
Abstract
Pulmonary rehabilitation includes upper and lower extremity exercise training. While validated tests such as the six-minute walk distance (6MWD) and shuttle walk tests are available to evaluate the effectiveness of lower extremity training, the optimal method of evaluating the effectiveness of upper extremity training has not been determined. This study evaluates the potential utility of unsupported arm lifts (UALs) testing as an outcome measurement for pulmonary rehabilitation. Records of chronic obstructive pulmonary disease (COPD) patients who underwent outpatient pulmonary rehabilitation at our institution were reviewed. Outcomes assessed before and immediately after the intervention included 6MWD, the self-administered Chronic Respiratory Questionnaire (CRQ-SA), and UALs. For the latter, the patient repeatedly raises a wooden dowel from thigh to arm level, with the number of repetitions per minute used as the outcome. Changes in variables from pre- to post-pulmonary rehabilitation were analyzed using paired t test. Pearson correlation coefficients were used to evaluate associations. Of the 241 patients, 51% were male. Mean age was 69 ± 9 years, body mass index was 28 ± 7 kg/m2, and forced expiratory volume in 1 second was 50 ± 20 percent-predicted. All studied variables increased significantly post-pulmonary rehabilitation: the 6MWD by 45 ± 50 m (effect size 0.49), the CRQ-SA total score by 0.84 ± 0.86 units (effect size 0.89), and UAL by 12 ± 13 lifts/minute (effect size 0.75; p < 0.0001 for all). As a measure of upper extremity exercise capacity, UAL appears to be responsive to the comprehensive pulmonary rehabilitation intervention. Using effect sizes, the degree of improvement appears to be between that of 6MWD and CRQ-SA. UAL may be a useful outcome assessment for pulmonary rehabilitation in COPD patients.
Keywords
Introduction
Goals of pulmonary rehabilitation include reducing symptoms, optimizing functional status, increasing participation, and reducing health-care costs. 1 In general, these positive outcomes are accomplished through exercise training, self management education, and psychosocial support. Measurements of lower extremity exercise capacity, such as performance on the six-minute walk distance (6MWD) or Shuttle Walk tests, have traditionally been emphasized in pulmonary rehabilitation. However, pulmonary rehabilitation professionals have long recognized the importance of upper extremity training 2,3 because many activities of daily living (ADLs) involve the arms, and this type of exercise often is very dyspnea-inducing. 2
Since upper extremity training is an integral component of comprehensive pulmonary rehabilitation, 1,4,5 consideration should be given to measuring its effectiveness. Outcome assessment in this area has involved a variety of approaches, including arm ergometry, a six-minute ring test (6MRT; moving rings over a six-minute period), counting the number of unsupported arm lifts (UALs; with or without weights) over a prescribed period of time, and indirectly through evaluating ADL performance in areas that involves the upper extremities. 2,6,7
The optimal method for determining the effectiveness of the upper extremity training component of comprehensive pulmonary rehabilitation remains to be determined. The ideal outcome assessment would be simple to administer, reliable, valid, and have demonstrated responsiveness to the therapeutic intervention. Our pulmonary rehabilitation program routinely measures the number of UALs (UAL test) as part of its rehabilitation outcome assessment. We reviewed our experience with this simple-to-perform assessment, with a view toward determining its evaluative properties in this setting.
Patients and methods
Institutional Review Board approval was obtained for this retrospective analysis. We reviewed data, over a 5-year period up to 2009, on outpatient pulmonary rehabilitation patients who had chronic obstructive pulmonary disease (COPD) as a clinical diagnosis, completed our outpatient program, and had pre- and postrehabilitation outcome assessments. The indication for pulmonary rehabilitation at our institution is persistent respiratory symptoms or functional status limitation despite otherwise standard medical therapy. Our program is comprehensive and multidisciplinary and consists of sixteen 3-hour sessions over 8 weeks. It includes initial clinical and laboratory assessments, exercise training, educational sessions, psychosocial support, and outcome assessment.
The exercise training component, which is approximately 90 minutes per session, is individualized to the patient, based on clinical assessments, incremental cardiopulmonary exercise testing, and 6MWD testing. It includes lower extremity training on the treadmill and cycle ergometer and upper extremity training using an arm ergometer and free weights. Vital signs are measured before exercise and, when-indicated, during and after the sessions. Dyspnea ratings, assessment of other symptoms (such as pain or fatigue), and oxygen saturation are measured before and during the sessions and at other times when clinically indicated. Exercise intensity on the exercise equipment is adjusted primarily based on dyspnea ratings, with a general goal to have a Borg dyspnea rating of approximately 5–6 on a 10-point scale. Supplemental oxygen is supplied for those with hypoxemia at rest or those with exercise-induced hypoxemia identified by pulse oximetry. In addition to the formal upper and lower extremity training described above, all patients participate in classroom calisthenics sessions. These 45 minute sessions include relatively light intensity upper and lower extremity training, including arm lifts, stretching, lifting light weights, and sit-to-stand exercises. The classroom calisthenics in our program have been described previously. 8
Routine outcome assessments in our program include the 6MWD test, the self-administered Chronic Respiratory Questionnaire (CRQ-SA), 9 and the UAL test. These outcomes were measured immediately before and at the termination of the pulmonary rehabilitation program by the same registered nurse. The 6MWD test was performed in a long corridor in the pulmonary section, using standardized encouragement at approximate one-minute intervals. Practice attempts were not given. Patients using supplemental oxygen carried their own portable unit or wheeled a portable tank. The CRQ-SA is a self-administered, 20-item questionnaire with dyspnea, fatigue, emotion, and mastery domains as well as a total score. We analyzed the mean, per-unit total score, which can range from 1 (greatest impairment) to 7 (least impairment). The CRQ-SA instrument is highly sensitive to the pulmonary rehabilitation intervention. 10 The UAL testing has been described previously. 8 Briefly, for UAL testing, the patient stood upright and repetitively raised a wooden dowel from a position resting at the thighs up to eye level, while the arms were kept straight at the elbows. The number of completed lifts in one minute was recorded as the outcome. No practice sessions were given, although the procedure was demonstrated in detail to the patient by the registered nurse immediately prior to testing.
Data are expressed as means ± SD. Changes in variables from pre- to postrehabilitation were analyzed by paired t tests. Pearson’s correlation coefficients were used to evaluate associations. Effect size was used to compare the magnitude of change among the outcome measures. This was determined by dividing the mean pre- to postrehabilitation difference in the variable using the SD of either value. 11 We used the SD from the pre-rehabilitation measurement for this determination. The following categories were used to quantify effect sizes: <0.1 = trivial effect; 0.1–0.3 = small effect; 0.3–0.5 = moderate effect; >0.5 = large difference effect. 11
Results
Data from 373 patients referred to pulmonary rehabilitation with clinical diagnoses of COPD were reviewed. Of these, 241 (65%) had postrehabilitation outcome assessments and were included in this analysis. Their mean age was 69 ± 9 years, body mass index (BMI) was 28 ± 7 kg/m 2 , and forced expiratory volume in 1 second (FEV1) 50 ± 20 percent-predicted. Of all, 44% had been prescribed supplemental oxygen; 51% were male. Compared with females, males were older (71 ± 9 vs. 68 ± 9 years, p = 0.008). There was no significant gender difference in BMI, FEV1 percent-predicted, and oxygen requirement.
Baseline assessments are given in Table 1. The mean number of UALs per minute was 40 ± 15. Males performed significantly better than females on this test: 48 ± 17 versus 35 ± 12 lifts/minute, respectively, p < 0.0001. Figure 1 gives the frequency distribution of arm lifts. Similarly, males performed better on the 6MWD test and the CRQ total score. At baseline, UAL did not correlate significantly with age, BMI, or FEV1 percent-predicted, but did correlate directly with the six-minute walk distance (6MWD) (r = 0.48, p < 0.0001) and the CRQ-SA total score (r = 0.21, p = 0.001).
Baseline assessments.

CRQ: Chronic Respiratory Questionnaire (mean per question scores are given).
a p values refer to male–female differences.
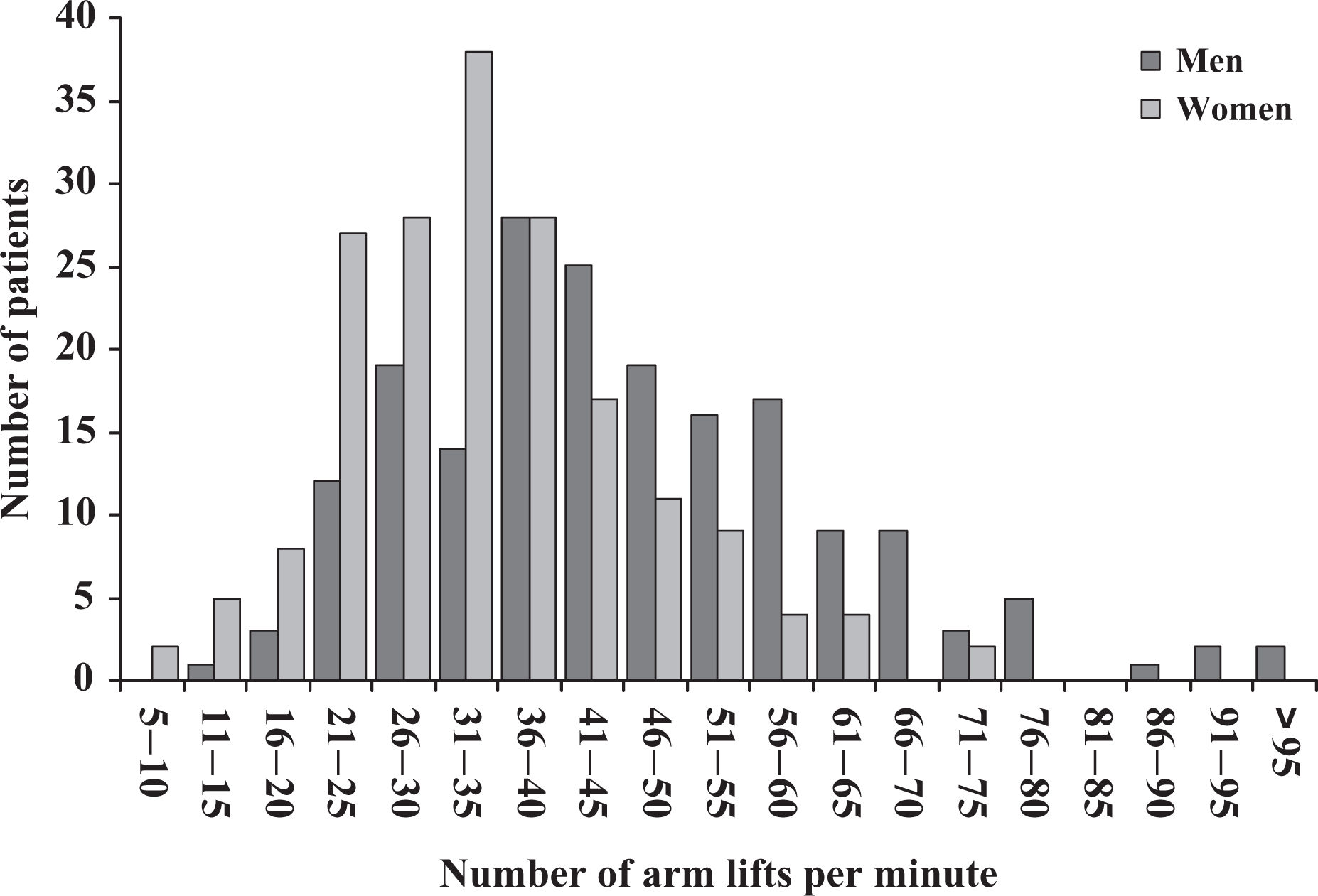
Frequency distribution of arm lifts at baseline determination.
Pre- to postrehabilitation changes in outcomes are given in Table 2. Significant pre- to postrehabilitation improvements were noted in all three outcome areas. UAL increased by 12 ± 13 lifts/minute (p < 0.0001); this amounts to a 29% increase over baseline. Although baseline values differed, absolute improvements were nearly identical in males and females in this outcome variable. Figure 2 gives the frequency distribution of changes in this variable. While there was no gender difference in change in UALs, females had greater increases in the 6MWD than males, and tended to improve to a greater degree in the health -status assessments.
Pre- to postrehabilitation changes in outcomes.a
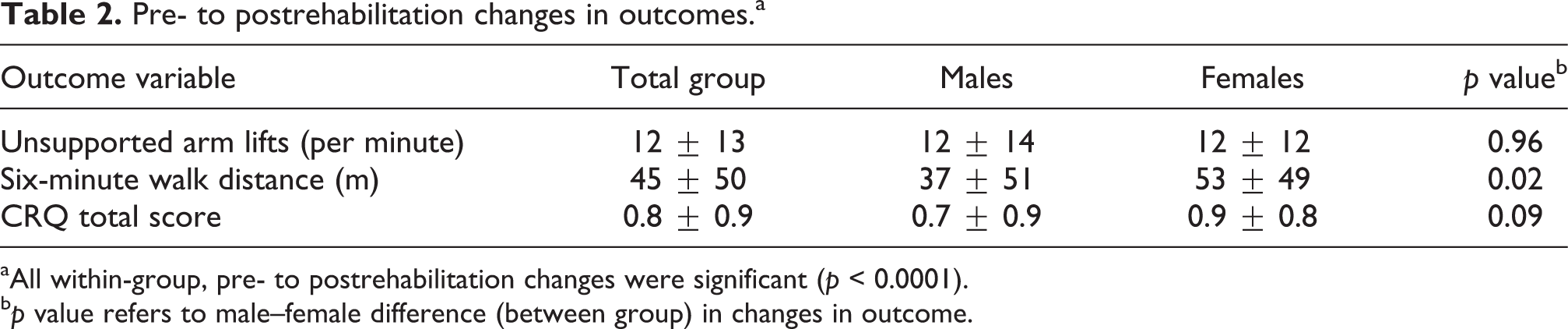
aAll within-group, pre- to postrehabilitation changes were significant (p < 0.0001).
b p value refers to male–female difference (between group) in changes in outcome.

Frequency distribution of changes in arm lifts following pulmonary rehabilitation.
Effect sizes for the pre-to postrehabilitation changes in outcome variables are as follows: 0.75 for UALs, 0.49 for the 6MWD test, and 0.89 for the CRQ-SA total score. The effect sizes for the UAL test and CRQ-SA are considered large effects while the effect size for the 6MWD test is considered moderate. 11
Discussion
The purpose of our study was to evaluate the effectiveness of the UAL as an outcome measurement for pulmonary rehabilitation in patients with COPD. Our analysis from this retrospective study revealed that UAL indeed appears to be responsive to the comprehensive pulmonary rehabilitation intervention. Furthermore, using effect size to compare changes, the degree of responsiveness of the UAL (0.75) appears to be situated between that of the 6MWD (0.49) and the CRQ-SA (0.89). These findings suggest that the easy-to-administer UAL might have utility as an assessment for the pulmonary rehabilitation of COPD patients.
At baseline assessment, males significantly out-performed females in UAL, an effect that is probably due to increased upper extremity muscle mass in males. Increased muscle mass is also probably responsible in part for the higher 6MWD that we observed in males, although a longer stride length may also be an important factor. 12 Our observed gender difference in baseline quality of life has been noted previously. 13 Despite differences in baseline performance, the improvement in UAL (12 lifts) was virtually identical in the genders.
Since the upper extremities are important in many ADLs, measuring upper extremity function would appear to be an important outcome. In a study evaluating the effectiveness of upper extremity training in pulmonary rehabilitation, Ries et al. 6 measured upper extremity exercise capacity in three ways: (1) symptom-limited peak exercise capacity and endurance capacity using arm ergometers; (2) upper extremity performance (shoulder flexion and abduction) requiring repeatedly lifting free weights up to a fatigue limit; and (3) a simulated ADL test using three standardized tasks that require upper extremity work. Upper extremity training improved performance on arm ergometry and arm lifts, but there was no improvement in the ADLs. Costi et al. 3 used a 6MRT and an ADL field test similar to that described by Ries et al. 6 as outcome measures in their study evaluating the effect of unsupported upper extremity exercise training in patients with COPD. Originally described by Celli et al., 2 the 6MRT counts the number of rings moved from one place to another over this time period. Both these tests showed responsiveness to the intervention. A recent systematic review of arm exercise capacity as an outcome in COPD; types included arm ergometry, ring shifts, dowel lifts, proprioceptive neuromuscular facilitation, and ADLs. Studies using UALs varied considerably in methodology, and most did not assess measurement properties. The review concluded that arm ergometry may be the best method for measuring arm exercise capacity and endurance. 14
Our study represents a “real world” analysis of the responsiveness of UAL to the pulmonary rehabilitation intervention. It is limited by its retrospective design and the fact that it does not include an untreated, randomly allocated control group. Furthermore, since practice attempts were not provided for either test of exercise capacity, it cannot be determined how much of the change was due to learning effect. Finally, this analysis focused on the responsiveness, not the reliability or the validity of this measurement.
In summary, we demonstrated that UAL as an outcome measurement is responsive to pulmonary rehabilitation in patients with COPD. Its responsiveness is on a par with the 6MWD test and the CRQ-SA. Since it is easy to administer, it may complement assessments in other areas such as lower extremity function and health status. Further studies, comparing test–retest results, determining the applicability to other rehabilitation sites, and relating this outcome to other areas of functional status would be necessary before firm conclusions regarding its usefulness could be made.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.