
Abstract
A systematic review was conducted to examine the association between co-morbidity and physical performance in people with chronic obstructive pulmonary disease (COPD). MEDLINE, EMBASE, CINAHL, SCOPUS and Cochrane Central Register of Controlled Trials were searched from inception to end-February 2013, using keywords ‘COPD’, ‘exercise’, ‘physical activity’, ‘rehabilitation’, ‘co-morbidity’ and individual co-morbid conditions. Studies reporting associations of co-morbidities in COPD with at least one objective measure of physical performance were included. Study quality was appraised using the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist. Nine studies met inclusion criteria. Mean (standard deviation (SD)) STROBE score was 16 (3) (maximum score = 21). Four studies examined anxiety as a co-morbid condition; three examined depression; two examined obesity and two examined a range of conditions. Reduced physical performance was associated with higher Charlson score (odds ratio (OR) = 0.72, 95% confidence interval (CI) = 0.54–0.98), metabolic disease (OR = 0.58, 95% CI = 0.49–0.67), anxiety (OR = 0.37, 95% CI = 0.23–0.59) and osteoporosis (OR = 0.28, 95% CI = 0.11–0.70). Depression had minimal association with physical performance but was associated with higher dropout rates from pulmonary rehabilitation programmes. Obesity was negatively associated with baseline physical performance but not with change from an exercise intervention. The presence of co-morbid conditions in people with COPD may negatively affect physical performance and should be identified and accounted for analysis of interventions.
Introduction
Chronic obstructive pulmonary disease (COPD) is a progressive condition characterised in the lung by airway inflammation and airflow obstruction which is not fully reversible. 1 COPD was ranked as the third leading global cause of death in 2010. 2 Clinical features include dyspnoea during physical activity, reduced exercise tolerance and symptom exacerbations that may require hospitalisation. As the condition progresses, dyspnoea and repeated exacerbations result in deterioration in quality of life. 3,4
Co-morbidity (the coexistence of one or more conditions in reference to an ‘index’ condition) is common in people with COPD. 5 In a US-based study, Mapel et al. 6 reported an average of 3.7 chronic conditions in cases with COPD compared with 1.8 chronic conditions in those without. Common co-morbid conditions in COPD include heart failure, 7 osteoporosis, 8 diabetes 9 and mental illness. 10 The presence of co-morbidity is a major determinant of functional capability, disease severity and patient outcomes for those with COPD. 5,11 Co-morbidity may also negatively influence the therapeutic management of COPD. For example, whilst corticosteroids are recommended in guidelines for the maintenance and treatment of acute exacerbations of COPD, approximately 20% of older patients with diabetes will also have COPD, thus corticosteroid use may interfere with blood glucose level and result in poor diabetes control. 12 People with multiple chronic conditions including COPD have been reported to prioritise the management of one condition over others, 13 creating challenges for management of risk factors including lack of exercise, recognising signs and symptoms of illness and managing medications.
A key non-pharmacological intervention in the management of people with COPD is pulmonary rehabilitation (PR) that consists of exercise training, education and psychosocial support. Beneficial effects of PR on exercise tolerance, symptom reduction and quality of life have been demonstrated in people with COPD. 14 Whilst depression has been associated with dropout from PR programmes, 15 the influence of co-morbidity on degree of improvement gained from rehabilitation, or baseline physical performance in people with COPD, has not been reviewed. Aspects of physical performance of interest in people with COPD include measures of exercise tolerance, functional exercise capacity 16 and physical activity levels. 17
Narrative reviews of co-morbidity in COPD have examined possible common disease mechanisms 18 and prompted consideration of the impact of co-morbidity on physical performance 19,20 but have not systematically reviewed existing literature regarding this association. Therefore, the aim of this study was to conduct a systematic review examining the association between co-morbidity and physical performance in people with COPD.
Methods
Search strategy and study selection
A primary systematic search of electronic databases, namely Cochrane Central Register of Controlled Trials (1996–February 2013), SCOPUS (1996–February 2013), CINAHL (1982–February 2013), MEDLINE (1946–February 2013) and EMBASE (1974–February 2013) was conducted. Search terms used in the major databases are listed in Table 1. Secondary searching examined the reference lists of all full text studies screened.
Systematic search strategy and terms.

COPD = chronic obstructive pulmonary disease.
aTruncation, including related terms.
Studies were eligible for inclusion if (a) participants were diagnosed with COPD (or chronic bronchitis or emphysema), (b) participants had one or more co-morbid conditions documented, (c) the study investigated how co-morbidity in COPD patients affected physical performance, (d) the study reported at least one objective outcome measure related to physical performance and (e) they were written in English.
Quality assessment
Two independent reviewers (KJ and KL) critically appraised the included studies using the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist. 21 This tool consists of 22 items that relate to study description, bias, statistical analysis and external validity. 22 One item (‘other analyses’) was combined with the ‘main results’ item, resulting in a maximum score of 21.
Data analysis
Associations between co-morbidities and measures of physical performance in people with COPD reported in the included articles were summarised. Where odds ratios (ORs) were not reported but significant associations were described using multiple regression, ORs and 95% confidence intervals (CIs) were calculated from the published data by exponentiating the unstandardised β regression coefficient (i.e. OR = exp(β)) to allow comparison of effect size between studies.
Results
The search strategy yielded 2430 records of which 2393 were excluded based on title or abstract and a further 10 were duplicates. A total of nine studies met the criteria for inclusion (Figure 1).

Flow diagram of study selection.
Quality assessment
Table 2 presents the STROBE checklist score for each included study. Scores ranged between 13 and 20 with a mean (SD) score of 16 (3). A study by Eisner et al. 10 reported how the study size was arrived at, whilst none justified sample size with power calculations. Strategies to address potential sources of bias were described in three studies. 10,25,29 Only three studies addressed the external validity or generalisability of their study results. 24,25,29
Characteristics of study participants, design and outcome measures.
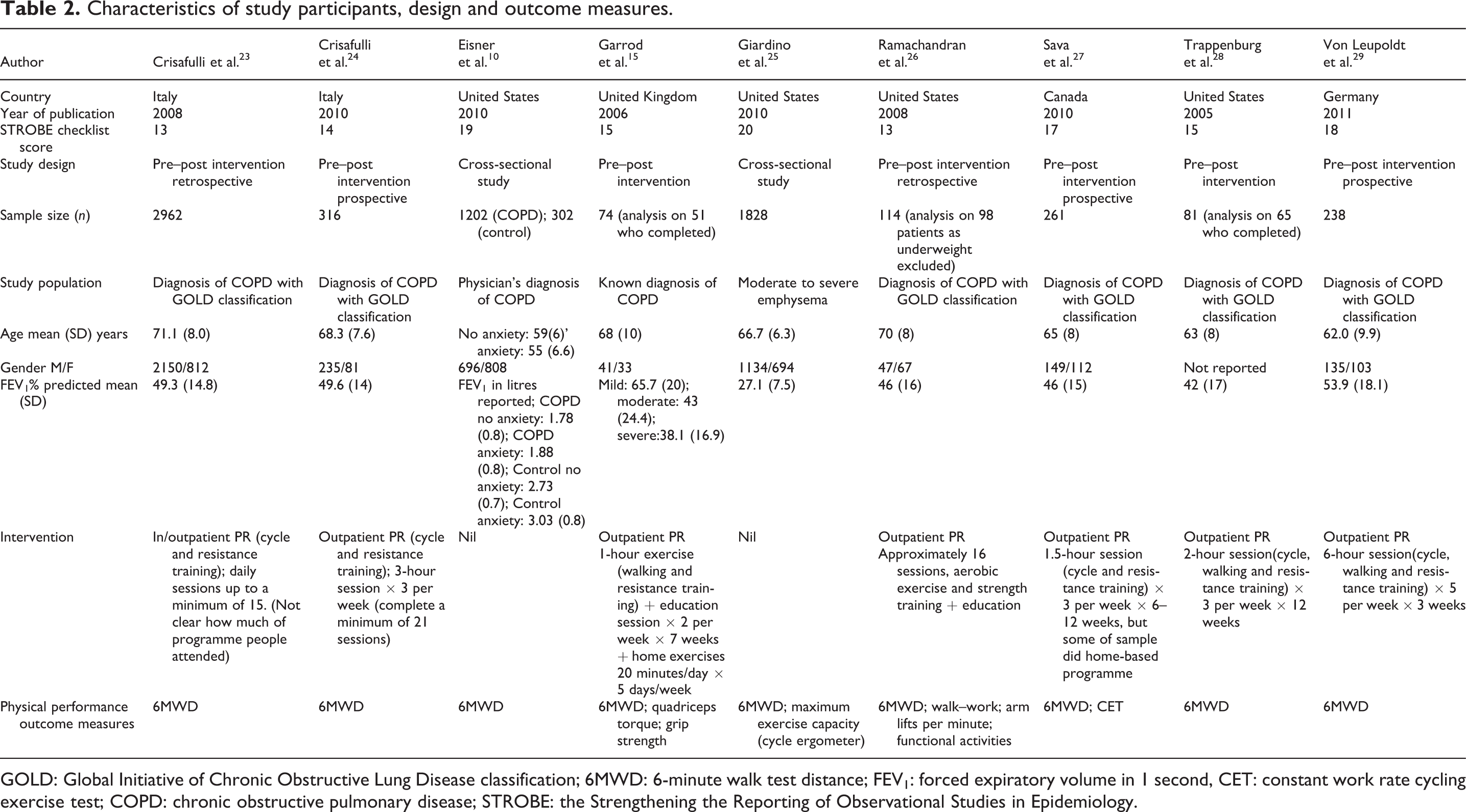
GOLD: Global Initiative of Chronic Obstructive Lung Disease classification; 6MWD: 6-minute walk test distance; FEV1: forced expiratory volume in 1 second, CET: constant work rate cycling exercise test; COPD: chronic obstructive pulmonary disease; STROBE: the Strengthening the Reporting of Observational Studies in Epidemiology.
Participant characteristics, study design and outcome measures
Table 2 presents the participant characteristics, study design and outcome measures of the included studies. The total number of patients included in 9 studies was 7076, ranging from74 to 2962 subjects per study. The mean age of participants in individual studies ranged from 55 to 71 years. The 6-minute walk test distance (6MWD) was used as an outcome measure of physical performance in all studies which met the inclusion criteria.
Two types of study design were used in the nine studies. Eisner et al. 10 and Giardino et al. 25 used cross-sectional study designs and found anxiety in COPD patients to be related to poorer health outcomes. The other seven studies 15,23,24,26 –29 measured participant’s physical performance before and after they participated in a PR programme.
Co-morbidities examined
Four studies 10,25,28,29 examined anxiety as a co-morbid condition; depression was examined in three studies 15,28,29 and obesity was examined in two studies. 26,27 A range of co-morbid conditions were examined in two studies by Crisafulli et al. 23,24 including chronic heart failure, coronary disease, diabetes, osteoporosis, dyslipidaemia and hypertension; however, mental health or obesity were not identified or examined in these studies. Details of co-morbidities examined in each study and how they were identified are included in Table 3.
Co-morbidities examined in included studies.

BMI: body mass index.
aValidated instrument.
Associations between co-morbid conditions and physical performance in COPD
Table 4 summarises associations reported between co-morbidities and physical performance in people with COPD. Inhomogeneity of statistical analyses for associations between physical performance and individual co-morbidities in the different studies prevented meta-analysis of findings. In the studies where ORs were reported or calculated, a higher Charlson co-morbidity index score had the largest negative association with physical performance (OR = 0.72, 95% CI = 0.54–0.98) 23 followed by the presence of metabolic disease (OR = 0.58, 95% CI = 0.49–0.67), 23 anxiety (OR = 0.37, 95% CI = 0.23–0.59) 25 and osteoporosis (OR = 0.28, 95% CI = 0.11–0.70) 24 in descending order. Depression only had a minimal effect on physical performance (OR = 0.003, 95% CI = 0.00–0.25). 29 The OR of the two studies on the effect of obesity on performance could not be calculated, however both authors concluded that obesity had a negative association with physical performance in COPD patients. 26,27 On the other hand, heart disease had a positive association with physical performance (OR = 2.86, 95% CI = 1.85–3.01). 23
Associations between co-morbidities and physical performance in people with COPD.

6MWD: 6-minute walk distance; MCID: minimal clinically important difference; PRP: pulmonary rehabilitation program; β: unstandardised regression coefficient; SE: standard error, OR: odds ratio; CI: confidence interval; HADS: Hospital Anxiety and Depression Scale.
aOR and 95% CI calculated from published data (regression coefficient β). All multivariate analyses accounted for effects of age, sex and lung function.
These associations are complicated by two issues. First, associations of Charlson index, metabolic disease and heart disease with achievement of minimal clinically important difference in 6MWD reported in a retrospective study by Crisafulli et al., 23 were not replicated in their subsequent prospective study. 24 Second, associations of co-morbidity are reported both with baseline measures of 6MWD (for anxiety, 10,25,29 depression 25,29 and obesity 26,27 ) and with improvements in physical performance after a PR program (for Charlson index, 23 metabolic disease, 23 heart disease, 23 osteoporosis, 24 depression 15,28 and obesity 26,27 ; Table 4).
Discussion
The findings of this systematic review indicate that the presence of co-morbid anxiety (in two cross-sectional studies 10,25 ), osteoporosis (one intervention study 24 ) or obesity (in two cross-sectional studies 26,27 , one retrospective 26 ) were associated with reduced physical performance in people with COPD. Associations with reduced physical performance were reported for metabolic disease, 23 higher Charlson index 23 and depression 25,28,29 but not found in other included studies of the same co-morbidities. 15,24 Obesity did not have an effect on the outcome of PR but was associated with lower baseline 6MWD. 26,27
The presence of co-morbid conditions is increasingly recognised as a major clinical consideration in the management of people with COPD, influencing both therapeutic management and clinical outcomes. 34 Recommendations made in clinical guidelines for COPD care are based on findings from clinical trials, which often exclude older patients and those with co-morbidity. For example, Herland et al. 35 found that a ‘typical’ clinical study would only include 17% of the ‘real-life’ asthma or COPD patient population, potentially limiting the generalisation of study findings to ‘real-life’ settings. Changes in physical performance are a common endpoint in COPD studies evaluating pharmacological 36 and non-pharmacological 37 interventions, and this review demonstrates existing evidence for the potentially confounding influence of co-morbidity on such results.
In order to control for the effects of co-morbidity on outcomes of clinical research, indices such as the Charlson co-morbidity index have been used. 38 Based on diagnosis of 17 specific conditions, the Charlson co-morbidity index is an established predictor of mortality. 38,39 However, the index does not include all conditions (e.g. depression, anxiety and obesity) and is not strongly predictive of other important health outcomes including quality of life 40 or health-care utilisation. 41 Other co-morbidity scores such as the medication based Rx-Risk score 42,43 may complement the Charlson co-morbidity index, as this includes co-morbid conditions not included in the latter, such as hypertension, anxiety, depression and osteoporosis, which are common in COPD and could negatively impact physical performance.
Two cross-sectional studies in this review 10,25 reported a negative effect of anxiety and/or depression on COPD patients’ physical performance, two reported no or negligible association 28,29 whilst one reported no significant association between baseline depression and change in 6MWD after pulmonary rehabilitation. 15 Other studies that examined obesity and multiple co-morbidities did not examine mental health issues. 23,24,26,27 If anxiety or depression were present in these patient populations, it may have had a confounding effect on physical performance outcomes. Anxiety and depression are common co-morbidities in people with COPD, with prevalence rates as high as 75% for anxiety and 71% for depression. 44 Depression has been associated with sedentary lifestyle or lack of adherence to exercise programmes in the general population. 45 Consistent with this finding, Garrod et al. 15 in an included study from this review reported greater drop out from a PR programme in participants with depression. Future studies in people with COPD that use a measure of physical performance as an outcome should document anxiety and depression and account for their presence in analysis, as these conditions may confound results and more information on the influence of anxiety and depression is required.
In one retrospective study, heart disease was associated with improved 6MWD after PR. 23 Cardiac risk factors have been shown to be reduced with a rehabilitation program. 46 PR may provide a common exercise pathway to address breathlessness during exercise, skeletal muscle dysfunction and lifestyle changes in chronic heart and lung conditions, 47 which may explain this observed association with greater benefit in 6MWD.
The primary measure of physical performance in the included studies was distance walked in the 6MWD. Whilst the 6MWD is a validated measure of exercise tolerance in people with COPD, 48 it only measures a narrow range of the physical performance spectrum. No studies were identified that examined the relationship of co-morbidities in COPD with other measures of physical performance. Future studies could examine other aspects of physical performance that might be affected by co-morbidities, for example, objective measures of physical activity or functional capacity.
Quality assessment of included studies used the STROBE checklist, which was developed to encourage authors to reported adequate information on research methods and data analysis for readers to interpret the results of observational studies with confidence. 22 Studies by Giardino et al., 25 Eisner et al. 10 (both reporting negative association of anxiety with cross-sectional 6MWD) and von Leupoldt et al. 29 (reporting no association of anxiety with cross-sectional 6MWD) had the highest scores thus greatest levels of completeness in reporting.
Co-morbidities were not identified in a uniform manner across studies included in this systematic review, except for obesity which was defined consistently with the body mass index. 26,27 Heterogeneous study designs and statistical analyses in the included studies prevented meta-analysis of associations with physical performance even for the same co-morbid condition. Associations with co-morbidity were reported in some studies with baseline measures of physical performance, and in other studies with improvement gained after a PR program. These inconsistencies in collecting and analysing co-morbidity data make it difficult to compare patient characteristics and results between studies and limit the strength of conclusions able to be drawn from this review. The inclusion of only English-language studies may have limited the completeness of this review.
Conclusion
An association between reduced physical performance in people with COPD who also have co-morbid anxiety, obesity and osteoporosis and possibly in those with metabolic disease or depression was observed in this study. This highlights the need to identify all co-morbid conditions present in those with COPD, to facilitate the development of specific strategies to ensure optimal participation in physical activity programmes and to improve exercise tolerance and health outcomes.
Footnotes
Conflict of interest
The authors declared no conflicts of interest.
Funding
This project received no specific grant from any funding agency in the public, commercial or not for profit sectors.