards developing interventions focused on reducing this uncertainty, thereby reducing the burden of the disease for the individual patient and facilitating PR attendance.
Introduction
Chronic obstructive pulmonary disease (COPD) is the third largest cause of mortality worldwide. 1 Furthermore, evidence suggests that one in four people will have COPD by the age of 80. 2 Pulmonary rehabilitation (PR) is recommended as a non-medical treatment option for people with COPD who are functionally disabled by their condition. 3 However, patients who could benefit from PR are not being referred to programmes and many of those who are referred do not attend or complete PR. 4 –6 Studies have investigated reasons for uptake, adherence, completion and non-completion of PR before and after patients attend PR. 7 –12 Themes from previous studies included the positive and negative influences of the referring practitioner to a PR programme and motivators and barriers to attendance and adherence to PR, such as patient transport, providing continued support or patients having competing commitments and demands. Nevertheless, PR attendance and adherence remain suboptimal. 4,5 Understanding patients’ experiences and motivations is key to designing PR programmes that will attract and retain patients for optimal benefit.
Bulley et al. 10 studied the perceptions of COPD patients after referral to PR. However, patients appeared to have already had clinical contact with PR staff. Therefore, their perceptions about their COPD and PR may have been different to those patients who had not yet had any clinical contact with a PR team. Furthermore, only severe and very severe COPD patients were included in the study and those with co-morbidities were excluded. This may not have reflected those who are referred in clinical practice. Knowledge is limited regarding the lived experience of COPD patients with a range of severities and co-morbidities, from the point after a referral has been made to a PR programme, but prior to the programme being started. It is possible that this period may hold the key to understanding subsequent attendance at the programme. Therefore, this study aimed to increase our understanding of COPD patient experiences of living with COPD and being referred to PR, from the point after referral to a PR programme to the point before programme participation.
Methods
The design of the study involved a qualitative inductive approach within a phenomenological framework using semi-structured interviews. Phenomenology enables exploration of people’s lived experiences in an embodied, temporal and interpretive process. 13 –16 It is a reflexive practice within which the role of the researcher is acknowledged and the researcher bias is explored. 16 –18 The methods were designed to answer the following research question:
What are the experiences and expectations of COPD and PR of patients with COPD who are referred to a PR programme, but have not yet started it?
Sample
A convenience sample of 25 patients with a diagnosis of COPD who had been referred to PR was recruited. Recruitment occurred at two sites on the South Coast of the United Kingdom. Both were community-based PR programmes (see Table 1 for a description of patient demographics). Inclusion criteria: patients who were referred to one of the two selected PR programmes; documented diagnosis of COPD. Exclusion criteria: previous participation in a PR programme; previous assessment for PR. Those patients who had already been clinically assessed for PR or who had previously participated in programmes were excluded because of the potential of those interventions changing participant’s experience and perceptions of COPD and PR. Of the 319 invitation letters sent out by the PR team administrative staff, 58 reply slips were received and 25 people agreed to take part in the study.
Participant demographic details.

GP: general practice.
Participants were aged between 42 and 90 years. Fourteen were male. There were seven smokers and two ‘never smokers’. The other 16 participants were ex-smokers. Nine participants lived alone and 21 participants were referred to PR from primary care via their surgery, general practice (GP) or practice nurse. Seven participants did not know who diagnosed their COPD. These details were obtained from a demographics form given to participants before their interview started and they were given the opportunity to provide open-ended answers. Further participant recruitment information is provided in Figure 1.
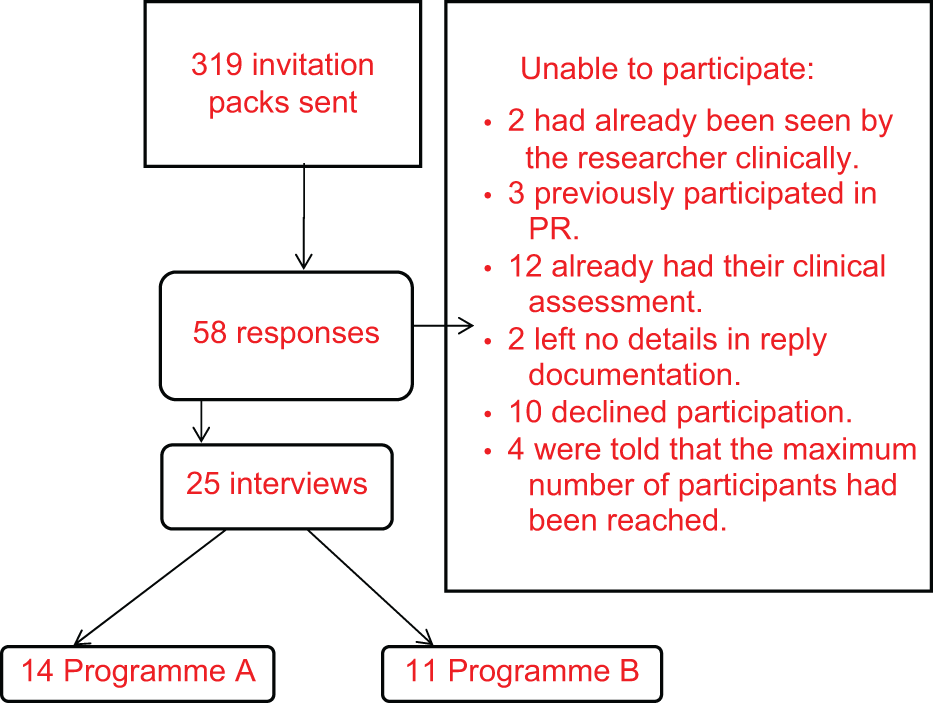
Participant recruitment information.
Data collection
Interviews were conducted after patients had been referred to PR, but before they attended for their first clinical assessment. Face-to-face interviews were carried out by the first author (AL) in participant homes or a university research facility between August 2009 and August 2010. Participants provided written consent on their interview day, and all interviews were audio recorded. Participants were aware that the interviewer was a postgraduate research student. The interviewer also worked as a physiotherapist in one of the teams in which participants were recruited but was not involved in their care during recruitment or known to any of the participants prior to study commencement. A sample of the interview questions is provided in Figure 2.
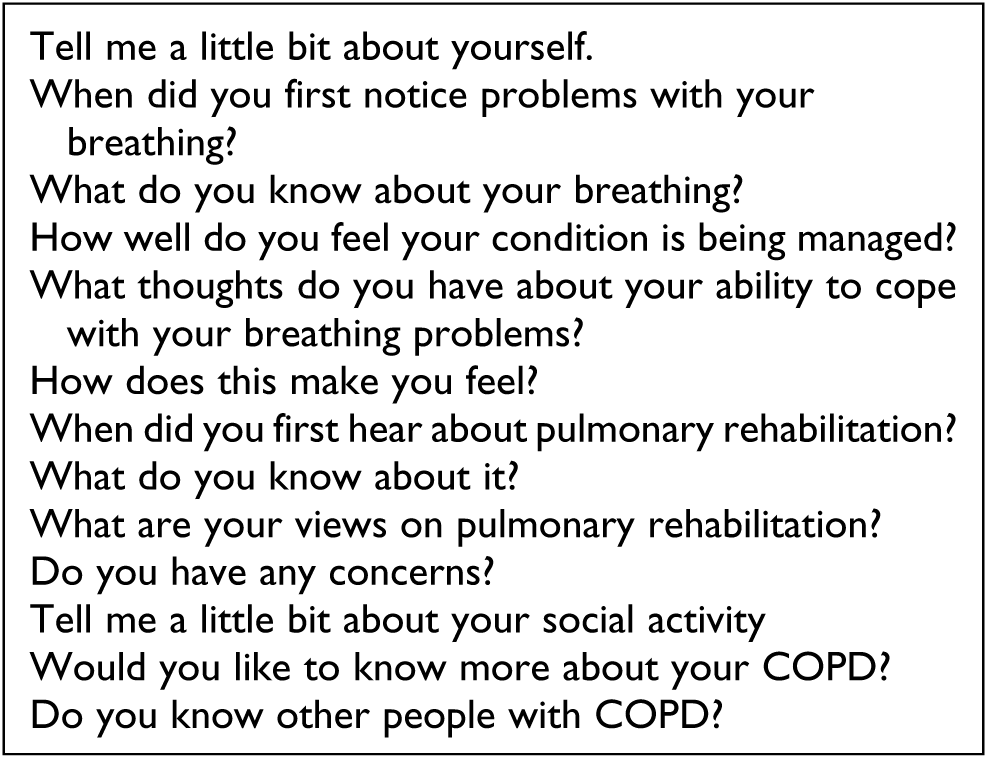
Sample interview questions.
Data analysis
Interviews were transcribed verbatim by the interviewer. This study was carried out within a phenomenological framework and involved carrying out several important steps to align the approach and explore researcher reflexivity. 15 –18 These included the creation of predicted participant responses to questions prior to interviewing participants. These responses were compared with the real participants’ responses to illuminate the researcher’s biases. Furthermore, a reflective account of each interview was written in order to provide a pathic analysis of the interview prior to transcript analysis. These stages enabled the researcher’s role within the research to be used as part of the analysis. Figure 3 is an excerpt from a reflective account of a participant’s interview:

Excerpt from a reflective account of a participant interview.
The analytical approach involved using applied interpretive phenomenology that uses a bricolage of phenomenological methodology influences that matched the research settings and researcher’s role and experience. 13 –18 Thematic statements were created from the transcript analysis of all of the interviews. Thematic statements were analyzed in context with the field notes for each participant and bias participant analysis in order to create themes. Themes of variance were explored 18 and continually discussed and reviewed among all three authors.
Ethical approval
Ethical approval was granted for this study by Southampton Research Ethics Committee prior to recruitment (Ethics no. 09/H0504/33)
Results
For these participants, uncertainty was the main overarching theme that affected their lived experience of COPD prior to starting PR. This uncertainty related to their lived experience temporally (i.e. related to their past, present and future). Participants also experienced uncertainty in their physical experience of COPD and relationships with others. Temporal uncertainty was the overarching theme most closely associated with participants’ journeys through primary care and the results of which are presented subsequently.
Temporal theme 1: Being in the past, being in the dark
Participants felt uncertainty during the development of their condition about what was happening to them. The responses below relate to participants’ understanding of what COPD is: “I don’t know what that means…Nothing at all…Always thought about my lung, not that tubes that go, so I know absolutely nothing…she never uh, nobody’s ever gone into the tubes to my lung…and I got a like an engineering logical brain that I could understand that, you know, but uh no I don’t know nothing about it.” (Keith, 79, lived alone, ex-smoker, unknown time since diagnosis (page 8, line 2)) “I have not got a clue, I’ve got no idea at all why it comes on and why it doesn’t you know…I can’t describe it, it’s just that your chest closes in and the, the thing I have got is uh, that caused this last bad bout, I’ve got bronchitis, and my, the bottom part of my right lung is clogged…I can’t see how they could diagnose it.” (Leonard, 77, lived with spouse, ex-smoker, diagnosed 18 months (page 1, line 40))
Leonard described the experience of breathlessness as one of the restrictions. He mentioned that he has got bronchitis which he felt was an acute condition for him.
Some participants did not believe that their disability was attributable to COPD, even though they acknowledged that they were receiving treatment for COPD. “I don’t know a lot about it at all, I really don’t. I know I had it, emphysema explained to me…but the COPD nobody has…they haven’t got time to explain it to you.” (Joe, 65, lived with spouse, smoker, diagnosed 14 years (page 27, line 16))
Joe described potential communication and patient education difficulties at the point of diagnosis. Joe’s uncertainty may have been related to the lack of information he perceived he received from his GP.
Temporal theme 2: Being in the present, being in limbo, ‘floating’ and panic
Uncertainty had a negative impact on participants’ perceptions of their COPD and their feelings about PR. Participants felt they were deteriorating whilst waiting for PR. Some developed pathophysiology perceptions that may have made them feel more disabled as a result. “Well, they, they reckon that it’s cos of the fluid in the bottom of me lung. It’s stale fluid. It never goes away, and same as the nurse was saying. If a germ gets into you then it, it causes, it’s like a piece of meat going off, you know. It’s alright for so long, but then once you know, it starts rotting away…Everything in the bottom half of the lung has gone…it will destroy the muscles in your lungs.” (Joe, 65, lived with spouse, smoker, diagnosed 14 years (page 36, line 15))
Some believed they were receiving second-class care because of their smoking status. Waiting for PR made them feel as if they were suspended or floating, and the waiting time to enter PR enhanced their feelings of uncertainty. “I thought you’re pissing me off now…the longer you’re floating with no treatment, no advice, no nothing, are you, are you making things worse like, are things getting worse? Have I lost something in that one year?” (Pauline, 59, lived with lodger and pets, ex-smoker, diagnosed 5 months (page 2, line 8))
Uncertainty was associated with fear, panic and awareness of the potential closeness of death, which affected these participants as much as their dyspnoea. “You get into a panic, you get to the stage is my next breath gonna be the last one?…thinking that I’m going to go to bed and not going to wake up.” (Nigel, 68, lived with spouse, ex-smoker, diagnosed 2 years (Page 12, line 1 onwards)) “The fear is only fear because it’s unknown.” (Leonard, 77, lived with spouse, ex-smoker, diagnosed 18 months. (page 12, line 1))
Some participants described the experience of breathlessness and panic as petrifying, where one could not have moved at all. Other participants controlled their feelings of panic or anger through relaxation and breathing techniques. “…if you feel one coming on just start breathing through your stomach gently…once you get over the scaredness of it, you get the freedom of it, of your breathing.” (Anne, 67, lived alone, ex-smoker, diagnosed 7 years. (page 18, line 43))
Anne’s ‘freedom’ related to her perceived benefit of overcoming her sense of fear through breathing techniques she learnt in hospital.
Some participants coped with uncertainty by perceiving their COPD as a temporary or a cyclical phenomenon. Richard felt that the ‘cold’ he had affected his health to the extent that objective measures of lung function were irrelevant. “I’ve got a heavy bronchial cold and they do a lung test and they tell me my lungs are 10 years older than they should be you know, why should I pay a lot of attention to it?” (Richard, 79, lived with daughter, ex-smoker, diagnosed 2 months (page 8, line 33))
The experience of uncertainty and being in limbo may have been highlighted because of the timing of the interviews within the participant’s journey into PR being on a wait list. This is seen as a justification of the study’s method because this experience of uncertainty has not previously been explored at such a time when uncertainty is so meaningful for these participants.
Temporal theme 3: Being in the future, PR as a ‘give it a go’ intervention
These participants showed uncertainty by expressing their ambivalence about the potential benefits of PR. “I’ll give anything a go you know. I’m not in the least bit (bothered).” (Elaine, 56, lived alone, smoker, diagnosed 1 year. (page 20, line 39)) “I’ll go and do it, which is free, I’ll go and try it…If it doesn’t work, then I’ll pack it in.” (Richard, 79, lived with daughter, ex-smoker, diagnosed 2 months. (page 9, line 3))
These examples illustrate a ‘give-it-a-go-but-not-convinced’ attitude towards PR. This may indicate a lack of commitment to PR, or an awareness of its potential value.
Discussion
Summary of main findings
The experience of uncertainty was common in patients with COPD before starting PR. The uncertainty began with their lack of knowledge with regard to how their COPD had been diagnosed. A comment about health professionals not having time to explain the condition is an example of this. Participants who were angry or disappointed with their COPD care felt they were floating in the NHS with an uncertain future. Those participants who expressed feelings of anger with the care they received also experienced more panic and uncertainty. However, some participants who expressed less frustration and anger perceived COPD to be a cyclical phenomenon, which they felt was less concerning as associated problems were temporary rather than chronic. Some were able to use breathing exercises to control their fear and panic. However, feelings of uncontrolled panic were very disabling for many participants and seemed to be made worse because of their uncertainty.
The strengths and limitations of this study
This study recruited participants from two PR programmes run by separate teams. This enabled greater variance in patient experience to be explored. Patients were recruited as a result of having COPD written on their referral to enter PR. This diagnosis was not necessarily confirmed by formal spirometry. Therefore, it is possible that the patients recruited all did not have COPD. However, spirometric diagnosis of COPD is reported to be underused and not always accurate in primary care. 19 –21 Therefore, the inclusion criteria strengthen this study’s applicability to clinical practice.
How and why it agrees or disagrees with the existing literature
The lived experience of uncertainty has been mentioned in other studies involving COPD patients. This finding has some similarities to reports that patients with severe COPD were ‘directionless’ from a longitudinal study by Pinnock et al. 22 Participants in Pinnock et al.’s study found it impossible to identify a beginning to their COPD story. Chan 11 also described the experience of uncertainty in a very small (n = 3) study of patients with COPD in Hong Kong. In 1993, Small and Graydon 23 reported that COPD patients in hospital experience uncertainty with regard to their future. However, they state that patients may use a range of mechanisms to cope with the uncertainty, such as developing a positive attitude, hope, acceptance and making positive comparisons with other people. The study presented here suggests that uncertainty may be just as disabling for patients early after diagnosis. In 2012, Wortz et al. 24 reported that COPD patients experienced uncertainty about preventing the progression of their disease and the future of living with COPD. However, participants in the study presented here were not only uncertain about the future but also expressed feelings of uncertainty from living with COPD which affected their past, present and future perceptions.
Floating has previously been characterized as a positive effect of PR and contrasted with the ‘sinking’ nature of living with chronic lung disease. 25 The experience of floating in the study by Toms and Harrison 25 was a positive but temporary phenomenon of coping with COPD which was lost following PR. The floating that participants described in our study is more akin to ‘drifting’ with no control over direction or speed and relates to their uncertainty and experience of being in limbo with their care in the present. This contrasts with Toms and Harrison’s description of floating versus sinking related to patients’ ability to cope, like an ability to swim in rough waters. This experience of floating was associated with anger and disappointment for participants in our study. These participants may have expected better care from the National Health Service and felt that they were waiting too long for consultations, treatment or therapy. A group education session during the waiting period prior to PR has been shown to improve patient attendance and retention. 26 This kind of session may also have benefits in terms of reducing the perceptions of waiting and floating before patients start PR, thus reducing patient anger and uncertainty.
Feelings of anger and panic have been previously described by other patients with COPD. 10 Howard et al. 27 found that those who were angry about their condition, and thought of COPD as chronic in nature, experienced increased severity of panic attacks. Encouraging patients to perceive their condition as more cyclical than chronic may therefore have positive health benefits and reduce the burden of living with COPD. Fischer et al. 28 suggest that the perception of COPD being cyclical may reflect a generally more positive outlook in those who are not significantly disabled by their symptoms. In one study, 47% of COPD patients who gave reasons for non-attendance at PR perceived their condition as either too mild or severe to warrant PR. 4 This study reinforces the message that illness perceptions impact on the ability of patients to manage their COPD.
Previous research has shown that the length of time since the appearance of first symptoms, and since diagnosis, affect patients’ perceptions of chronic conditions. Fischer et al. 28 found that illness perceptions of COPD patients who had been diagnosed for 5 years or more differed from those diagnosed for <5 years. However, in their study, illness perceptions appeared to be associated with an increase in disease burden in those diagnosed for 5 years or more. 28 It is not known how time affects illness perceptions of patients with COPD. In this study, many had been recently diagnosed and were experiencing anger with their care, panic and uncertainty. Further research is needed to establish if this persists, worsens or is alleviated as time passes.
The implications for future research and clinical practice
Many of the participants in this study were interviewed soon after they were diagnosed. There is a national drive in the United Kingdom to diagnose COPD earlier in patients’ disease progression. 29 However, there may be limited benefit in earlier diagnosis if pathways are not in place to provide optimal care at that point of time. Currently, PR is generally being offered when significant physical difficulty is already well established. By this stage, many patients may have endured years of disabling uncertainty, potentially leading to higher levels of morbidity.
Prompt and regular communication with COPD patients in primary care may reduce their experience of floating. This would reduce anger at their perceived lack of attention, which should also reduce other disabling emotions such as panic. Early referral to PR (possibly based on psychosocial disability rather than the modified Medical Research Council dyspnoea scale score) may benefit these patients earlier in the progression of their disease. It is proposed that there is currently a gap in health care pathways for COPD patients immediately after diagnosis in primary care, where disabling uncertainty seems to be common. More understanding of the importance of uncertainty early after diagnosis will enable us to develop interventions directed at alleviating the associated effects, such as fear and panic.
Further research is required to explore illness perceptions in patients with COPD immediately after diagnosis and how these might impact their uptake of PR. It would also be useful to determine whether encouraging COPD patients to perceive their condition as a cyclical disease, rather than a chronic deteriorating process, can reduce their experience of uncertainty and panic.
Conclusions
This is the first study to explore the lived experience of patients with COPD from point of referral to PR to uptake (or not) of PR. In this sample, the lived experience of uncertainty was disabling. The uncertainty was associated with negative perceptions regarding their past and current care, their illness and PR. Recognition of the role that uncertainty plays in patients with COPD patients is the first step towards developing interventions focused on reducing this uncertainty and thereby reducing the overall burden of the disease for the individual patient and facilitating PR attendance.
Footnotes
Acknowledgements
The authors would like to thank all the participants for giving their time to this study and providing such valuable information. Moreover, we are thankful to both the community respiratory teams in Solent NHS Trust and the University of Southampton for providing continued support.
Funding
This study was funded by NHS Education South Central as part of a Clinical Academic Pathway PhD Studentship.