
Abstract
Anxiety is frequently observed in persons with chronic obstructive pulmonary disease (COPD). Although anxiety in persons with COPD is multifaceted, it is mostly assessed as a general psychopathological condition. Consequently, the objectives of this study were to revise an existing questionnaire assessing relevant anxieties for use in clinical practice and research, to examine the association between COPD-related fears and disability, and finally to develop norms for COPD-related fears. Disease severity (Global Initiative for Chronic Obstructive Lung Disease (GOLD) stage, use of long-term oxygen), sociodemographic characteristics, COPD-specific disability (COPD assessment test), and psychopathology (depression, general anxiety, somatoform symptoms, and disease-related fears) were obtained from a sample of 1025 individuals with COPD via the Internet. We used the COPD Anxiety Questionnaire (German: CAF) for the assessment of different fears that have been found to be relevant in COPD: fear of dyspnea, fear of physical activity, fear of progression, fear of social exclusion, and sleep-related worries. Mean COPD-specific disability was high (22.87). After explanatory and confirmatory factor analyses, a revised version of the CAF was constructed. The economical and user-friendly CAF-R showed adequate reliability and expected correlations with convergent and discriminant constructs. Gender-specific norms are provided for use in clinical practice and research. Even after controlling for GOLD stage, sociodemographic variables, and psychopathology, COPD-related fears contributed incrementally to disease-specific disability. The CAF-R is an economical and reliable tool to assess different specific fears in COPD. Results indicate that disease-specific fears have an impact on disability, supporting the assumption that detailed assessment of anxiety in COPD should be included in clinical practice.
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by progressive and mostly irreversible airflow limitation. Persons with COPD suffer from severe physical symptoms such as chronic dyspnea. Furthermore, COPD affects personal psychological well-being, has social consequences, and demands a successful coping concerning general physical weakness or dependency on long-term oxygen. A significant amount of COPD patients suffer considerably from psychopathological conditions. Clinically relevant anxiety disorders or combinations of anxiety and depressive disorders were diagnosed in up to 56% of COPD patients. 1 –3
Anxiety in persons with COPD is comparably high like in other end-stage chronic medical conditions (acquired immuno deficiency syndrome, cancer, and renal disease). 4 Anxious patients report a lower quality of life, higher functional impairment, and increased dyspnea during and after activity. 1,5 –9 Moreover, anxious patients have an increased risk for hospitalization. 3,10 –12 Inclusion of an assessment of anxiety in the diagnostic routine of COPD patients has been recommended. 13 Most studies investigating the effect of anxiety in COPD used more general measures for anxiety symptoms. 14 However, recent studies showed the importance of more specific and disease-related fears regarding disability and illness behavior and allocation of precise therapeutic targets. 15 –18 It has been argued that general measures of anxiety do not provide these therapeutic targets. 17 Specific fear measures have been expected to be related more closely to processes in clinical rehabilitation and to be able to predict COPD treatment outcome measures after controlling for general anxiety. 18
The effect of disease-specific fears on disability and quality of life has already been demonstrated in other chronic conditions. 19 –23 Disease-specific fears can be defined as anxiety in the face of severe physical symptoms and their consequences. 15 Kühl et al. 15 identified five important fears in persons with COPD after psychometric analysis of an item pool assessing COPD-related fears derived from expert opinion, literature, and patients’ view: fear of dyspnea (FD); fear of physical activity (FPA); fear of progression (FP); fear of social exclusion (FSE); and sleep-related worries (SRW) due to COPD. Based on these findings, they constructed the COPD Anxiety Questionnaire (CAF; German: COPD-Angst-Fragebogen).
Recent studies found evidence for the impact of disease-specific fears in COPD. It has been suggested that dyspnea-related anxiety and fearful beliefs related to exercise may help to explain patients’ avoidance of physical activity. 17,18 Anxiety and fear of exercise are associated with poorer performance in physical activity after adjusting for pulmonary function. 12,24,25 COPD patients’ FP is associated with end of life fears and lower quality of life. 26
Still, despite the importance of anxiety in COPD, there is little research about the different roles of disease-specific fears (FD, FPA, FP, FSE, and SRW) that go along with the illness. The CAF 15 allows the assessment of specific fears that have been found to be relevant in COPD, but it was only validated in a clinical rehabilitation setting with a small sample (n = 96). Furthermore, some psychometric aspects seem problematic: The item distribution is not balanced (e.g. FSE 8 items and FD 5 items) and some of the 27 items load substantially on multiple factors (e.g. item 14 loading on FP 0.58 and FD 0.48).
The aims of the current study were to improve the CAF as a tool for the reliable, valid, and economic assessment of different fears and to analyze the influence of disease-related fears on COPD-specific disability with a large sample of individuals with COPD. We modified the CAF by reducing it to 20 items, evaluated the revision, and established norms for COPD-related fears for use in clinical practice and research. More knowledge about the implications of different fears in COPD would facilitate the selection of appropriate treatment options.
Methods
Participants
Participants were assessed using an online survey promoted by a self-help organization for COPD in Germany. Data were collected between May 2012 and April 2013. No financial benefit was offered, and the participation was voluntary. The study was approved by a local ethics committee (reference number 2012-02 K). In all, 1079 volunteers with (self-reported) COPD participated in the survey. After data screening, 54 participants were excluded (n = 45; repeated participation, n = 3; age missing, n = 1; reported age of 22). Five participants were excluded due to being statistical outliers in survey execution time (13 minutes or less). Thus, the study is based on the data from 1025 participants.
Measures
Demographics and COPD status-related variables were collected in a self-developed questionnaire including age, sex, marital status, education, occupation, cigarette smoking, use of long-term oxygen, and Global Initiative for Chronic Obstructive Lung Disease (GOLD) stage. With respect to their health status, participants were asked to consult their respiratory physician in case of uncertainty.
COPD-specific disability was assessed using the COPD assessment test (CAT), 27 a standard instrument for the perceived disability concerning health status and daily life. The CAT consists of 8 items for assessing, for example, limitation of activities on a semantic differential scale (0 = I am not limited doing any activities at home, 5 = I am very limited doing activities at home). The sum score ranges between 0 (low impact) and 40 (high impact). The questionnaire serves as a short and reliable measure and demonstrates good validity. 28
For the assessment of psychopathology, the Patient Health Questionnaire (PHQ) modules for depression (PHQ-9), general anxiety (GAD-2), and somatoform symptoms (PHQ-15) 29 were used. All scales show good reliability and validity. 29 –32
COPD-related fears were measured with the CAF 15 , a 27-item questionnaire assessing specific fears and worries about the physical, mental, and psychosocial implications of COPD that we previously described. On five scales (FD, FPA, FP, FSE, and SRW), items such as “When I get short of breath, I get scared.” are rated on a 5-point Likert-type scale ranging from 0 = never to 4 = always. The CAF has good reliability ranging from α = 0.84 (FPA) to α = 0.89 (FSE) and demonstrates appropriate psychometric properties. 15 Permission has been obtained for the use and adaption of the instrument.
To examine discriminant validity, we used questionnaires measuring general cognitions about illness and the future. The Future Time Perspective 33 questionnaire assesses the perception of one’s future opportunities and remaining time. The Locus of Control About Disease and Health (German: KKG) questionnaire 34 was used as a general measure for attribution of the cause of physical complaints.
Analysis
For the revision of the CAF, item, reliability, validity, and factor analyses were executed. The CAF was analyzed with a two-way strategy. After splitting the data randomly into two subsamples, one subsample underwent an exploratory principal component analysis (PCA) with Statistical Package for Social Sciences (SPSS) for Windows (version 19; SPSS Inc., Chicago, Illinois, USA). The resulting factor solution was tested with structural equation modeling (SEM) in AMOS (version 19; SPSS Inc., Chicago, Illinois, USA) with the second subsample serving as a confirmatory method. Reliability was assessed by computing Cronbach’s α. Convergent and discriminant validity were tested with correlations. The impact of the CAF-R on disease-specific disability was then examined with regressions (hierarchical, blockwise). Finally, norms for the different scales were computed.
The values of p used in all analyses were two-tailed; p ≤ 0.05 was considered statistically significant. Due to the configuration of the survey items (mandatory) and Internet presentation, there were no missing values. Participants were allowed to pause and continue the survey at any time, but they could only continue to the next page of the survey after completion of every item. Participants had the possibility to e-mail the investigators in case of difficulties with the survey.
Results
Participants
The data of 1025 participants were analyzed. The mean age was 59.7 years (SD = 9.2), average COPD-specific disability was high (CAT score 22.87, SD = 7.73, possible range 0–40) and differed significantly between the genders, t (1023) = 4.00, p < 0.001 (see Table 1 for further sample characteristics). Only one participant e-mailed the investigator when encountering problems (server down time due to maintenance) but was able to finish the survey as well. On average the survey took 37.7 (20.1) minutes to complete.
Sample characteristics.a

CAT: chronic obstructive pulmonary disease-assessment test; COPD: chronic obstructive pulmonary disease; GOLD: Global Initiative for chronic Obstructive Lung Disease; SD: standard deviation.
aData are presented as number or percentage unless otherwise indicated.
Revision of the CAF
After statistical and content analyses, seven items were excluded due to the deductive test construction strategy: Four items that had the lowest factor loadings in the FSE scale and similarities in content (FSE 13, 15, 22, and 26; original version’s factor loading 0.47–0.69), one item from the FPA scale due to low factor loading and ambiguity with regard to content (FPA 7; factor loading 0.47 in original version), and two items with the lowest factor loadings or factor loadings on multiple factors from the FP scale (FP 11, 14; factor loading 0.50–0.57). The remaining 20 items were analyzed using PCA with oblique rotation (Promax) in the first subsample. The resulting five-factor solution replicated the one found in the original CAF validation 15 and accounted for 70% of the data’s variance. Item factor loads ranged from 0.43 to 0.94. The average communality was high (0.7).
The replicated factor solution was then tested confirmatory with a SEM in AMOS (Figure 1) with subsample two. The SEM fit indices standardized root mean residual (SRMR, 0.06), root mean square error of approximation (RMSEA, 0.06; 90% confidence interval, 0.05–0.07), the Tucker–Lewis Index (TLI, 0.94), and the comparative fit index (CFI, 0.95) indicated a good model fit. These fit indices were recommended by Hu and Bentler 35 who suggested the following cutoff criteria: SRMR ≤ 0.08, RMSEA ≤ 0.06 (both absolute fit indices, the lower the better), TLI ≥ 0.95, CFI ≥ 0.95 (both incremental fit indices, the higher the better). The χ 2 test statistic yielded significance at χ 2 (160, n = 513) = 457.37, p < 0.001.
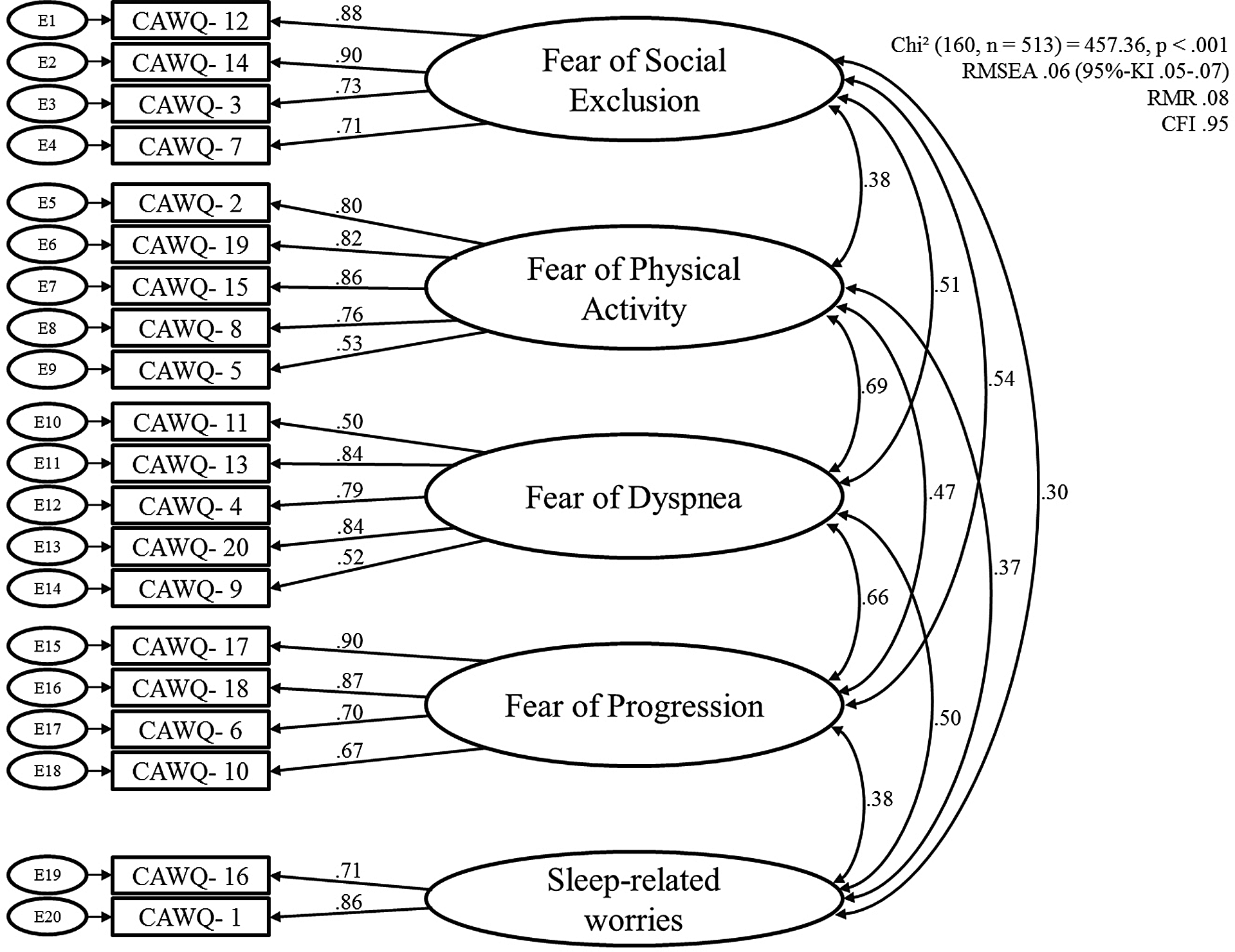
Structural equation model. Structural equation modeling was carried out with subsample 2 (n = 513); standardized regression weights are depicted between items and subscales as well as correlations among the subscales; χ 2 statistics is reported as well as fit indices RMSEA (with 95% confidence interval), RMR, and CFI. RMSEA: root mean square error of approximation; RMR: root mean residual; CFI: comparative fit index.
Reliability
All scales showed moderate to high reliability with Cronbach’s α ranging from 0.78 to 0.87. Furthermore, item-total correlations for the scales were assessed and ranged from 0.47 (FPA) to 0.82 (FP), showing adequate selectivity.
Construct validity
We analyzed Pearson’s correlations with constructs related to disease-related fears (Table 2). All scales showed the expected moderate to high correlations (r = 0.31–0.61). Correlations with discriminant constructs were generally lower (r = −0.15 to 0.34). An exception was a higher correlation between PHQ-15 and SRW (r = 0.47).
Validity and reliability of the CAF-R.a

CAF-R: chronic obstructive pulmonary disease anxiety questionnaire-revised; CAT: chronic obstructive pulmonary disease assessment test; FSE: fear of social exclusion; FD: fear of dyspnea; FPA: fear of physical activity; FP: fear of progression; FTP: future time perspective; GAD-2: patient health questionnaire general anxiety scale; KKG: locus of control about disease and health; PHQ-9: patient health questionnaire depression scale; PHQ-15: patient health questionnaire somatoform symptoms scale; SRW: sleep-related worries.
aCorrelation coefficients between CAF-R scales and convergent and discriminant constructs are presented as well as Cronbach’s α for the scales.
b p < 0.01.
c p < 0.05.
Regression
The contribution of COPD-related fears to COPD-specific disability (CAT) was analyzed with a regression analysis. In three consecutive hierarchical steps, covariates (age, gender, and smoking status), COPD status variables (GOLD stage and use of long-term oxygen), and psychopathology (PHQ-15, PHQ-9, and GAD-2) were entered cumulatively. Addition of the CAF-R scales in the final step (Table 3) improved the explained variance by 0.13 up to 0.64 (adjusted R 2). Both FPA and SRW contributed more to disease-specific disability than GOLD stage, PHQ-9, and GAD-2. Finally, the different scales were tested for their individual contribution to disability. Thus, the regression model was repeated with each scale in the last step as well as with the sum score. Every scale and overall score significantly improved the explained variance in CAT significantly with the values of p < 0.01.
Associations of COPD-related fears with disease-specific disability.a

COPD: chronic obstructive pulmonary disease; GOLD: Global Initiative for Chronic Obstructive Lung Disease; LTo2: use of long-term oxygen; GAD-2: patient health questionnaire general anxiety scale; PHQ-9: patient health questionnaire depression scale; PHQ-15: patient health questionnaire somatoform symptoms scale.
aResults from regression analyses depicting the contribution of COPD-related fears to COPD-specific disability (outcome variable: COPD assessment test, CAT). For reasons of brevity regression coefficients from the final model four are depicted. In a stepwise regression, covariates were controlled for in the first model. In the second model, COPD status variables were added and psychological symptoms were added in the third model. In the final model, COPD-specific fears (CAF-R scales) were added.
bModels’ explained variances are reported as R 2.
cSignificance of increase in models’ explained variance (p < 0.01).
Norms
Percentiles were calculated to provide norms for the CAF-R (Table 4). Due to significant gender differences in FSE, FP, and SRW (p < 0.001), norms are presented based on gender.
CAF-R norms for females and males presented in percentiles, total scores.a

CAF-R: chronic obstructive pulmonary disease anxiety questionnaire-revised; FSE: fear of social exclusion; FD: fear of dyspnea; FPA: fear of physical activity; FP: fear of progression; SRW: sleep-related worries.
aTotal scores ranged between 0 and 20 (FD, FPA), 0 and 16 (FSE, FP), and 0 and 8 (SRW).
Discussion
The high comorbidity of anxiety in COPD led to an increasing amount of research investigating its impact on disease-related disability and illness behavior. To date, specific fears have not been considered adequately. For that reason, we improved and validated an instrument to assess a variety of fears and examined the association between COPD-related fears and disability. The CAF-R is a short and reliable instrument with adequate validity. COPD-related fears contributed to disease-specific disability after we statistically controlled for GOLD stage, sociodemographic variables, and psychopathology.
As recommended, 13 clinical practitioners often assess patients’ anxiety as part of the diagnostic routine of COPD. Anxiety is mostly assessed on a broad trait level or as a general psychopathological condition. Some authors recently discussed the idea of measuring disease-specific fears to provide precise therapeutic targets. 17,18 The revised CAF measures fears found to be relevant in COPD patients. Psychometric properties were evaluated with a large sample. Both explanatory and confirmatory factor analysis indicated a good model fit of the assumed five-factor solution. It is noteworthy that the original factor solution and item distribution by Kühl et al. 15 was replicated: While their sample was collected in an inpatient clinical setting after acute exacerbation, the present sample consists of nonstationary COPD patients from all over Germany.
Due to the sample size, the present sample might be more representative of the general population for people suffering from COPD compared to the sample in Kühl et al. 15 Still, the degree to which this sample is representative is limited, because only Internet users could participate. This possibly influenced the mean age of the sample which was relatively low (59.7) for a sample of COPD patients. However, comparable mean ages were found in recent studies: Eisner et al. 12 reported an average age of 59 (SD = 6) in a sample of 1024 COPD patients, while von Leupoldt et al. 8 found a mean age of 62 (SD = 9.9) in a sample of 238 stationary pulmonary rehabilitation patients with COPD. This study provides a first set of norms for disease-specific anxieties assessed with the CAF-R. Future research should analyze to which extent these norms are generalizable for COPD samples in different settings (e.g. paper-based surveys).
Notably the reliability of the scales was not significantly reduced compared with the original CAF even though up to four items in the FSE scale were removed and seven items totally. Correlations with well-established questionnaires mostly supported the validity. Due to the lack of comparable-validated instrument measuring differential COPD-related fears, we used related constructs to show convergent validity. General anxiety and depression correlated moderately with different COPD-related fears. High correlations were not expected because the constructs used to show convergent validity were either not disease specific (GAD-2, PHQ-9) or disease specific but not assessing anxiety (CAT). More extensive diagnostic assessment of anxiety (state anxiety, trait anxiety, and general anxiety) and more direct-related constructs for the different scales (e.g. measures of social fears) would be needed to further demonstrate validity. The discriminant constructs generally showed lower correlations with the CAF-R scales with the exception of the higher correlation between SRW and somatoform symptoms (PHQ-15). This might be explained by the PHQ items “shortness of breath” and “trouble sleeping” that share content with the SRW items. Therefore, participants experiencing more shortness of breath and trouble sleeping (PHQ-15) might experience more SRW. Each specific fear tested on its own contributed significantly to disability.
Several studies indicated that anxiety in COPD impacts functional impairment. 1,3,5,9 In this study, we examined the effect of specific fears on COPD-related disability with regression analyses. We found that even after controlling for indicators of pulmonary function, confounding variables, and psychopathology, disease-related fears contributed significantly to COPD-specific disability. Each specific fear tested on its own contributed significantly to disability.
Dyspnea is an extremely unpleasant sensation and one of the main symptoms of COPD. People with COPD therefore avoid physical activities leading to exertional dyspnea. 36 Of the factors that determine dyspnea, airflow obstruction and lung function impairment show only modest associations with physical activity in daily life and exercise performance. 37,38 Our study supports the assumption that dyspnea-related anxiety and fearful beliefs related to exercise may help to explain patients’ avoidance of physical activity. Physical inactivity was shown to be the strongest predictor of mortality in COPD. 39 Hence, it is important to assess FD and FPA and to apply appropriate treatment. Higher FP is associated with more end of life fears and lower quality of life. 26 Due to the progressive and immobilizing character of the disease, persons with COPD are often afraid of the future concerning the course of the disease and social factors. The CAF-R can help identifying patients with elevated levels of FP or FSE. After identification, treatment can be derived, for example, acceptance-based strategies in case of end of life fears, discussion about realistic and unrealistic beliefs about progression of the disease, increase motivation for engagement in a self-help group to decrease fears of social exclusion.
The COPD-specific disability measured with the CAT in this sample was comparable to that found in Dodd et al. 40 in inpatients before pulmonary rehabilitation or in Kelly et al. 41 with outpatients in routine clinical practice. Lung function parameters often only moderately correlate with CAT score. 40 –42 By adding exacerbation rate, breathlessness, treatment specifics, and anthropometrics, Kelly et al. 41 could account for <40% of variance in COPD-related health status (CAT). In a regression including dyspnea score, age, body mass insex, gender, and percentage of forced expiratory volume in 1 second, Dodd et al. 40 explained 30% of variance in CAT score. With the inclusion of psychological symptoms and disease-specific fears, our regression model accounted for 64% of variance in disability.
Gender differences were found in the CAF-R FSE, FP, and SRW scale in which female participants’ mean score was statistically significant higher. Female participants also reported significantly higher COPD-specific disability in this sample. Some authors emphasized the importance of gender differences in COPD patients: Females have worse quality of life, lower subjective well-being, and more perceived dyspnea after controlling for pulmonary dysfunction. 43,44 One study also found higher general anxiety in females. 43 Higher disability and higher general anxiety in female participants in this study might partly account for the gender differences in the CAF-R scales. Although prevalence rates are rising for females, gender differences in COPD are still understudied. 45 Thus, future research should consider these differences accurately.
Some limitations of this study should be noted. First, no causal conclusions can be drawn with the present cross-sectional data. Future studies should investigate the impact of disease-specific fears longitudinally. Second, the nature of the data collection poses several problems. Self-selection biases could exist since promotion for the study took place via Web sites and e-mail lists of a support group for COPD in Germany. We tried to reduce self-selection biases by not offering a financial benefit. Participation itself was completely anonymous and voluntarily.
The online recruitment of the sample could be accompanied by more limitations, such as selectivity of the sample (Internet access necessary) and reduced reliability of the COPD diagnosis. Given the anonymity of the study, we had to rely on the participants self-ascribing the COPD diagnosis and stage. Due to promotion placement, people not directly affected by the COPD (e.g. family members) could participate in the study. We tried to reduce the risk of incorrectly self-ascribed COPD and inaccurate information about GOLD stage by adding a “status unknown” option. Participants with an unknown stage were excluded from the regression analysis.
The current study also has various strengths. The CAF-R is the first instrument to assess different relevant fears in COPD on a reliable and economical basis. It was validated with a large online sample to provide robust findings. To ensure reliability, an exemplary approach was used by testing the assumed five-factor solution both with explanatory and confirmatory factor analysis. The latter showed good model fit without any statistical restrictions being necessary. The final regression model showed that COPD-related fears contributed significantly to the disease-specific disability, even though strong predictors like depressive symptomatology and somatoform symptoms were included beforehand. Norms were calculated for interpretation of this instrument’s assessment results in clinical practice. They are also eligible as reference values for research purposes, but the generalizability is limited.
Our findings provide further evidence that detailed assessment of specific anxiety in persons with COPD should be included in clinical practice. As shown in other chronic conditions, 19 –23 we found an association between disease-specific fears and disability. The CAF-R is an economical and reliable tool for assessing different, specific fears in COPD. Further longitudinal studies and experimental research are necessary to explore the role of COPD-related fears.
Footnotes
Acknowledgment
We thank Lungenemphysem Deutschland (patient organization), especially Jens Lingemann, for supporting this study. He is the head of this patient organization and administrator of the Web pages where the hyperlinks for the online survey were provided.
Authors’ Note
Authors DCK and NMS contributed equally to this article and take responsibility for the content of the manuscript, including the data and analysis.
Conflict of Interests
The authors declared no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.