
Abstract
A retrospective analysis of 23 patients was undertaken to evaluate the outcome of pulmonary rehabilitation (PR) in patients with pulmonary hypertension (PH) over a preceding 6-year time frame. Chart review and data analyses were undertaken evaluating pulmonary arterial hypertension pharmacotherapy versus the same therapy with the addition of PR. Analysis included 23 patients who had a mean pulmonary artery pressure of 36.6 while on therapy and who had initial six-minute walk tests (6MWTs) ranging between 54 and 396 meters. Outcomes included 6MWTs and Saint George’s Respiratory Questionnaire. There was no improvement in 6MWT postpharmacotherapy. Patients with low 6MWT <250 meters had substantial gains in 6MWT postrehabilitation (average of 86 meters). As well, those with initial 6MWT >250 meters had a significant improvement of 52.55 meters, documenting the utility of PR in patients with PH. PH patients are increasingly seen in PR clinics as they share many characteristics present in chronic respiratory disease states. There is increasing literature supporting the utility of PR in this population. We have found that patients with 6MWTs as low as <250 meters are also candidates for PR and can demonstrate substantial benefits as measured using the 6MWTs.
Keywords
Introduction
Pulmonary hypertension (PH) leads to reduced physical activity and poor quality of life (QOL) because of exertional dyspnea. 1 Previously, expert recommendations included avoidance of any exertion or activity, including pulmonary rehabilitation (PR), but there are now sufficient studies demonstrating the benefits of PR in this population. 2 –8 These studies have demonstrated the presence of myopathic changes in skeletal musculature that are responsive to training. 3,9 They have also demonstrated meaningful outcomes in physical activity as measured by the six-minute walk test (6MWT) 4,6 as well as improvement in QOL scores postpulmonary rehabilitation. 2,5,10
The 6MWT is a part of the evaluation of patients with chronic respiratory disease in general and has been used as a part of the evaluation of pharmacotherapy in PH. We were interested to learn of the outcomes from our experience at Beth Israel Medical Center in patients with PH who participated in PR services. Specifically, we wanted to compare the outcomes in 6MWT as a result of pharmacotherapy and PR as well as to ascertain whether PR had meaningful outcomes when initial 6MWTs were in a low to very low range. We have chosen to review 6 years of data from our hospital which has both a PH center and a PR center.
Objectives
We have retrospectively evaluated the effect of PR in patients with PH who are already optimized on medical therapy. We were curious to learn whether the clinical improvements from PR were comparable to the impact of PH medication. The outcome measures used were those available at our PR center. Data on the 6MWT as well as the Saint George’s Respiratory Questionnaire (SGRQ) are included.
Methods
We completed a retrospective analysis of charts for patients with PH who participated in PR at our center from January 1, 2007 to December 31, 2012. Patient baseline demographics included age, gender, body mass index (BMI), ethnicity, World Health Organization (WHO) classification, and forced expiratory volume in 1 second (FEV1). Comorbidities were documented and analyzed using the Charlson comorbidity index scale. Objective evidence of the presence and degree of PH was verified by analysis of right heart catheterization (RHC) and/or echocardiogram. Pharmacologic therapies were also documented. Standard PR was comprised of 30–60 minutes of lower body aerobic training performed two to three times a week consisting of treadmill, bicycle, and cross-trainer exercises targeting a Borg scale of moderate intensity. Exercise was prescribed following an exercise tolerance test and an evaluation by the medical director of the program. Data on 6MWT before and after initiation of PH therapies were recorded as well as 6MWT and SGRQ scores before and after pulmonary rehabilitation. A biostatistician was consulted. Using STATA version 12, paired t tests were employed to analyze the metrics. Each subject served as his/her own control and in each case, the test examined the difference between the preobservation versus the postobservation with the presumption that the difference between the preobservation and the postobservation was not equal to 0.
Inclusion criteria
This study population was comprised of patients with PH who were optimized and stable on medical therapy and who subsequently completed between 17 and 36 sessions of PR. Patients averaged two to three sessions a week; details can be seen in table labeled Appendix 1. Patients with erratic attendance were included as long as attendance did not fall below one time a week.
Exclusion criteria
The following criteria were used to exclude patients from the study: Patients who were unable to do a follow-up 6MWT or who were lost to follow-up. Patients who could not complete at least 17 sessions of PR. Reasons for withdrawal from the program are detailed in Appendix 1.
Results
Study population
Of the 41 patients with PH referred for PR, 18 were excluded due to various reasons as summarized in Figure 1. Among the 23 patients, there were 14 women (61%) and 9 men (39%). Mean age was 66.9 years (SD = 12.4, range of 37–91 years). There were 14 Caucasians (60.9%), 7 African Americans (30.4%), and 2 Hispanics (8.7%). The mean BMI was 30.3 (SD = 6.9, range of 19–40). WHO classification at baseline was available in 14 patients. There were no patients in class I; 5 were in class II (36%); 8 were in class III (57%), and 1 in class IV (7%) (Table 1). Charlson comorbidity index was available in 21 of the 23 patients, with an average of 2.43 (range of 1–6). Of the 23 patients, 9 (39%) were using oxygen at baseline and postrehabilitation. An additional two patients initially naive to oxygen were subsequently found to require oxygen during rehabilitation. The change in 6-minute walk in these two patients was +73 meters in one patient and −50 meters in another. Baseline FEV1 was 56.5%; 1.24 liter (SD = 0.42 liter range: 0.63–2.08 liter). There were no changes in the use of oxygen during the initial titration of PH medication.

Patient Selection Diagram.
Demographic and clinical characteristics.

NYHA/WHO: New York Heart Association/World Health Organization; mPAP: mean pulmonary artery pressure; RAP: right atrial pressure; PCWP: pulmonary capillary wedge pressure; CI: cardiac index; 6MWT: six-minute walk test; BMI: body mass index.
RHC was available for 14 patients and echocardiographic evidence of PH was evident in the remaining 9 patients. Of the 14 patients with RHC, the mean right atrial pressure was 8.87 mmHg (SD = 4.2); cardiac index (CI) was 2.56 (SD = 0.47); mean pulmonary artery pressure was 36.60 mmHg (SD = 7.9); mean pulmonary vascular resistance was 4.27 (SD = 2.5) Wood units and mean pulmonary capillary wedge pressure was 14.33 mmHg (SD = 5.5). Of the nine patients referred to PR with abnormal echocardiograms, seven echocardiograms were available for review and had a mean pulmonary artery systolic pressure (PAS) of 61 mmHg.
Change in 6MWT before and after PH medication and PR
The 6MWT is conducted by trained staff following the American Thoracic Society guidelines using an indoor 30 meter long hallway. Starting and ending points of each 30 meter lap were clearly marked. Data were taken once subjects stated they understood the task. Practice runs were not performed. Of the 23 patients, 21 were on PH medication prior to PR, and 12 of the 23 patients had 6MWT data available. The baseline 6MWT prior to initiation of medication was 284 meter (SD = 110.8, range 91–457 meter). The mean 6MWT on follow-up after initiation of medication was 286 meter (SD = 137.8, range 61–488 meter). The change between 6MWT pre- and postmedication was not statistically significant, p = 0.95 (95%CI = −56 to 59). The baseline 6MWT prior to start of PR, n = 23, was 231 meter (SD = 105.3, range 55–365 meter). Patients completed an average of 27 sessions of PR (range of 17–36 sessions). The mean 6MWT after completing rehabilitation was 301 meter (SD = 117.0, range 60–488 meter). The difference in 6MWT before and after rehabilitation from was 70 meter, p = 0.0012 (95%CI = 30.99–109.01).
Change in SGRQ before and after PR
SGRQ scores are available for patients undergoing PR but not for the initial drug therapy period. Complete SGRQ scores prior to and at conclusion of rehabilitation sessions were available for 14 of the 23 subjects. Nine patient charts were missing from the form or did not have adequate data to merit inclusion. SGRQ scores are reported in the domains of symptoms, activity, and impact as well as a total score. Results are presented in Table 2 and Figure 2.
SGRQ before and after rehabilitation.

SGRQ: Saint George’s Respiratory Questionnaire.
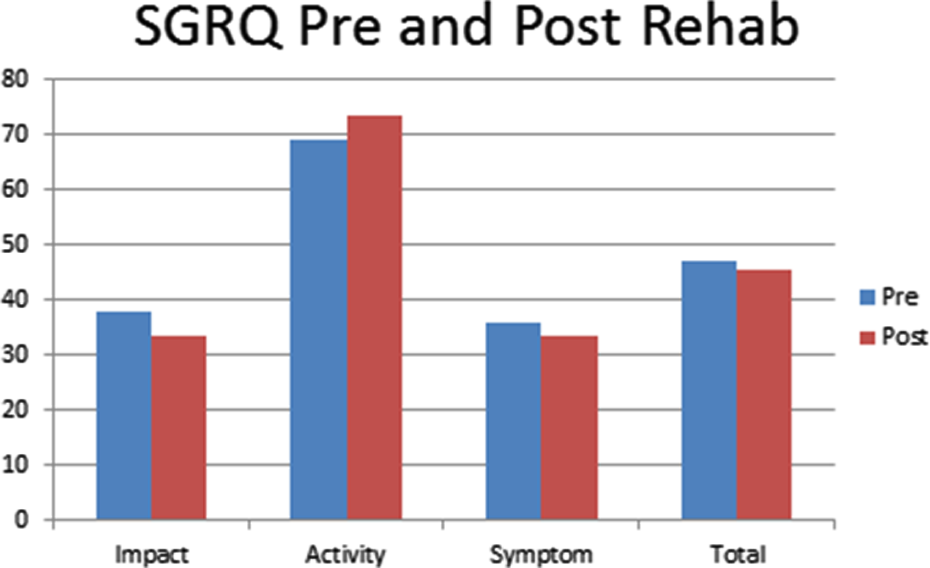
Saint George Respiratory Questionnaire outcomes pre and post pulmonary rehabilitation.
The data on SGRQ demonstrate a clinically significant improvement in the domain of impact (from 37.9 to 33.6, Δ = 4.3) and a clinically significant decline in the domain of activity (69.1 to 73.4, Δ = −4.3). The domains of symptoms (36.1 to 33.7, Δ = 2.4) as well as the total score (47.1 to 45.7, Δ = 1.4) did not meet the criteria of a delta of 4 used to acknowledge a clinically important outcome.
Discussion
PH is characterized by the progressive increase in pulmonary vascular resistance leading to cor pulmonale, decreased exercise tolerance, and decreased QOL. Advances in medical therapy have improved the prognosis of patients with PH. Recent registry data from 1982 to 2006 demonstrated an 85% survival rate at 1 year for patients with PH. 12 Exercise tolerance only partly correlates with resting pulmonary hemodynamics in PH. 13 Therefore, other factors contribute to the exercise limitation, such as morphological and functional changes in quadriceps including decreased proportion of type I fibers and lower quadriceps strength. 9 It is therefore conceivable that exercise training would improve exercise endurance and quadriceps muscle function in patients with PH. 3
PR includes a multidisciplinary approach to the treatment of patients with chronic respiratory disease who are symptomatic and demonstrate decreased tolerance for activities of daily living. 14 The data supporting its use come largely from studies involving patients with chronic obstructive pulmonary disease (COPD) and interstitial lung disease. 15,16 An emerging database is now available among patients with PH of different etiologies and the database continues to grow. Several authors have demonstrated that PR is a promising adjunct to medical treatment in PH. 2 –8 Given the heterogeneity of causes for PH, the role of PR continues to evolve, but our review of the literature consistently reveals positive outcomes for PR in the management of PH. 2 –9,17 –19
Summary of main findings
This study sets out to retrospectively evaluate the benefits of PR in comparison with pharmacologic therapy. There were 43 charts found with a primary diagnosis of PH and 23 patients met criteria for inclusion. In total, 14 patients underwent cardiac catheterization and 9 patients met criteria using echocardiogram data. In this retrospective study of patients with PH referred for PR, there was a definite benefit seen with PR (average of 27 sessions). Such benefit was assessed using the 6MWT, with an average gain of 70 meter before and after PR. This outcome is on a par with the minimal clinically important difference (MCID) in other chronic disease states, such as 54 meter in COPD 20 or 56–57 meter seen in patients with interstitial lung disease 16,21 or 25 meter in patients with coronary artery disease. 22 Our intention was to evaluate and compare the outcomes in pharmacotherapy and PR in PH and also compare it to newer data that supports an MCID of 33 meters for patients with PH. 23 In patients initiating pharmacologic therapy for PH, 41 meter has been characterized as an MCID in 6-minute walk. 24 In our retrospective analysis, we found only a 2 meter change postdrug therapy intervention. We cannot offer a plausible explanation for the lack of change in 6MWT outcomes after initiation of PH medications. Given the small number of patients who underwent a 6MWT as a part of their evaluation for pharmacologic intervention (14 of the 23 patients), it is conceivable that the varying disease states and the varying pharmacologic agents provided an inadequate sample from which to draw any meaningful conclusions.
Of note in our study in those patients undergoing PR, subgroup analysis revealed a greater gain among patients who started out with lower baseline 6MWT. Those who started out with a 6-minute walk of <250 meter (12 patients) showed an average increase in 6MWT postrehabilitation of 86 meter, p = 0.0265 (95%CI = 12.06–159.94). The remaining 11 patients who started with a baseline 6MWT of >250 meter had a statistically significant gain of 52.55 meter in 6MWT postrehabilitation, p = 0.005 (95%CI = 19.89–85.22). This finding of greater improvement in 6MWT among those with low initial 6MWT is substantially greater than anticipated. The smaller improvement in 6MWT distance among patients with higher baseline 6MWT has still achieved a level consistent with known outcomes in other chronic lung diseases. 2,6,16,25 We believe that the findings of our study are fairly unique as few studies have evaluated PH therapies and PR in a population that starts at a low baseline 6MWT. Outcomes in PH and PR are usually found in the literature with baseline results above 350 meter and gains are in the range of approximately 50 meter. 4 –6,9,26 It is worth noting that there were no untoward events seen as a result of PR in the study population over the 6-year period.
Strengths and limitations
A disparity found in our study is that despite a significant objective gain in 6MWT, the SGRQ domain of activity did not reflect this change. The SGRQ is a tool that has been validated primarily in COPD and asthma and, to our knowledge, has not been validated among patients with PH. Typical outcome measures utilized in pulmonary arterial hypertension such as The Cambridge Pulmonary Hypertension Outcome Review, Short Form 36, or Assessment of QOL were not available for review. The SGRQ was available and utilized to evaluate QOL in this chronically ill community. The domain of impact did improve, but the utility of SGRQ in PH is unclear and remains to be proven useful in this population.
The inhomogeneity of the patient population in PH will always confound outcomes as PH occurs in various disease states with overlapping conditions and comorbidities much like the realities seen in COPD. Even in COPD, PH can be a reality that has been acknowledged. 27,28 In our retrospective analysis, we employed the Charlson comorbidity index which did reveal a low score perhaps minimizing the impact of comorbidities.
Implications for future research
One potential insight our study offers is that patients with a low initial 6MWT should not be excluded from PR services as they may be able to raise their post-PR 6MWT to a level associated with better QOL and perhaps survival. 29 There is some controversy in the literature on this matter as Miyamoto et al. 30 concluded that 6MWT can be used in predicting outcomes, but a meta-analysis in 2007 found that changes in exercise capacity was not predictive of survival benefit. 31 Galiè et al. 17 considered patients whose 6MWT <332 meter as high risk for early mortality and in need of aggressive pharmacotherapy. This was further elucidated by Benza et al. in 2010, who concluded that 6MWT thresholds of >440 meter are associated with longer survival and <165 meter with increased mortality. 32
To our knowledge, there has been no other study that has evaluated the effects of rehabilitation in PH patients with baseline 6MWT <250 meter. We have demonstrated significant improvement in 6MWT in this cohort. Our study included 12 patients with an initial 6MWT <250 meter and who demonstrated an average of 86 meter improvement. This level of improvement has been seen prior but only in patients whose starting 6MWT was in a high range typically >400 meter. 4 –6,26 We believe that Δ6MWT in this cohort of patients demonstrates that PR should be offered to those patients along with pharmacotherapy and that a low baseline 6MWT should not preclude referral. It should be noted that best clinical practice should include the employment of PH medications prior the initiation of PR. This study now joins other studies demonstrating that 6MWT outcomes with PR are at least of a similar magnitude as those seen with the use of PH medication and parallel outcomes seen in other chronic lung diseases.
Conclusion
Multiple studies have demonstrated that PH patients benefit from PR. This study adds to the literature as it is perhaps the first study to prove that patients with PH and a low initial 6MWT will significantly benefit from PR services. As in other types of chronic lung disease, PH requires disease management strategies that should include referral to PR centers.
Footnotes
Appendix 1
Appendix 2
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.