
Abstract
Pulmonary rehabilitation (PR) is an evidence-based, low-cost, non-medical treatment approach for patients with chronic respiratory diseases. This study aimed to start and assess the feasibility, acceptability and impact of a PR programme on health and quality of life of respiratory patients, for the first time in primary care in Crete, Greece and, particularly, in a low-resource rural setting. This was an implementation study with before–after outcome evaluation and qualitative interviews with patients and stakeholders. In a rural primary healthcare centre, patients with chronic obstructive pulmonary disease (COPD) and/or asthma were recruited. The implementation strategy included adaptation of a PR programme previously developed in United Kingdom and Uganda and training of clinical staff in programme delivery. The intervention comprised of 6 weeks of exercise and education sessions, supervised by physiotherapists, nurse and general practitioner. Patient outcomes (Clinical COPD Questionnaire (CCQ), COPD Assessment Test (CAT), St. George’s Respiratory Questionnaire (SGRQ), Patient Health Questionnaire-9 (PHQ-9), Incremental Shuttle Walking Test (ISWT)) were analysed descriptively. Qualitative outcomes (feasibility, acceptability) were analysed using thematic content analysis. With minor adaptations to the original programme, 40 patients initiated (24 with COPD and 16 with asthma) and 31 completed PR (19 with COPD and 12 with asthma). Clinically important improvements in all outcomes were documented (mean differences (95% CIs) for CCQ: −0.53 (−0.81, −0.24), CAT: −5.93 (−8.27, −3.60), SGRQ: −23.00 (−29.42, −16.58), PHQ-9: −1.10 (−2.32, 0.12), ISWT: 87.39 (59.37, 115.40)). The direct PR benefits and the necessity of implementing similar initiatives in remote areas were highlighted. This study provided evidence about the multiple impacts of a PR programme, indicating that it could be both feasible and acceptable in low-resource, primary care settings.
Introduction
Background of the problem
The burden of chronic respiratory diseases (CRDs) in Greece is significant. Namely, the prevalence of chronic obstructive pulmonary disease (COPD) is estimated at 8.4%, with higher rates being observed in semi-urban and rural areas. 1 The prevalence of asthma in the adult population reaches 9%. 2 At the same time, exposure to risk factors is high, with the country having one of the highest rates of tobacco consumption in the European Union. 3
CRDs are also responsible for substantial costs for Greek patients and the healthcare system, with the total annual costs of managing COPD and asthma (including medications and hospitalizations) reaching 4730 and 2281 euros per patient, respectively. 4,5 Further to their economic impact, CRDs constitute an important issue for the quality of life and work productivity of patients in Greece. Specifically, annual per patient productivity losses exceed 900 euros for COPD 4 and 600 euros for asthma, 5 while disability adjusted life years are estimated at 0.2 for COPD and 0.4 for asthma per 1000 capita per year. 6
Despite the above, integrated services for patients with CRDs, including pulmonary rehabilitation (PR), are largely absent in the country, especially at the primary care setting. While the World Health Organization (WHO) places increasing emphasis on chronic diseases, integrating primary and secondary care in the management of long-term conditions remains a neglected area in the current health agenda. 7 The situation has been aggravated during the last decade due to the economic crisis experienced in the country, leading to even more severe restrictions for patients with CRDs. 8,9
Rationale for the implementation strategy
In 2015, a development study was conducted in Uganda aiming to assess the feasibility of a culturally adapted PR programme, 10 developed based on UK standards. 11 This was not a substitution of hospital-based PR, but rather a low-cost and locally tailored approach (e.g. PR training equipment was substituted by practical, everyday objects, while recruitment, referral and learning processes were based on local cultural demands).
Experience gained from this programme was used to inform content, design and delivery of PR programmes for roll-out in other resource-limited settings. This particular study was part of the European Horizon 2020 FRESH AIR project. 12
Rationale for the intervention
PR is an evidence-based, non-medical, low-cost treatment intervention, proven effective in amending the systemic effects of lung disease, including breathlessness, inactivity and deconditioning. 13 PR is recommended by international guidelines for patients with COPD. 13 –15 The pilot PR programme of Uganda resulted in substantial improvements in patient symptoms, exercise capacity 10,16 and quality of life. 17,18 To this direction, improving functional status with limited cost may significantly benefit people with CRDs and their families also in Greece, especially during the ongoing period of austerity.
Aims and objectives
This study aimed to adapt, implement and evaluate a PR programme for patients with CRDs, in a rural primary care setting in Crete, Greece. Specific objectives were: To determine the programme content (e.g. exercise and educational activities); To adapt existing manuals and educational materials; To define suitable outcome measures for evaluating the programme’s impact on patients, including general- and disease-specific indicators; To evaluate process outcomes (i.e. recruitment, response and engagement rates); and To assess the programme feasibility and acceptability through qualitative research.
Methods
Study design
A pre–post implementation study of a community-based PR programme was conducted using quantitative and qualitative research. The quantitative component assessed recruitment, concordance, attrition and patient outcome indicators. Qualitative research explored feasibility and acceptability of the PR programme. The study followed the Standards for Reporting Implementation Studies. 19
Context
The Greek healthcare system combines elements from both the public and the private sector. 20 Primary care is mainly represented by vocationally trained general practitioners (GPs), typically serving in healthcare centres and rural practices with limited inter-professional support.
Respiratory care is organized at three levels: (i) GPs and private practice doctors offering primary care; (ii) hospitals providing secondary care; and (iii) tertiary hospitals offering specialized services. Respiratory services mainly focus on acute care with much lower emphasis on long-term management and preventive services. Integration and coordination within primary care and between primary and secondary care still requires extensive efforts.
The economic crisis has, additionally, meant reductions to healthcare budgets, resulting in cuts to several public services. PR is offered at a very limited scale, remaining restricted to few tertiary hospitals. PR programmes are not available in the rural periphery, where the burden of CRDs is substantial 1 while the population is more deprived in terms of both income and healthcare provision. 21,22
Study population
The study population consisted of patients with a diagnosis of a clinically stable CRD, including COPD and asthma. Patients were recruited and referred by GPs serving the study site who also performed an initial medical review to confirm diagnosis.
Suitable patients were invited to undertake a baseline assessment performed by a PR supervising team to determine eligibility for entry into the study. This included screening and tests to determine physical capacity and respiratory status.
Inclusion criteria were: Definite diagnosis of COPD and/or chronic asthma; Medical Research Council (MRC) dyspnoea score of two or higher.
Exclusion criteria were: Within 4 weeks of an acute exacerbation; Unwilling or unable to attend the programme; Unstable cardiovascular disease or locomotor difficulties precluding exercise; and Unable to provide informed consent.
Since this was a development study, sample size estimation was not performed. Based on previous studies suggesting that a sample of 30 patients is sufficient to measure before and after changes in the main outcome measures (Incremental Shuttle and Walking Test (ISWT) distance and Clinical COPD Questionnaire (CCQ) total score), assessing at least 40 patients was set as the recruitment goal. 16
Sites
A public primary healthcare centre located at a rural area of Heraklion on the island of Crete, Greece was selected to host the PR programme due to its representativeness, capacity, safety and quality standards (basic diagnostic tools, brief inpatient treatment, ambulance service, comfortable spaces), affordable distance from the university and focal position (serving a population of 48,855 people with 13 rural practices belonging to its operational responsibility). PR sessions were performed in a spacious room and the grounds of the building.
Two physiotherapists and one nurse were posted at the study site to conduct PR. Their selection was based on their professional experience and availability from official duties. A GP serving the centre completed the PR team. Supervising team members had over 15 years of practice in public healthcare facilities, with lifelong experience with respiratory patients.
Implementation strategy
The implementation strategy consisted of stakeholder meetings, adaptation of PR context and educational materials, training of the supervising team and programme delivery and assessment. Groundwork was conducted in 2016 in Crete. Meetings were held with regional health authorities, healthcare and administrative staff, patients, academicians and researchers to determine suitable locations, processes of patient recruitment and the team required to assess patients and conduct the programme. Key messages delivered by groundwork activities established that: Patients were interested and available in sufficient numbers in primary care. Patients were able to access the study site. GPs were able to refer to PR. There was sufficient space and facilities in the site to run the programme.
In March 2016, the research teams from United Kingdom and Crete met in Crete to adapt PR content, design and delivery and train the local healthcare professionals. The training of the PR team was provided face-to-face by the UK team during a one-week period and was supported by previously developed educational materials and videos. 10 It included introduction to PR and its benefits, interactive demonstration and explanation of exercises, train-the-trainer sessions on risk factor education, motivational techniques, assessment of patient eligibility and data collection procedures. These activities were also tested in field prior to programme initiation. Several distant sessions were also held online to support the local team. Data collection procedures were also established and visits to the study site were performed to ensure appropriateness of space and procedures.
Intervention
PR consists of a programme of exercises and health education based on international guidance. 11,23 Following the structure of the original programme (Figure 1), PR in Crete was delivered as a 6-week programme, with twice-a-week sessions of approximately 2 hours. After baseline assessment, patients were assigned to one pilot (June–July 2016) and two main groups (September–October 2016) of 10–12 participants each. Programme completion was defined as attendance of 75% of classes. There were no differences in the design, implementation or evaluation between the pilot and main groups. The distinction served only with identifying unexpected procedural barriers that could have hampered programme conduction. Since no such barriers were encountered, we report our results on the overall sample rather than on each group individually.
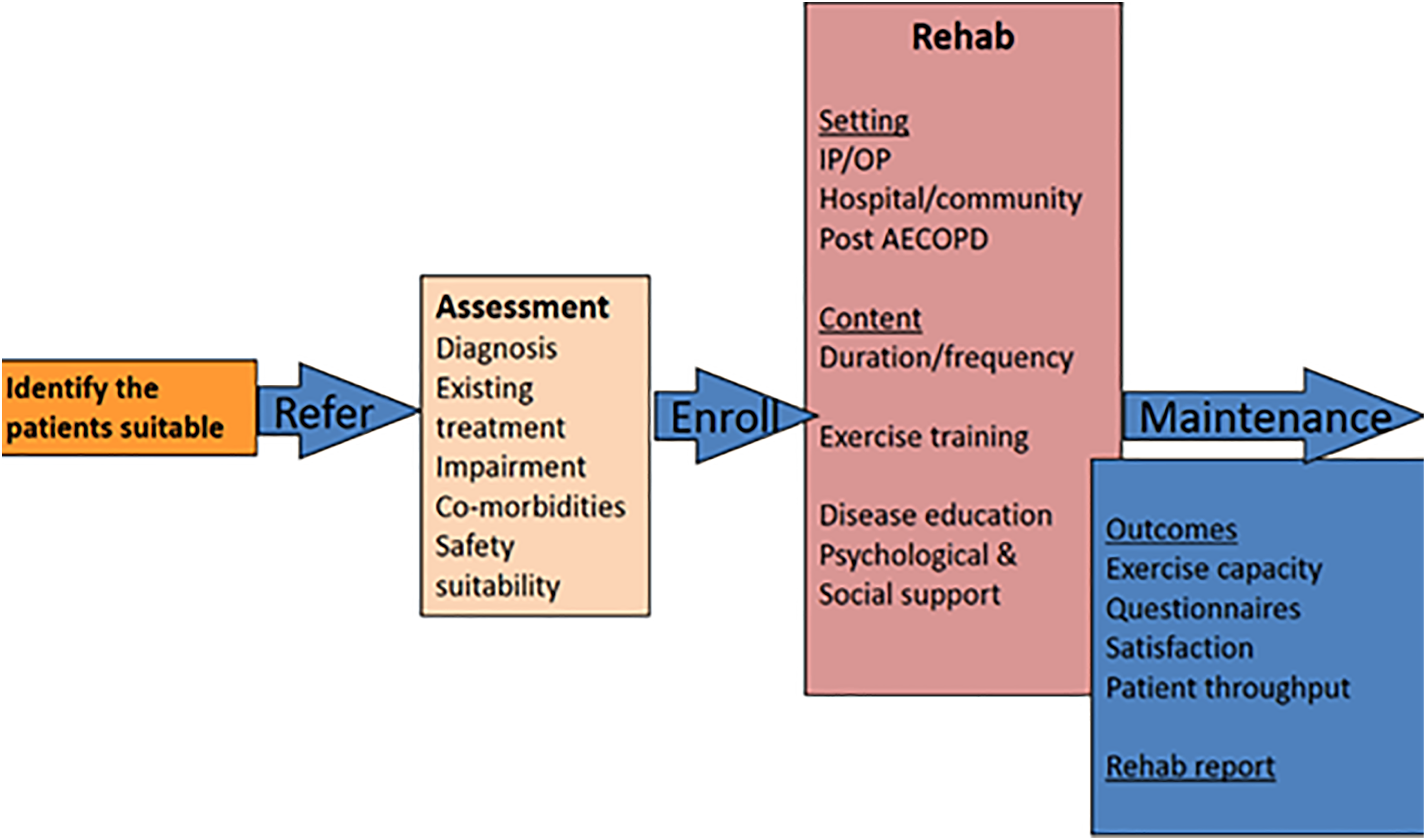
Components of the programme of Crete, Greece.
Each PR session included half an hour of walking in the yard and 1 hour of resistance and strength exercising (bands and weights for upper and lower limbs, sit-to-stand, steps) and static bicycle. PR equipment was kept minimal, while practical solutions were provided to patients to maintain PR exercises at home (e.g. weights as bottles of water). Everyone followed the same exercise regime; however, its level of difficulty was adjusted for each individual and monitored as programme progressed. Specifically, walking and exercise intensity and duration were based on Borg rating. If patients graded 4 or lower, exercise intensity was increased in the next session. In case Borg score was between 4 and 6, intensity was kept the same, until exercise became easy. In case of disagreement between heart rate and Borg score, heart rate guided the progression of exercise intensity in the following session.
Seven educational sessions of 1 hour were delivered per group by the trained PR team (GP, physiotherapists, nurse). Their contents were based on existing materials, adapted during groundwork. 16,24 They covered causes of breathlessness, coping and relaxation techniques, secretion disposal, risk factor (tobacco and biomass smoke) avoidance, behaviour and lifestyle modifications (e.g. nutrition), medication intake (e.g. using inhalers), handling the CRD psychological impacts and understanding the importance of exercising and maintaining PR benefits. Written materials reminding the exercises and education were developed and provided to participants to encourage PR continuation and sharing with other community members.
Outcomes of the implementation strategy
Implementation strategy outcomes included the production of a culturally adapted and affordable PR programme, training of healthcare staff and programme implementation. Adaptation of procedures was summarized from stakeholder meeting reports, field notes and patient comments. Barriers and facilitators were recorded throughout the project to inform the implementation process and were summarized in discussions between the two research teams. Costs associated with purchasing PR equipment not routinely available in primary care were also documented to keep track of the direct extra expenditure.
Outcomes of the intervention
Patient socio-demographic characteristics, medical history, health habits and outcomes were assessed by the PR supervising team at baseline and at the end of PR using an adapted Case Report Form.
10,16
Outcomes included: Respiratory health status using the CCQ,
25
COPD Assessment Test (CAT)
26
and Saint George Respiratory Questionnaire (SGRQ)
27
; Dyspnoea using the MRC and Borg Dyspnoea Scales
28
; Functional impairment using the Karnofsky Score
29
; Depression using the Patient Health Questionnaire-9 (PHQ-9)
30
; Biometric indicators (height, weight, limb circumference); Functional measures using the sit-to-stand time
31
; and Exercise capacity using the ISWT
32
with before and after pulse oximetry.
Process evaluation
Adoption and reach of the programme were evaluated by reporting the number of sites implementing PR, the numbers and types of healthcare staff trained and delivering PR and the number of patients assessed, entered and completing the programme.
Feasibility and acceptability of the PR programme were examined through qualitative research, using theoretical input from the health belief model. 33 Semi-structured interviews were performed by local researchers before and after the PR programme with a sample of purposively selected patients. A focus group with stakeholders (site healthcare and administrative staff, community leaders, PR team members, specialized doctors) led by a local qualitative expert was also conducted at the end of the programme. In summary, qualitative activities assessed programme’s practicality (e.g. how easy was it to attend and follow the programme), implementation (e.g. what went wrong or well, recruitment, retain, achievement of expectations), barriers/facilitators (e.g. to attendance, implementation) and sustainability (e.g. maintenance of benefits, programme scaling up).
Analysis
Patient outcomes were summarized using descriptive statistics; 95% confidence intervals (95% CIs) were estimated for quantitative variables. Fishers’ exact test was used to compare proportions, with significance set at a = 0.05. Analysis was performed using SPSS (Version 23.0. Armonk, NY: IBM Corp). Published Minimal Clinically Important Differences (MCIDs) are reported in relation to observed changes in clinical outcomes.
All qualitative activities were audio-taped, transcribed and analysed using thematic content analysis by a local qualitative expert. The majority of qualitative data was translated into English and a qualitative scientist from the UK team cross-checked results. Conclusions were based on consensus between the two teams.
Ethics
The study was approved by the 7th Health Region of Crete (Pr. No.: 6951, 27 May 2016). During baseline assessment, eligible patients were provided with an information sheet, explaining the study aim and all activities. Explicit information was provided verbally by the supervising team, along with the opportunity to ask any questions. All participating patients signed an informed consent document. Signed informed consent was also obtained by stakeholders for participation in the focus group.
Results
Developing the implementation strategy and intervention
Relatively minimal adaptation to the PR programme of Uganda was performed. Adaptations were mainly cultural and included: Translation of documents into Greek and Exclusion of post-TB patients due to very low TB notification rates in Greece.
34
Replacement of the EuroQoL (EQ-5D) questionnaire with the SGRQ and CAT as disease-specific health status tools, validated and used widely in the Greek context
35,36
: Delivery of walking exercises outdoors due to suitable weather; Purchase of training equipment instead of using practical objects due to higher capacity; Discarding of the follow-up data collection at 6 weeks post-rehabilitation; and Development of patient diaries to record symptoms, medications and exercises.
Delivering the intervention
A total of four healthcare professionals were trained and delivered the PR programme in one primary healthcare centre. Patient flow in the study is illustrated in Figure 2. Overall, 63 patients underwent baseline assessment and 46 were found eligible. In total, 40 patients started PR (participation rate: 87%), with 31 completing the programme (completion rate: 77.5%). Lack of time and reluctance due to unfamiliarity with PR procedures were mentioned as main reasons for not engaging with the programme. Medical issues and lack of time were reported as main reasons for dropping out the programme.
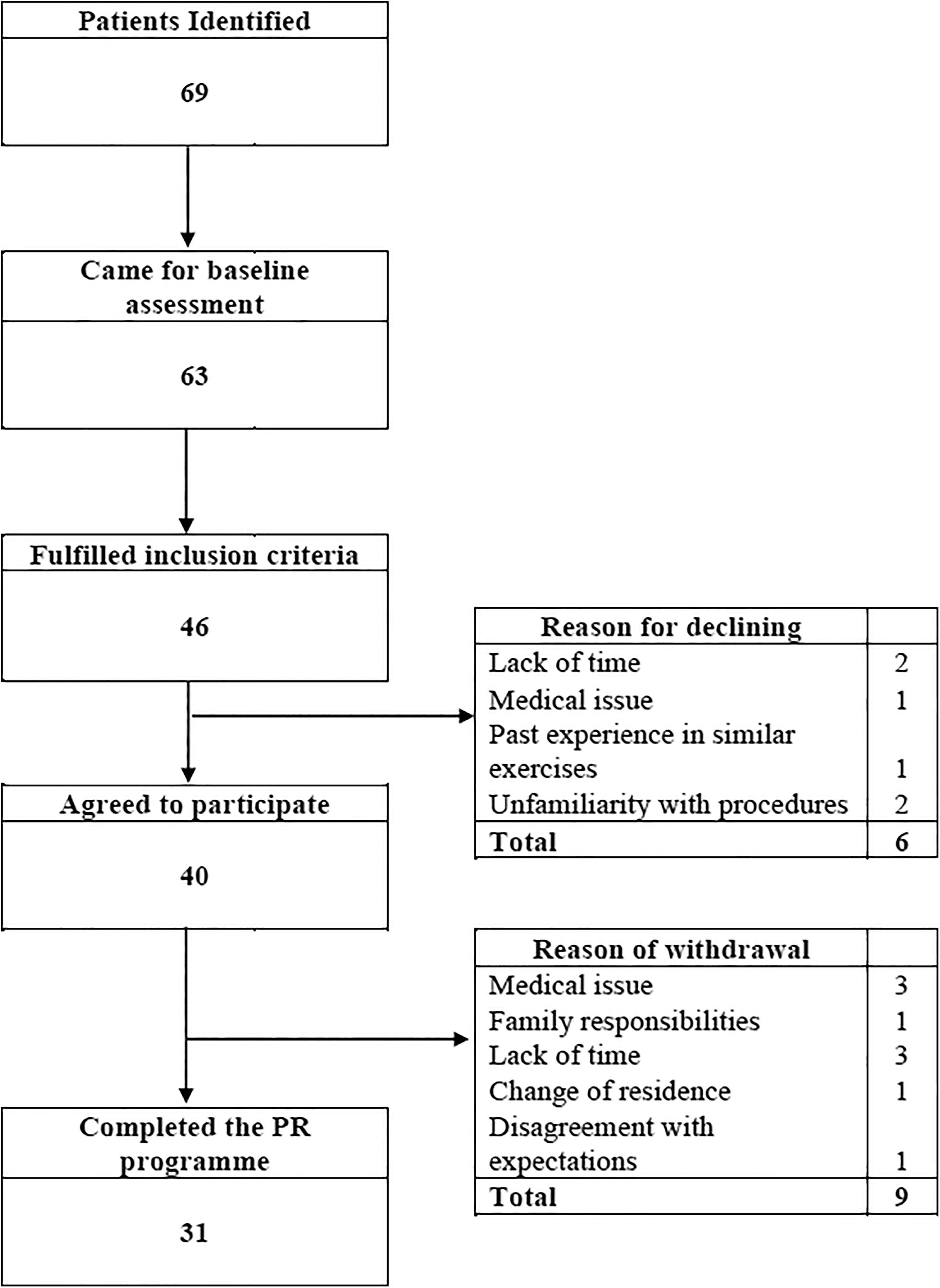
Recruitment flow diagram of COPD and asthma patients of the PR programme in Crete, Greece. PR: pulmonary rehabilitation; COPD: chronic obstructive pulmonary disease.
The total cost of purchasing PR equipment (weights, digital chronometers, bands, step aerobics, stationary bicycles and printouts) was 1602.66 euros.
Patient health outcomes
Table 1 presents the main baseline characteristics of the original sample of patients, along with differences among individuals who dropped out and those who completed the programme. Overall, slightly more than half of patients were females (55.0%), with a mean age of 67.2 years (95% CI: 63.9, 70.5). COPD was the main diagnosis for 60.0%, while 65.0% had ever smoked. With the exception of education (p = 0.019), no differences were observed between people completing and dropping out of PR with respect to socio-demographic characteristics.
Baseline characteristics of the original sample of COPD and asthma patients (N = 40) and differences between patients dropping out and completing the PR programme in Crete.

CI: confidence interval; BMI: body mass index; ISWT: Incremental Shuttle Walking Test; CCQ: Clinical COPD Questionnaire; CAT: COPD Assessment Test.
a p Value based on Fischer’s Exact Test.
In addition, mean BMI of the total sample was 31.24 kg/m2 (95% CI: 29.63, 32.84), namely 33.79 (95% CI: 31.17, 36.41) for patients dropping out and 30.58 (28.69, 32.47) for those completing the programme. Patients who dropped out also had lower ISWT than their counterparts (mean difference: −53.84, 95% CI: −134.26, 26.59), with the mean value for the overall sample being 244.36 m (95% CI: 211.21, 277.51). Total CCQ score was 1.86 (95% CI: 1.51, 2.21) with a difference of 1.04 (95%CI: −0.41, 2.49) between individuals dropping out and completing PR.
Data on pre- and post-PR outcomes are presented in Table 2, for patients who completed the programme. Mean dyspnoea levels as measured by the MRC scale was reduced by 1.03 points, reaching the MCID of 1. 37 Functional and exercise capacity measurements were improved by the end of PR. The mean sit-to-stand time was reduced by 2.41 seconds, a change close to the MCID of 2.3 seconds. 38 The mean ISWT increased by 87.39 m greatly exceeding the MCID of 47.5 m. 39 The mean dyspnoea levels after performing ISWT, as measured by the Borg scale, decreased by 0.94 units.
Outcomes of patients at baseline and at the end of the PR programme in Crete.

CI: confidence interval; BMI: body mass index; MRC: Medical Research Council; ISWT: Incremental Shuttle Walking Test; CCQ: Clinical COPD Questionnaire; CAT: COPD Assessment Test; SGRQ: Saint George Respiratory Questionnaire; PHQ-9: Patient Health Questionnaire-9; PR: pulmonary rehabilitation; COPD: chronic obstructive pulmonary disease.
Substantial improvements were also documented in all health status indicators. The mean CCQ total score was reduced by 0.53 units, a difference above the MCID of 0.4. 40 Mean CAT score dropped by almost 6 units, exceeding the MCID of 2. 41 The mean SGRQ total score decreased by 23 units, a difference higher than the MCID of 4. 42 The mean Karnofsky score was improved by 9.67 units. PHQ-9 scores were low already from baseline, yet a reduction of 1.10 points was observed.
Feasibility and acceptability
Interviews were conducted with a total of 8 patients (4 males, mean age: 64.5 years) pre- and post-PR. Seven stakeholders attended the focus group, including the PR physiotherapists and nurse, one GP facilitating patient recruitment, the site director (also a GP), the community vice-mayor and a pulmonologist from a public hospital of the city.
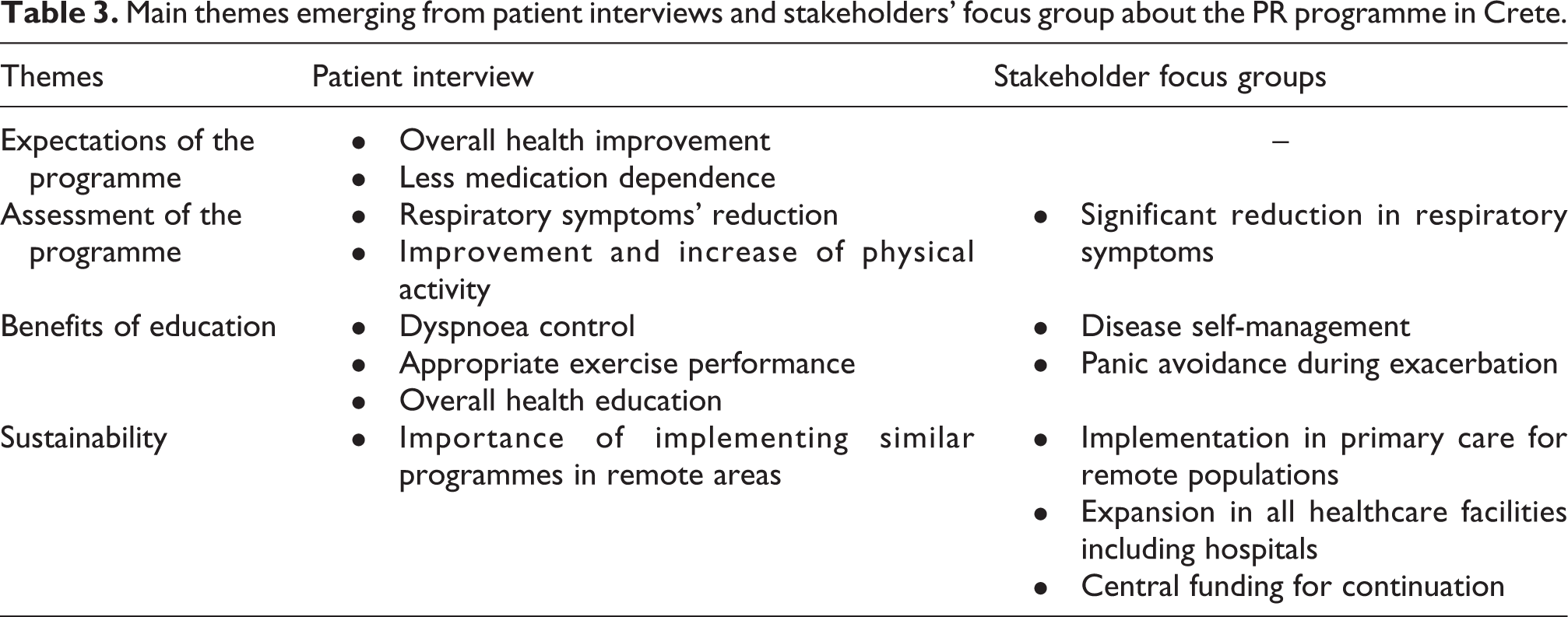
The main themes of qualitative interviews and focus groups are presented in Table 3. A detailed description will follow in a separate report. In summary, patients’ expectations included an overall health improvement and less medication dependence, partly to alleviate the financial burden of drugs. At the end of PR, both patients and stakeholders positively assessed the programme, noting the significant symptoms’ reduction, the improvement and increase of physical activity and the benefits of received education on disease self-management. Patients and stakeholders recommended that the PR programme should be sustained and similar actions should be implemented in remote areas.
Main themes emerging from patient interviews and stakeholders’ focus group about the PR programme in Crete.
Barriers and facilitators of implementation
Key barriers and facilitators identified by patients and stakeholders are summarized in Table 4. According to patients, barriers mainly concerned caring responsibilities, while few were related to accessing the programme. A key facilitator enhancing participation as perceived by both patients and stakeholders included the opportunity offered to patients by the programme to socialize while improving their health. Additionally, stakeholders identified timely information and comprehensive GPs’ referral as core elements facilitating optimal recruitment. In contrast to patients, barriers to attending PR according to stakeholders’ concerned transportation and an initial hesitation of patients attributed to lack of experience with such initiatives.
Key barriers and facilitators to implement the PR programme in Crete, according to patients and stakeholders.

PR: pulmonary rehabilitation; GP: general practitioner.
Discussion
Summary of findings
Our results suggested substantial and clinically important improvements in patient outcomes including symptoms (MRC dyspnoea scale), exercise (ISWT, sit-to-stand test) and quality of life (CCQ, CAT, SGRQ). The feasibility potential, along with a request for sustaining and expanding similar initiatives for remote populations, was also highlighted.
Discussion of the study’s findings in the light of international literature should be performed with caution due to considerable diversities in settings, patient characteristics and programme designs. Yet, pre- and post-PR differences in main clinical outcomes (CCQ and ISWT) were generally close to those observed in the development study of Uganda. 16
By reading other studies, differences in ISWT and CCQ recorded in this one were generally higher. In a comparative review, the change in ISWT was found 39.77 m higher in COPD patients receiving PR versus usual care, a result much lower than the pre-/post-ISWT difference documented in this study (87.39 m). 43 Similarly, in a prospective study of 419 COPD patients, CCQ improved by 0.6 points after PR, a change close the one observed in this study (−0.53). 44 Changes in SGRQ total score (−23.00) were also higher than in other studies (−21.07 and −12.3, respectively). 45,46
Improvements observed in SGRQ scores were impressive. This may explained by the fact that, as disease-specific questionnaire, the SGRQ is more likely to be responsive to changes after PR and more sensitive to specific respiratory issues. 47 Additionally, the fact that the programme served patients in a holistic manner, including medical, psychological and social support, may have increased their overall positive response and assessment.
Interestingly, the completion rate documented in our study (77.5%) was similar or higher than other reports. In a study assessing a community-based PR programme, less than 57% of patients completed the full regime. 48 In an assessment of over 200 PR programmes in the United Kingdom, the completion rate was lower than this study (60%). 49 In other studies, adherence or completion rates ranged around 70%. 50,51
Strengths and limitations
To the best of our knowledge, this is the first attempt to establish and assess a community-based PR programme in rural primary care areas in Greece. Yet, our study is prone to certain limitations. Firstly, this was a development study with small sample size and without adequate statistical power to perform significance testing. Its design does not also allow for any type of comparisons or causality determination. We are also unable to report on patient lung function characteristics. Spirometry is not available in Greek primary care and our efforts in overcoming this by using a portable spirometer did not provide quality results (most frequent errors: reduced expiration time, obstruction of the spirometer mouthpiece, poor patient collaboration and reduced peak expiratory flow). Additionally, we did not capture an overview of the long-term effects of the PR programme; however, this does not affect our before and after indicators. Furthermore, the local setting and population as well as the primary care context and organizational culture may significantly differ from Western or other low-resource settings, raising implications regarding generalizability. Interpretation of results also requires caution due to two sources of potential bias which may have influenced the provided self-reported information: the free-for-service nature of the present PR programme and the close relationships established over time between patients and healthcare professionals. As implementation research, our results may, however, offer valuable insights in terms of PR delivery for local and other low-resource settings.
Implications of the study
This study is in accordance with international literature documenting the beneficial effects of PR for patients with CRDs. 14,52 The experience and novel evidence gained through the PR programme of Crete may provide ground for future research to elicit precise estimates about the effectiveness and cost-effectiveness of PR and to ensure the optimal implementation of similar efforts addressing respiratory as well as other non-communicable diseases.
The PR programme achieved to bring together a group of diverse healthcare professionals and engage patients in an interactive procedure of education and health improvement. This is particularly relevant for informing clinical practice and service delivery in a country which is missing high performance in several aspects of quality-based care, including proactive involvement of patients in their therapeutic process, use of multidisciplinary teams and focus on disease prevention and health promotion. 53,54 Creating the health and social environments to support patients’ participatory engagement and motivation to act for their health, along with exploring how medical curricula could be adjusted to include education on PR and other team-based approaches, seem to be important messages of this study.
The PR programme of Crete was implemented in times of an economic recession which has significantly affected the size, structure and quality of provided health care services, with particular evidence capturing these unfavourable effects on patients. 9,55,56 Primary care is the most sustainable, accessible and cost-effective setting to tackle non-communicable diseases according to the WHO. 57 Additionally, it provides the ground for multidisciplinary collaboration, patient empowerment and community reactivation, which are all core components of PR. Instigating integrated disease management programmes such as PR in primary care may assist not only with improving patient outcomes and quality of life 58,59 but also with increasing the overall level of care integration 60 with positive effects on systems and communities.
The findings of this study, supported by the already reported health and financial benefits of PR, 52,61,62 speak to the need to work with policymakers to advocate for integration of PR programmes in primary care, provision of universal coverage through social insurance and investigation potential synergies with existing services to offer high-quality and affordable respiratory care for all. Taking into consideration the Primary Healthcare Reform and the changes of the curriculum of General Practice currently unfolding in Greece, 63 this study comes as timely as ever to provide further space for constructive discussion.
Conclusions
In a period of economic recession, these results highlight that evidence-based and low-cost PR programmes may constitute a promising in terms of improving patient outcomes, feasible and acceptable approach towards CRDs in low-resource, primary care settings.
Footnotes
Acknowledgements
The authors thank the healthcare and administrative personnel as well as the patients of the study site for their contribution in this programme. The authors also thank Mr Antonis Bertsias and Mr Myron Galenianos, team members of the Clinic of Social and Family Medicine, School of Medicine, University of Crete, for their assistance in the implementation of the project. The authors thank the local municipal and health authorities for their support. The authors thank Prof. Sally Singh and colleagues at the University Hospitals Leicester for their support of the physiotherapists in Crete. The authors gratefully acknowledge the International Primary Care Respiratory Group (IPCRG) for introducing us to the consortium and primary care networks involved in this study, for their continued facilitation of clinical engagement and for their leadership in the execution of this work. RJ and SvK were supported by the PenCLAHRC network of the NIHR in United Kingdom.
Author contributions
MA participated in the local coordination of the project, analysed the quantitative data, interpreted all results with the co-authors and wrote the first version of the manuscript. MT conducted the qualitative research and analysed the data, participated in the writing of this manuscript. AP, MT and MM participated in the local adaptation procedures were trained and delivered this programme and contributed to the finalization of this article. NC is the principal investigator of the overall FRESH AIR project, an original author of the FRESH AIR protocol and participated in the finalization of this manuscript. RJ and JP contributed to the design, conduct of the study, data interpretation and manuscript writing. SvK contributed to the analysis of data and writing of the article. CL was the country leader for the FRESH AIR project and participated in the design, study conduct, data interpretation and writing of the manuscript. IT participated in all steps of this programme by designing, coordinating, assessing and evaluating patients, being the GPs responsible for this programme and writing of this article. All authors have read and approved the final version of this manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MA, MT, AP, MT, MM, NC, JP, SvK, CL and IT have no conflict of interest to declare. RJ reports grants, personal fees and non-financial support from Astra Zeneca, GSK and Novartis; personal fees and non-financial support from Boehringer Ingelheim and Chiesi, and non-financial support from Nutricia.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: FRESH AIR was funded by European Union’s Research and Innovation program Horizon 2020 (Health, Medical research and the challenge of ageing) under grant agreement no. 680997 TRIAL ID NTR5759, ![]() . Funders had no role in any aspect of the study including design, data collection, analysis and interpretation, or writing of the manuscript.
. Funders had no role in any aspect of the study including design, data collection, analysis and interpretation, or writing of the manuscript.