
Abstract
This pilot study investigated the benefits of adjunctive psychological intervention for smokers accessing standard smoking cessation interventions. Chronic obstructive pulmonary disease (COPD) smokers attending a smoking cessation service were offered up to 12 adjunctive clinical psychology sessions. Baseline data included demographics, smoking history, and disease severity. Outcomes included attendance and quit rate. In all, 59 patients with moderate COPD were referred. Of the 20 patients who attended training sessions, 7 (35%) were relapse prevention referrals and 13 (65%) were current smokers. Of the seven relapse prevention referrals, six (86%) maintained their quit, 2 of 13 (15%) of the current smoker group maintained a 28-day quit and 3 of 13 (23%) of current smokers reduced their tobacco intake. For COPD smokers with a heavy smoking history and multiple past quit attempts, there was insufficient evidence to show that additional psychological intervention leads to higher quit rates. Significant barriers to quitting and complex medical and psychosocial needs were identified in this group, suggesting that the current ‘one-size-fits-all’ approach to smoking cessation may not be sufficient to meet the needs of such a complex group.
Introduction
Chronic obstructive pulmonary disease (COPD) is the fifth biggest cause of death in the United Kingdom. 1 Smoking cessation is one of the different ways to slow down the progression of COPD, regardless of the patient’s age or disease severity. 2 Evidence-based interventions are the most effective and the most cost-effective treatment, costing approximately £2000 GBP/(Quality adjusted life year) QUALI, to support quitting smoking. 3 Smoking cessation prolongs life and postpones incapacity and is associated with a reduction in the risk of hospital admission for patients with COPD. 4 The more intensive the smoking cessation intervention for patients with COPD, the more cost-effective it is. 3 Pharmacotherapy in combination with intensive counselling has been shown to be cost saving compared with intensive counselling alone. 3
Despite clear health and economic arguments, little is known about the effectiveness of different smoking cessation interventions for patients with COPD. Jiménez Ruiz et al. 5 demonstrated that smokers with severe or very severe COPD and a high degree of physical dependence upon nicotine could achieve a 48.5% continuous abstinence rate with a combination of varenicline and intensive cognitive behavioural therapy (CBT). A Cochrane review of smoking cessation interventions with smokers with COPD found evidence that a combination of psychosocial interventions and pharmacological interventions is superior to no treatment or to psychosocial interventions alone. 6 Another Cochrane review specifically of motivational interviewing (MI) interventions for smoking cessation 7 concluded that there is modest evidence to support the use of MI compared with brief advice or usual care as a smoking cessation intervention. However, these authors concluded that more research is needed to determine what kinds of interventions are most effective for which kind of patient.
There are a number of challenges around provision of smoking cessation services for smokers with COPD. Firstly, local data suggest that uptake of smoking cessation services by smokers with COPD is very low. This study was carried out in a London borough where data from local smoking cessation services showed that only 1.4% of smokers who used the service in 2009/2010 had a recorded diagnosis of COPD. Secondly, for smokers with COPD, quit rates are low and relapse rates are high, and this population tend to have a long history of smoking, failed quit attempts and very strong nicotine addiction. 8 The proportion of people with COPD who continue to smoke despite their respiratory diagnosis has been estimated to be between 33% and 70%. 9 It is difficult to identify a national average quit rate for smokers with COPD. Coronini-Cronberget al. 10 reviewed 14 studies of smoking cessation interventions with smokers with COPD in Northwestern Europe. They cited a study carried out by Wagena et al. in the Netherlands in 2005, which found that Buproprion and smoking cessation counselling produced a quit rate of 27.3% (n = 12) versus 8.3% (n = 4) for placebo plus smoking cessation counselling. However, the numbers in this study were low. In reviewing the 14 studies, Coronini-Cronberg and co-workers stated that most of the studies excluded people with other significant conditions such as those with ‘severe co-morbidities’ or alcohol dependence issues, and therefore, the evidence identified may therefore not be generalizable to all COPD patients.
Overall, Coronini-Cronberg and colleagues concluded that there is a lack of high-quality evidence showing which smoking cessation support methods work for these patients.
Aims
The aim of this study was to determine whether a stop smoking intervention incorporating a psychological intervention in partnership with standard quit smoking support (including pharmacotherapy), specifically for smokers with COPD, resulted in higher quit rates than the average for current smokers and helped to prevent relapse for smokers who had quit but were at risk of relapse. The second aim was to characterize and better understand the factors influencing the individual’s smoking habit and barriers to cessation.
Method
Psychological intervention
The psychological intervention, delivered by a clinical psychologist with additional training in smoking cessation (level 2), was integrative, drawing on MI, CBT and mindfulness-based cognitive therapy. The intervention was formulation driven, and the clinical psychologist worked with each patient to build up an individualized understanding of the factors that kept them smoking and what skills they might need to build up to help them quit smoking or stay quit. Participants were offered up to 12 sessions, depending on the level of need, with each session lasting 50 minutes. All patients were also advised to continue to engage with local smoking cessation services in parallel. Participants who attended two full sessions or more were included in intervention numbers.
The intervention was not manualized and standardized; instead, intervention was formulation driven, that is, it was individually tailored to each participant. Formulation-driven interventions are a cornerstone of clinical psychology interventions. This approach was chosen as it allows maximum flexibility in building up an individualized understanding of the individual’s difficulties and, in this case, looking at the function of smoking for the individual and barriers to quitting particular to the individual, which was one of the aims of the study. It has been noted in previous research in the field that psychological interventions often include a variety of approaches. In a review of MI for smoking cessation, Hickman et al. 21 noted that MI interventions are often combined with other therapeutic approaches such as relapse prevention, counselling, and so on.
Standard quit smoking support
The psychological smoking cessation intervention was designed to be delivered in addition to standard smoking cessation intervention consisting of pharmacotherapy and basic counselling. The hospital-based standard smoking cessation appointments were 30 minutes long for new patients and 15 minutes for follow-up appointments. Smoking cessation advisors could offer up to eight sessions depending on the need. All study participants were advised to engage with the standard smoking cessation service. The pilot study was carried out in consultation with the local smoking cessation service who provide hospital-based and community specialist service teams, trained to level 3 smoking cessation advice with additional training during counselling. This service provides individual sessions to patients on an inpatient or an outpatient basis and group stop smoking support. Local smoking cessation advisors are also based on general practitioner (GP) practices and are practice nurses, health care assistants or GPs who have completed training in smoking cessation advice (level 2). All stop smoking cessation services provide advice on quitting, provide detailed information on available pharmacological products and can prescribe pharmacological products. All stop smoking cessation services require the patient to set a quit date by the second session.
Inclusion, exclusion and attendance criteria
Adult smokers with a confirmed diagnosis of COPD on spirometry, who accepted referral for stop smoking support, were first seen by a smoking cessation advisor and then offered a referral to the pilot program, Extra Quit Smoking and Relapse Prevention. Only patients receiving their respiratory care at the Whittington hospital or living in the borough of Islington were included in the study. The only exclusion criterion was insufficient English-language skills to attend psychology sessions without an interpreter.
Recruitment
The study was carried out between March 2013 and April 2014. A fixed date for the end of recruitment was necessary due to the time restrictions and fixed end point of the study. Referrals were accepted from Islington GP practices, the local community outreach multidisciplinary respiratory team and the local (Whittington hospital-based and Islington community-based) specialist smoking cessation teams. Referrers were notified about the project in person via attendance at general practice meetings and local COPD steering group meetings, via email GP bulletins and by short presentation about the project to the local stop smoking specialist teams.
Follow-up period
If patients did not attend, they were contacted again on one further occasion either by phone or by letter to offer another appointment. If patients did not respond to this follow-up communication, they were deemed to be ‘lost to follow-up’.
Outcome measures
Each participant was asked to complete the Hospital Anxiety and Depression Scale (HADS 9 ) at the first and the final session. Demographic information (age and gender), smoking history (number of cigarettes per day, tobacco pack years and number of previous quit attempts) and COPD severity (spirometry and Medical Research Council dyspnoea score), as well as physical and mental health comorbidities, were documented at baseline.
Final outcome measures included attendance of psychologist session, CO (Carbon Monoxide)-verified quit rate, relapse prevention or cut down and qualitative thematic analysis of the complexities of this group of smokers with COPD.
During the individual sessions, a large amount of patient information about what the barriers to quitting were for each individual was gathered and discussed. The case notes included these written formulations or shared psychological understandings of what the function of smoking was for each individual and what the barriers were. As such, formulations included important qualitative information that participants reported in individual sessions. At the end of the intervention period, a file review (using brief content analysis) was carried out on patients’ case notes in order to review themes regarding the barriers to quitting. A file review was a way of using the information generated in sessions, without having to add another means of qualitative data collection such as a semi-structured interview or focus group.
Ethics approval
This study received ethics approval from the Health Research Authority, National Research Ethics Service, West Midlands Coventry and Warwickshire and West London Review Committee (REC ref: 12/LO/1810). Local approval was also obtained from the local trust’s Research and Development Department.
Results
Attendance data
A total of 59 patients were referred to the project. Two were deemed not suitable for various reasons (e.g. one non-smoker with an addiction to nicotine lozenges and one misinformed about the purpose of the project). In all, 57 patients were accepted for treatment. Of the 57 patients, 22 (38%) accepted never engaged (i.e. did not attend any sessions with the psychologist) and 15 of 57 (26%) were lost to follow-up (i.e. patient attended one assessment session but did not attend further sessions). These figures suggest that engagement and retention are two significant challenges in targeting this population. This project was restricted by ethics approval stipulations that prohibited an assertive outreach approach.
Of the 57 patients, 20 (35%) attended two or more psychology sessions (mean = 5, range 2–12). The referred patients who engaged with the service fell into two subgroups: those who had already quit and were referred for relapse prevention (7 of 20, 35%) and those who were current smokers (13 of 20, 65%; see Figure 1).
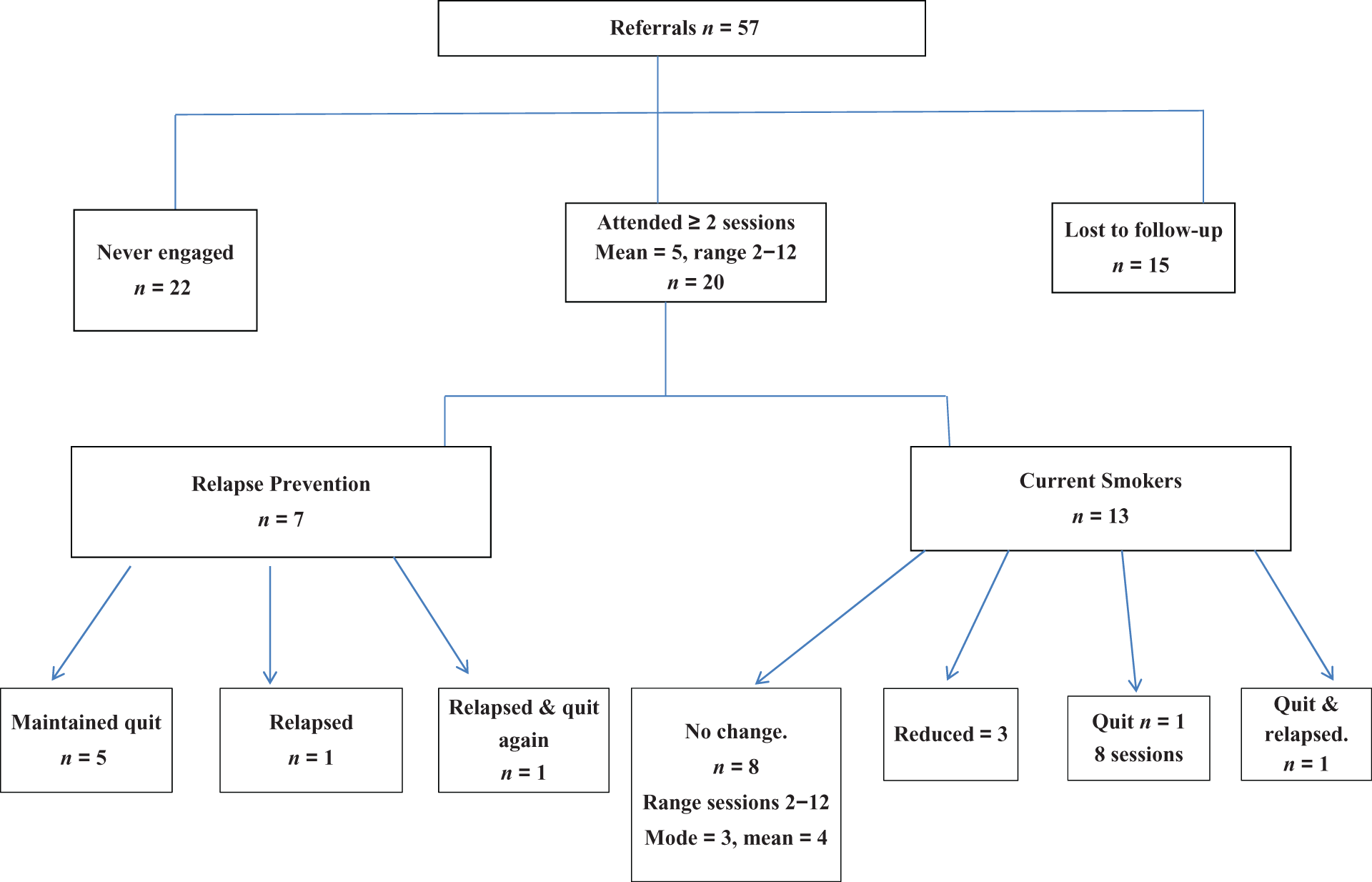
Referrals and attendance chart.
Demographic data
Participants reported 3 ± 2 (mean ± SD) previous quit attempts, with a reported range of 1 to >10 (n = 29), had moderate COPD (based on obstructive spirometry with forced expiratory volume in 1 second (FEV1) 50–79% predicted) and a high prevalence of complex physical and psychological co-morbidities (see Table 1).
Patient demographics.
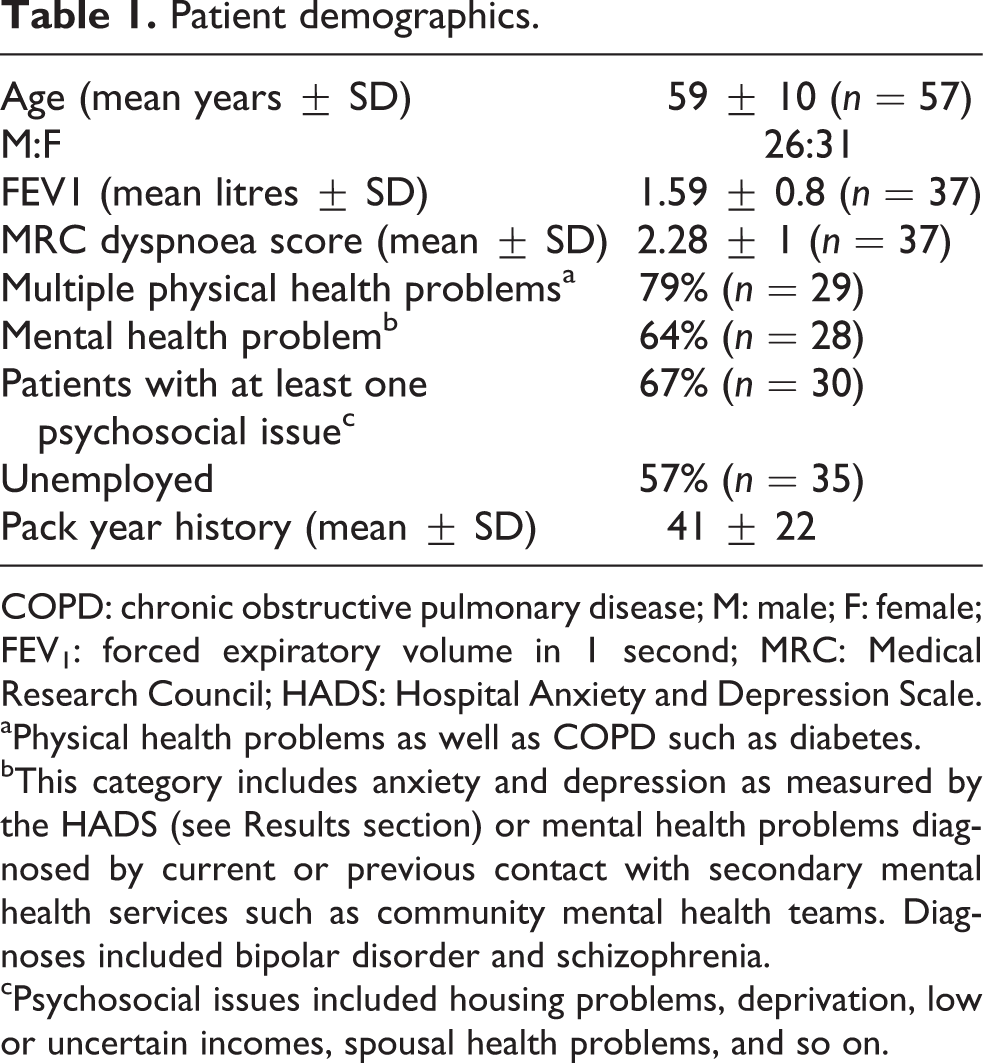
COPD: chronic obstructive pulmonary disease; M: male; F: female; FEV1: forced expiratory volume in 1 second; MRC: Medical Research Council; HADS: Hospital Anxiety and Depression Scale.
aPhysical health problems as well as COPD such as diabetes.
bThis category includes anxiety and depression as measured by the HADS (see Results section) or mental health problems diagnosed by current or previous contact with secondary mental health services such as community mental health teams. Diagnoses included bipolar disorder and schizophrenia.
cPsychosocial issues included housing problems, deprivation, low or uncertain incomes, spousal health problems, and so on.
Reported anxiety and depression
Nine of 17 (53%) participants fell into the moderate or severe range for anxiety and 7 of 17 (41%) of participants fell into the moderate or severe range for depression on the HADS self-report measure. According to the scoring criteria for the HADS, the moderate category for anxiety and depression is defined as scores of 11–14, the severe category is defined as scores 15 and above on the relevant sub-scale. As most participants did not have a planned ending, only three participants completed the post measures, preventing a meaningful comparison.
Quit rates
Of the 7 participants in the relapse prevention group, 6 (86%) maintained their quit, which includes one patient who relapsed a number of times, but went on to achieve a CO-verified quit and 2 of 13 (15%) of the current smoker group maintained a 28-day quit. However, one went on to relapse after the 28-day period whilst still engaged with the project. Due to the low numbers in this study, it was not possible to compare quit rates to national figures.
Barriers to quitting
Over the course of psychology sessions, individualized formulations were devised for each patient, with the aim of identifying factors maintaining smoking and barriers to smoking cessation. During these individual sessions, rich qualitative data emerged on the complexity of quitting for a core group of sick smokers. A content analysis of patient files revealed four main themes: Reduction versus quitting, Relapse, Co-morbid mental health problems and Early adverse experience and emotion regulation.
Reduction versus quitting
Some smokers who did want ultimately to quit, however, felt that they were unable to set a quit date.
Although some smokers reduced their tobacco intake, none wanted to engage with quit smoking services as they reported that they were not ready to quit.
Relapse
One participant from the relapse prevention group who had quit when referred went on to relapse whilst engaged with the project. In addition, one of the current smokers quit for 28 days but then relapsed also whilst engaged with the project, suggesting that the current Department of Health’s (DoH) target of measuring a quit at 28 days 11 may not capture the long-term struggle that smokers with COPD and additional complex needs have with quitting smoking.
Co-morbid mental health problems
Seven of eight (88%) of the current smoker group who were unable to reduce or quit were known to secondary or specialist mental health services. Due to high dropout rates, only 17 of 57 participants completed and returned the HADS questionnaire. Participants who did respond reported high levels of anxiety and depression. However, due to this low response rate, results must be interpreted with caution. During individual sessions with the psychologist, participants reported other mental health problems including substance misuse (drugs and alcohol), severe and enduring mental health problems (e.g. psychosis and bipolar disorder) and psychosocial problems including homelessness.
Adverse early experience
Although the project did not set out to acquire this data, during psychology sessions, many participants who were unable to reduce or quit reported adverse early experiences (ACEs) including history of trauma, childhood abuse, persecution and refugee experience. Formulation with participants who reported ACE and/or mood disorders revealed a common theme of maladaptive emotion regulation skills as a barrier to quitting smoking. Smoking was one of the few ways available for participants to regulate negative emotions. For this group, pharmacotherapy alone may not be sufficient in achieving and maintaining a quit.
Discussion
Challenges of the study
There were a number of difficulties in trying to address the main research question of whether a psychology-led smoking cessation intervention helped to improve quit rates. Firstly, recruitment and engagement were significant obstacles in this study. There were low numbers in this pilot study due to low take-up rates and high dropout rates.
There were no available data on how many patients refused referral to the project due to the challenge and inaccuracy of collecting these numbers from the diverse group of referrers to the project – hospital-based smoking cessation advisers, GPs, community-based smoking cessation advisers, respiratory team and community respiratory team. However, future studies may want to consider gathering this data to investigate how acceptable this intervention is to smokers with COPD.
To address high dropout rates, future research with this group of patients may wish to consider assertive outreach approaches in an attempt to reduce patient dropout.
Secondly, although the pilot project was designed to be adjunctive to regular smoking cessation advice, some participants did not want to attend the standard smoking cessation service, possibly due to the burden of attending both sessions. In addition, participants reported that the need to set a quit date by the second session with the smoking sessation advisor was a barrier to engagement. Some smokers expressed a wish to ultimately quit but felt unable to set a quit date. It is likely that this group would usually not access standard smoking cessation services, which require smokers to set a quit date by the second session. It may be that, for some smokers with COPD, interventions focusing on interim goals such as reduction may be another way of engaging smokers who are not yet ready to quit, as reduction may seem like a more achievable goal. Participants reported that reducing their tobacco intake gave them a positive sense of mastery as it allowed them to achieve their goals in relation to smoking. Sessions focused on reduction also gave them a space to review their smoking habits without having to commit to a quit date. There is some existing evidence to support the value of cut down to quit (CDTQ) approaches. Le Houezec and Sawe have shown that smoking reduction appears to increase the motivation to quit. 12 Smokers in the pre-contemplation stage need to progress along the stages of change 13 before becoming receptive to messages about quitting. Smoking reduction programmes may offer an opportunity to engage a large group of smokers who are in the pre-contemplation stage of change, 13 who may traditionally choose not to engage with standard smoking cessation services. It would be interesting for future research to measure stages of change and to investigate whether a ‘pre-quit intervention’ facilitates progress along the stages of change. Le Houezec and Sawe 12 note that existing smoking cessation methods target motivated smokers who are ready to quit, however, the vast majority of smokers are pre-contemplators, who are neither ready nor willing to begin a quit attempt.
A systematic review of the effectiveness of CDTQ by Wang et al. 14 noted that nicotine replacement therapy (NRT) was superior to placebo in sustaining at least 50% reduction in cigarettes smoked per day. Smokers who wished to reduce their tobacco intake were prescribed NRT, and those receiving NRT were greater than three times more likely to maintain their reduced amount of nicotine from smoking than those receiving placebo. The authors recognized that smokers who would not otherwise attempt to quit might do so if CDTQ were an option, which would be cost saving for the National Health Service (NHS).
Participants varied widely in the number of sessions they attended with a smoking cessation advisor. This caused difficulty in addressing our initial research question of whether extra psychology sessions help to improve quit rates.
Relapse
The results showed that some participants, even with added support, relapsed after maintaining a 28-day quit.
Data from ‘healthy smoker’ populations show that relapse is the rule rather than the exception and that three quarters of people who quit smoking relapse. 15 Smokers with COPD and additional complex needs may require sustained and targeted intervention beyond the current DoH 28-day guidelines. One of the challenges with providing extended support will be balancing this with low attendance rates. The relevance of the current national 28-day quit target as a marker of success is questionable for smokers with COPD. It may be that for this group, quitting smoking is conceptualized as an ongoing process rather than a one-off event.
Co-morbid mental health problems
This pilot study set out to offer smoking cessation interventions to a non-mental health population. We were surprised by the high level of co-morbid mental health problems and histories of adverse childhood experience.
Mental health problems are one of the most-cited risk factors for nicotine dependence. 16 Smokers with current or past depression are often more nicotine dependent, more likely to experience negative mood changes following nicotine withdrawal and more likely to relapse than the general population. 17 A meta-analytic review of smokers with COPD and current/past depression showed that additional psychosocial mood management input with standard smoking cessation increases cessation rates in smokers compared with standard smoking cessation treatment only. 18 Aubin et al. 18 argue that flexible, open-ended approaches combining pharmacotherapy and talking therapy may be more suitable for smokers with mental health difficulties. Screening all smokers for mood problems both past and current may be useful in identifying those who may benefit from additional psychosocial mood management and longer, more intensive support.
van der Meer et al. 17 advocate that health-care teams should consider the maltreatment history and depression status of their patients when patients report multiple failed attempts to quit smoking. Educating health-care professionals and smoking cessation advisers on the literature around the link between early adverse experience and smoking and factors associated with quitting may facilitate more effective interactions with COPD smokers with such histories.
Research suggests that ACEs including abuse (emotional, physical and sexual), neglect (emotional and physical) and household dysfunction (e.g. substance abuser in the household, incarcerated household member, domestic violence, etc.) have a long-term impact on children’s development and can lead to adoption of unhealthy coping behaviours throughout the lifespan. 19 The more ACEs patients experienced in life, the more likely they were to smoke. 20 The magnitude and complexity of the relationship between ACEs and smoking is only beginning to be understood; however, research conducted thus far suggests that ACEs are strongly and significantly associated with early smoking initiation, smoking maintenance, heavy smoking and lifetime smoking.
Teaching smokers with ACE and/or mood disorders additional skills in emotion regulation may help to facilitate a quit. This recommendation is echoed by a meta-analytic study by Bartlett et al. 13 of smoking cessation interventions for COPD patients. Bartlett et al. concluded that building self-regulation skills are particularly important for this group and is key to moving towards a quit. Interestingly, they also found that boosting motivation and self-efficacy in this group was contraindicated, and it seems that for this group skills plus will is a core message for quitting.
Further research is needed into incorporating emotion regulation skills building into specialist smoking cessation services for this group. Such an intervention would need to be measured and evaluated.
Considering the interrelationships between mood disorders, ACEs and emotion regulation problems, future research with smokers with COPD may benefit from investigating models of multi-agency working when providing smoking cessation services targeting smokers with COPD and any of the above difficulties. Such a model could include working alongside respiratory psychologists and local psychology services, in addition to GPs in order to access other agencies and services who can offer psychological or psychosocial interventions in parallel, which may facilitate smoking cessation/reduction at a later date.
Conclusion
This study demonstrates that providing an adjunctive psychological intervention alongside standard quit smoking support (pharmacotherapy and counselling) does not increase the poor quit rates for COPD smokers. Whilst the apparent barrier is resistance to engage with this intervention and to retain those who start, the difficulties are more likely related to the complex needs of this group of patients, whose narrative is one of multiple quit attempts in the past, numerous co-morbid physical and mental health problems, histories of early adverse experiences and other psychosocial issues. As smoking cessation is the most effective and cost-effective treatment for these smokers, the challenge is to design novel stop smoking services that address these needs, and we have made some recommendations to address this.
Footnotes
Acknowledgements
The authors thank Sejal Patel, Aleda Erskine and Beverley Flint for their supervision and support at various stages of the project and also thank Julie Browne for her input into the development and planning of the project.
Funding
This study was funded by NHS Islington (grant number 5K8000).