
Abstract
The objective of this study was to derive and validate an equation to estimate the speed for the endurance shuttle walk test (ESWT) using results from the six-minute walk test (6MWT) in patients with chronic obstructive pulmonary disease (COPD). Participants with diagnosed COPD (n = 84) performed two incremental shuttle walk tests (ISWTs) and two 6MWTs. ESWT speed was calculated from the ISWT results using the original published method. An equation was derived, which directly related six-minute walk distance (6MWD) to ESWT speed. The derived equation was validated in a different group of people with COPD (n = 52). There was a strong correlation between average 6MWD and the calculated ESWT speed (r = 0.88, p < 0.001). The ESWT speed (kilometre per hour) was estimated using the following equation: 0.4889 + (0.0083 × 6MWD). The mean difference (±limits of agreement) between ESWT speeds was calculated using the original published method and found to be 0.03 (±0.77) km/hour. When the ISWT is not the test of choice for clinicians, the 6MWT can be used to accurately estimate the speed for the ESWT.
Introduction
Field walking tests are commonly used to evaluate the response to pulmonary rehabilitation in people with chronic obstructive pulmonary disease (COPD). The endurance shuttle walk test (ESWT) has been shown to be more responsive to change following pulmonary rehabilitation than the six-minute walk test (6MWT) and the incremental shuttle walk test (ISWT). 1 –3 To demonstrate an improvement in the ISWT or the 6MWT, a person must be able to walk faster (and/or have fewer rests in the 6MWT). In some instances, pulmonary rehabilitation may not improve a person’s walking speed but may improve their ability to walk at a constant speed for longer. This improved walking endurance, which is important for activities of daily living, can be demonstrated by an ESWT. 1
Despite the responsiveness of the ESWT to change following pulmonary rehabilitation, it has not been widely used as an outcome measure in pulmonary rehabilitation programmes. 4 –6 The necessity to perform an ISWT in order to calculate the speed for the ESWT may limit the use of the ESWT in programmes where the 6MWT is the test of choice at initial assessment.
Therefore, the aim of this study was to derive and validate an equation to estimate ESWT speed from the six-minute walk distance (6MWD) in people with COPD. If the 6MWD could be used to derive a speed for the ESWT, this would negate the need for the ISWT, thus enabling the ESWT to become more widely used for evaluating the effects of pulmonary rehabilitation in people with COPD.
Methods
Study design and population
The study was designed with a development phase and a validation phase. In the development phase, an equation (6MWDESWT) was derived, which directly related the 6MWD to the ESWT speed calculated using the original method published by Revill et al. 2 In the validation phase, data from a different group of people with COPD were used to explore the accuracy of the derived 6MWDESWT equation.
Participants for both the development and validation phase were recruited from referrals to hospital outpatient pulmonary rehabilitation programmes in two cities within Australia (Sydney, New South Wales and Perth, Western Australia). Participants were included in the study if they had a medical diagnosis of COPD according to the Global Initiative for Chronic Obstructive Lung Disease classification 7 (forced expiratory volume in one second (FEV1)/forced vital capacity (FVC) ratio of <0.7; FEV1 < 80% predicted normal), were in a stable clinical state and had a smoking history of greater than 10 pack-years. Exclusion criteria were prescription of long-term oxygen therapy, morbid obesity (body mass index > 35 kg/m2), use of a walking aid or co-morbidities likely to adversely affect performance during exercise testing. The majority of participants were naive to the exercise tests. Written informed consent was obtained from all participants. The study was approved by the ethics committees of Sydney South West Area Health Service (lead Human Research Ethics Committee), The University of Sydney, Curtin University, Sir Charles Gairdner Hospital and Bentley Hospital, Australia. The trial was registered in the Australia and New Zealand Clinical Trials Registry (ACTRN12609000472279).
Pulmonary function tests
Spirometry (FEV1 and FVC) was measured using a calibrated portable spirometer (EasyOne spirometer, ndd Medical Technologies Inc., Andover, Massachusetts, USA) according to standard procedures. 8 Lung volumes and diffusing capacity were measured by body plethysmography and the single-breath technique according to standard protocols, respectively. 9 The obtained measures were compared with normative data. 10 –12
Measurement of exercise capacity
Participants in both the development and validation groups were required to complete two ISWTs and two 6MWTs within a 7-day period. Participants performed the two ISWTs on 1 day followed by two 6MWTs on another day. Repeat tests were separated by a 30-minute rest period. For both the 6MWT and ISWT, the test that yielded the greatest distance was recorded as the test outcome. The ISWT and 6MWT were performed according to standard protocols. 13,14 The 6MWT tracks varied according to site and were rectangular (26–32 m) or straight (20–45 m) tracks. The distances achieved on the tests were compared with normative data. 15,16 In all walk tests, oxygen saturation (pulse oximeter, RAD-5v Masimo Corporation, Irvine, California, USA or Novametric, Murrtsville, Pennsylvania, USA) and heart rate (polar heart rate monitor; ©Polar Electro, Kempele, Finland) were continuously monitored in order to report nadir oxygen saturation. If oxygen saturation fell below 80% during testing, the ISWT was terminated and a rest was imposed in the 6MWT until pulse oxygen saturation returned to 90%. Ratings of perceived breathlessness were assessed using the modified Borg 0–10 point category ratio scale 17 before and at the end of each exercise test.
Calculation of ESWT speed
The speed for the ESWT was calculated as originally described by Revill et al. 2 using the incremental shuttle walk distance (ISWD). 2 For this calculation, an estimate of the peak rate of oxygen consumption (VO2peak) was derived from the ISWD using the following equation: 4.19 + (0.025 × ISWD). Thereafter, a walk speed that corresponded to 85% of the estimated VO2peak was determined from a graph that plotted the relationship between the estimated VO2peak and walking speed (kilometre per hour). 2 This speed was used to select the level for the ESWT from a table of 16 levels, with walking speeds ranging from 1.78 km/hour to 6 km/hour. If the calculated speed fell between levels, the higher level and the corresponding speed were selected.
Statistical analyses
All data are presented as mean and standard deviation unless otherwise stated. Data were analysed using Statistical Package for the Social Sciences (SPSS) software (version 20 for Windows, SPSS Inc., Chicago, Illinois, USA). The value of p ≤ 0.05 was considered significant. In the development phase, the relationship between 6MWD and the speed calculated for the ESWT (described previously) was assessed by Pearson correlation coefficients (r). To determine whether any independent variables influenced the relationship between 6MWD and calculated ESWT speed, stepwise multiple regression was performed using 6MWD, age, height (metres), weight (kilograms) and gender as independent variables and ESWT speed as the dependent variable. In the validation phase, paired sample t tests were used to determine the mean difference between the speeds for the ESWT calculated using the original method 2 and those derived using the 6MWDESWT equation. The methods described by Bland and Altman 18 were used to determine agreement and to assess for any bias between the methods.
Sample size
Based on the number of independent variables tested (6MWD, age, height, weight and gender), a sample size of 84 participants was estimated to provide adequate power (α = 0.05, power = 0.8) to detect a moderate effect size of 0.5 19 between the calculated ESWT speed using the published method and that derived using 6MWDESWT equation. In the validation phase, 50 participants were considered sufficient to determine the agreement between the ESWT speed calculated using the original method and that derived using the 6MWDESWT equation.
Results
Baseline characteristics of the development and validation groups are shown in Table 1, and data collected during the 6MWT and ISWT are shown in Table 2. All participants completed the study. Of the total participants, 11 participants in the development group and 3 participants in the validation group rested during the 6MWT.
Participant characteristics.a

BMI: body mass index; FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity; TLC: total lung capacity; FRC: functional residual capacity; RV: residual volume; D LCO: diffusing capacity of the lung for carbon monoxide.
aData are represented as mean (SD).
Exercise test data.a

6MWT: six-minute walk test; ISWT: incremental shuttle walk test; HR: heart rate; SpO2: pulse oxygen saturation.
aData are presented as mean (SD). For the 6MWT, 11 participants in the development group and 3 participants in the validation group had one or more rests.
Association between 6MWD and ESWT speed
The average speed for the ESWT calculated from the ISWT was 4.31 (0.82) km/hour, which was equivalent to 95 (9)% of average speed achieved during the 6MWT. There was a strong correlation between 6MWD and the speed calculated for the ESWT (r = 0.88; p < 0.001; Figure 1) such that ESWT speed could be derived by the following equation (6MWDESWT): ESWT speed (km/hr) =0.4889 + (0.0083 × 6MWD (in metres); R 2 = 0.78).

Scatter plot with regression line illustrating the association between 6MWD and ESWT speed calculated using the original published method. 6MWD: six-minute walk distance; ESWT: endurance shuttle walk test.
If the average speed achieved during the 6MWT was substituted for 6MWD, the equation for calculating ESWT speed was: ESWT speed (km/hr) = 0.4889 + (0.8336 × 6MWT speed; R 2 = 0.77), where 6MWT speed (km/hour) was calculated using the following equation: 6MWD (in metres) × 10)/1000.
Associations between independent variables and ESWT speed
The speed calculated for the ESWT, derived using the original method, 2 had a weak association with age (r = −0.35, p < 0.001) and height (r = 0.29, p = 0.008) and no association with weight (r = 0.15, p = 0.177) or gender (r = −0.19, p = 0.09). All independent variables except for 6MWD were excluded from the stepwise multiple regression.
Validation of 6MWDESWT equation
The average speed for the ESWT calculated using the 6MWDESWT equation was 4.32 (0.73) km/hr, which was 94 (2)% of average speed achieved during the 6MWT. Bland–Altman plots (Figure 2) demonstrated excellent agreement with minimal bias between the speeds calculated using the published method and the new 6MWDESWT equation method. The mean difference (±limits of agreement) between the ESWT speed calculated using the original method and that derived using the 6MWDESWT equation was 0.03 (±0.77) km/hr, which was not significant (p = 0.57).
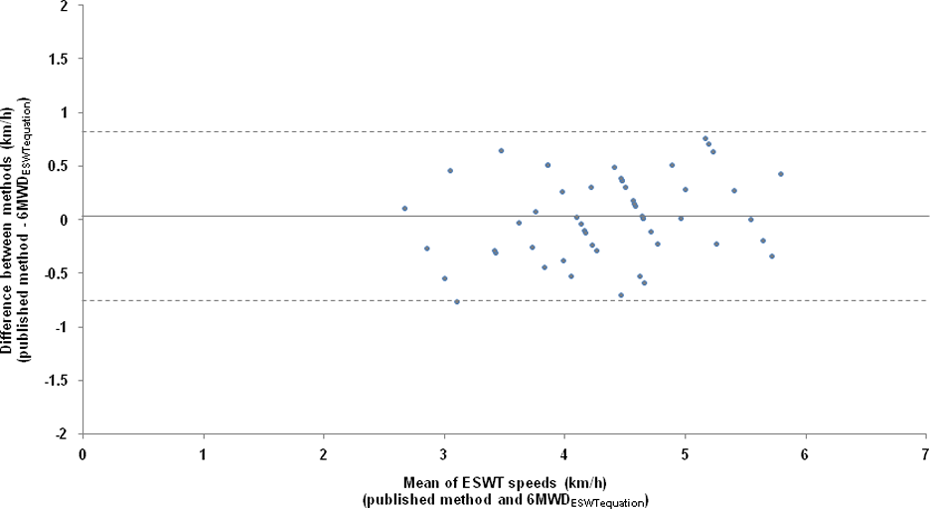
Bland–Altman plot demonstrating agreement between the speed calculated for the ESWT using the original published method 2 and the ESWT speed derived using the 6MWDESWT equation. The solid black line indicates the bias (mean difference between speeds of 0.03 km/hour). The dashed lines represent the limits of agreement (±0.77 km/hour). ESWT: endurance shuttle walk test; 6MWD: six-minute walk distance.
Discussion
To our knowledge, this is the first study to develop and validate an equation to estimate ESWT speed based on the 6MWD in people with moderate to severe COPD. In the development phase of this study, a strong association was found between the ESWT speed calculated using the original method and 6MWD. The derived 6MWDESWT equation to estimate ESWT speed was 0.4889 + (0.0083 × 6MWD). When the 6MWDESWT equation was tested on a different group of individuals with COPD, there was only a very small difference of 0.03 km/hour between the speeds calculated for the ESWT using the two methods. Only one other study has provided a method of simplifying the calculation of ESWT speed 20 but this method still requires the performance of the ISWT. Our study has demonstrated that the 6MWT could be used instead of the ISWT as the test from which to calculate a speed for the ESWT, thus making the ESWT more accessible to those clinicians who use the 6MWT as the initial screening test on entry to pulmonary rehabilitation.
For any endurance test, peak exercise capacity should first be measured from which an appropriate speed for an endurance test, such as the ESWT, can be calculated. Although the 6MWT has sometimes been regarded as a sub-maximal test and the ISWT as a peak test of exercise capacity in COPD, the 6MWT has been shown to elicit a similar peak rate of oxygen consumption and heart rate as the ISWT in people with moderate to severe COPD. 21 –23 Thus, it is a reasonable assumption that the 6MWT could be a test from which the ESWT speed could be calculated in people with moderate to severe COPD. This was further demonstrated in our study where the group in the development phase had a similar peak heart rate at the end of the 6MWT and the ISWT, providing support that the 6MWT elicited a similar cardiac response as the ISWT. The independent variables of age, height, weight and gender did not influence the 6MWDESWT equation. This was not surprising as any influence these variables had on walking capacity were likely to have influenced each individual’s 6MWD, and therefore, they did not serve to explain a greater proportion of variance in ESWT speed.
Pulmonary rehabilitation is often focused on improving an individual’s capacity to walk further (i.e. endurance) rather than to walk at a faster pace. Evidence for greater improvements in performance during the ESWT compared with the 6MWT following pulmonary rehabilitation has been previously reported. 1 –3 One study showed a mean improvement of 92% (i.e. 302 metres (95% confidence interval (CI) = 104–501) in ESWT distance compared with a 17% improvement in the 6MWD (i.e. 47 metres (95% CI = 3–90) after pulmonary rehabilitation, which included endurance training on a treadmill. 3 Not all people with COPD demonstrate a significant improvement in 6MWD after exercise training. Some studies that have used the 6MWD as an outcome measure reported that between 32% and 53% of participants did not increase their 6MWD after exercise training. 24,25 These studies suggest that participants were unable to substantially increase walking speed or reduce the number of rests required during the test following training. It is possible that the ESWT may have been a more appropriate test to demonstrate change in some of these participants.
The potential of the ESWT to provide a more responsive measure of change following pulmonary rehabilitation is important for patients, clinicians and managers, as all these groups are interested in outcome measures for pulmonary rehabilitation programmes. At present, assessment using the ESWT is limited if the ISWT is not the test of choice at initial assessment. This study has developed and validated a method to determine the ESWT speed from the 6MWT.
Study limitations
Track length for the 6MWT varied between pulmonary rehabilitation centres. Whilst track length has been shown to have an effect on 6MWD, 26 different track lengths could be regarded as enhancing the external validity of the equation due to the variety of track lengths used in clinical practice. Participants in the study had moderate to severe COPD 7 so the 6MWDESWT equation may not be applicable to individuals with mild COPD.
Conclusions
The ESWT speed derived from the 6MWD using the 6MWDESWT equation resulted in very similar ESWT speeds with those of the original published method. 2 This finding indicates that the distance walked during the 6MWT could be used instead of the ISWT to determine the speed for the ESWT when the ISWT is not the test of choice. The findings of this study make the ESWT more accessible to clinicians or researchers who commonly use the 6MWT as the test of choice at initial assessment.
Footnotes
Acknowledgements
The authors would like to thank the Pulmonary Rehabilitation Departments at Royal Prince Alfred Hospital, Concord Repatriation General Hospital, Prince of Wales Hospital, Manly Hospital, Hornsby-Kuring-Gai Hospital, Sir Charles Gairdner Hospital and Bentley Hospital for assisting with participant recruitment and for use of space for testing. The authors would also like to thank the Respiratory Medicine Departments at Royal Prince Alfred Hospital, Prince of Wales Hospital and the Department of Pulmonary Physiology at Sir Charles Gairdner Hospital for conducting pulmonary function testing.
Conflict of interest
The authors declared no conflicts of interest.
Funding
This study was supported by an Australian NHMRC project grant (Grant No.: 570814).