
Abstract
Aim: To study the long-term benefits of ambulatory oxygen (AO) in combination with pulmonary rehabilitation (PR) in chronic obstructive pulmonary disease (COPD) patients experiencing exertional desaturation. Patients and methods: Normoxaemic COPD who participated in outpatient PR and desaturated >4% and <90% during endurance shuttle walk test (ESWT) were randomised to control (n = 23) or AO 2 L/min from a portable oxygen concentrator (n = 22) to be used during exercise. PR consisted of supervised training for 20 weeks combined with unsupervised daily training at home followed by 13 weeks without supervised training. Results: Only 45 of 165 eligible patients wanted to participate. Mean forced expiratory volume in 1 s = 32% (SD 13.8) and Medical Research Council (MRC) = 4.5 (3–5). Supplemental oxygen improved oxygen saturation during ESWT by 2.3% (95% CI: 1.2%–3.5%; p < 0.001). In the study period of 33 weeks, 10 and 6 patients withdrew from the AO group and control group, respectively. Patients spent an average of 7.9 h/week on oxygen. PR improved ESWT by 18,076 s (95% CI: 101–258 s; p < 0.001) and St. George’s Respiratory Questionnaire (SGRQ) score by 2.6 units (95% CI: 0.1–5.1 s; p = 0.04) after 7 weeks, and these gains remained at 33 weeks of evaluation. There were no differences between the AO group and control group at 33 weeks of evaluation with regard to change in ESWT (223 vs. 241 s; p = 0.32), change in SGRQ (−3.6 vs. −4.5 units, 0.91), and number of patients with acute exacerbation in COPD (AECOPD), hospital admission or dropout (17 of 22 vs. 20 of 23, p = 0.59). Conclusions: AO seems not to provide additional beneficial effects in patients with COPD participating in pulmonary rehabilitation and experiencing exertional desaturation without severe resting hypoxaemia.
Introduction
Long-term use of supplemental oxygen improves survival and reduces hospitalization in patients with chronic obstructive pulmonary disease (COPD) and severe resting hypoxaemia.1–3 However, the effect of oxygen treatment in COPD patients with moderate hypoxaemia at rest and desaturation during activity is less clear. In these patients, studies have shown an acute beneficial effect of supplemental oxygen on ventilation, dynamic hyperinflation, breathlessness, and exercise performance. 4 Therefore, international guidelines recommend supplemental oxygen to COPD patients who desaturate >4% with activity and below 88–90%,5,6 especially if oxygen during exercise improves the physical tolerance. 7 Oxygen desaturation during a 6-min walk distance (6MWD) is seen in nearly half of all COPD patients referred to an outpatient pulmonary rehabilitation (PR), 8 and one would expect that supplemental oxygen enhanced the effects of rehabilitation in these patients. Yet, the few studies of supplemental oxygen in this group have been insufficient to demonstrate any significant benefit,9–13 but they have various methodological weaknesses. All studies have been of small size and short observation (6–10 weeks), and the oxygen has only been available during the supervised training.10–13 Only in one of the studies, was the exertional desaturation an obligate inclusion criterion 12 ; and in another study, patients with desaturation below 88% were excluded. 13 In two studies, exercise intensity was adjusted to avoid desaturation.10,11
The aim of the present study was to evaluate the long-term effects of supplemental oxygen in COPD patients with moderate hypoxaemia at rest and exertional desaturation. The patients participated in PR and had supplemental oxygen available at home to use as much as possible during exercise and physical activity.
Material and methods
Selection of patients
Eligibility criteria included stable COPD (forced expiratory volume in 1 s (FEV1) <80% and FEV1/forced vital capacity (FVC)<70%; Medical Research Council (MRC) score 3–5; motivated for PR; oxygen saturation at rest above 90%, desaturation >4% and below 90% during incremental shuttle walk test (ISWT) or endurance shuttle walk test (ESWT). Exclusion criteria included long-term oxygen therapy (LTOT), significant musculoskeletal, cardiac, or cognitive problems.
In the study period from March 2007 to March 2011, 391 patients started PR at our centre, and 163 eligible patients were encouraged to participate in this randomised controlled trial (Figure 1). Only 45 (27.6%) patients accepted the invitation and were randomised to either ambulatory oxygen (AO) (n = 22) or to a control group (n = 23) in blocks of 6, using sealed envelopes.

Flow chart of patients who entered the study.
Rehabilitation programme
The programme consisted of supervised walking and cycling twice a week for 7 weeks combined with unsupervised daily training at home. 14 Patients were instructed to exercise 30 min (including warm-up, breaks, and cool down) at a level equal to 85% of a predicted peak VO2 as calculated from the ISWT. 15 The training was supplemented with educational sessions once a week. 16 This programme was followed by maintenance training once a week for 3 months at the hospital and additional 3 months without supervised training (Figure 2). Patients were instructed to continue the unsupervised training at home at least 30 min every day during the whole study period. PR and transportation to the training centre were free.
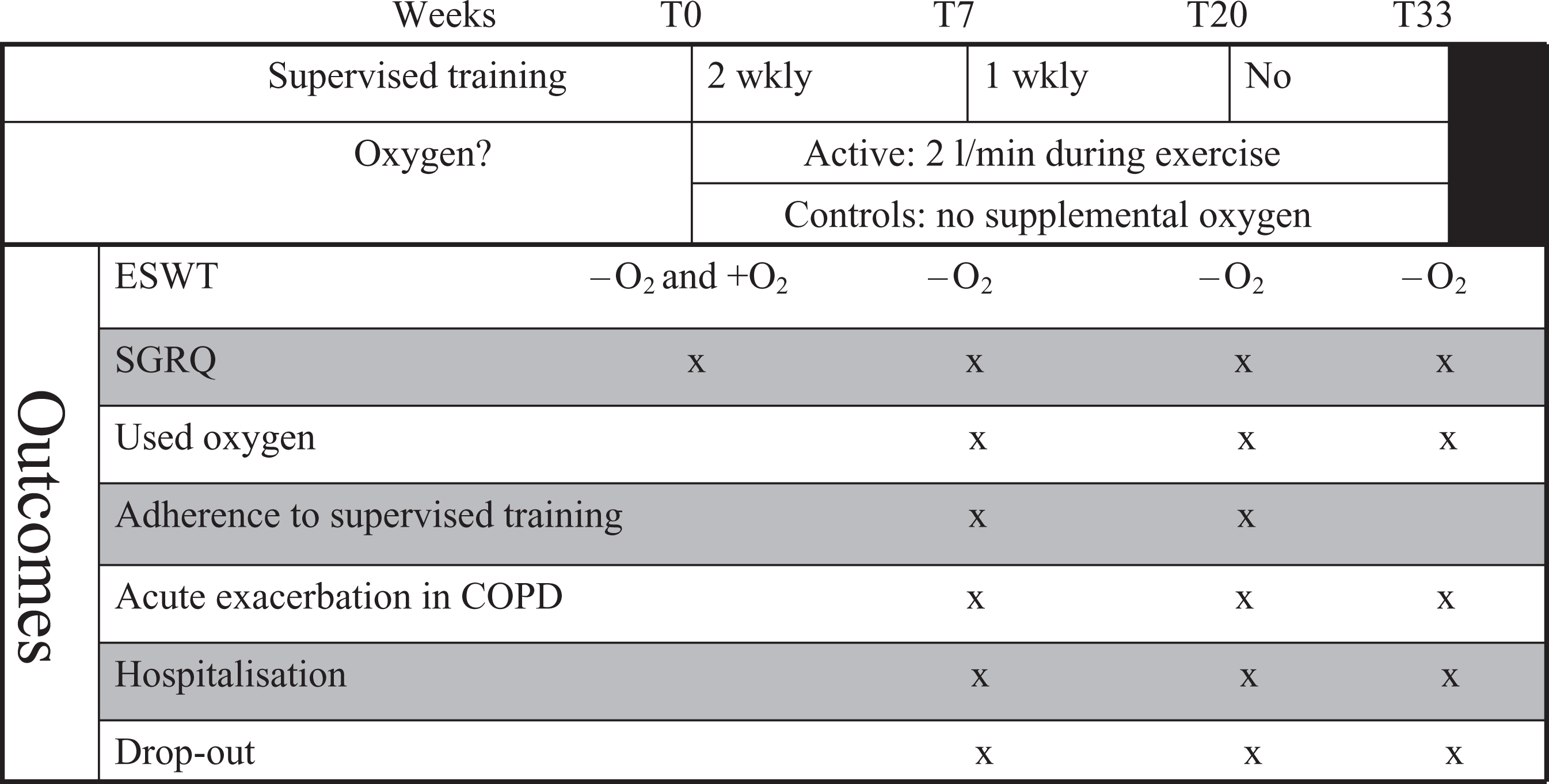
Study flow.
Portable oxygen device
Patients in the AO group received supplemental oxygen 2 L/min through a 2.3 kg portable oxygen concentrator (AirSep, FreeStyle; www.airsep.com/medical/freestyle.html) with an oxygen-conserving device. This device was able to provide a flow of 1–3 L/minute. In a prestudy test of the device, as several patients complained of the noise (44 dB) from the concentrator, when the highest flow was used, we decided to use 2 L/min (41 dB). Patients were asked to use the oxygen during supervised and unsupervised exercise (at least 30 min/day).
Outcomes
The primary outcome was ESWT, which was recorded at baseline, 7, 20, and 33 weeks (Figure 2). An incremental shuttle walk test (ISWT) was used to measure the maximal exercise performance in order to calculate the sub-maximal walking speed equating to 85% of predicted VO2 peak. After resting 30 min, patients were asked to walk as far as possible with the calculated sub-maximal speed (ESWT).
The acute effect of supplemental oxygen on ESWT was measured at baseline with at least 1 day between the two tests. The first test was on room air for both groups. The second test was on 2 L/min from the portable concentrator in the group randomised to oxygen and on room air in the control group without use of a sham concentrator.
Secondary effect parameters were St. George’s Respiratory Questionnaire (SGRQ), adherence with the supervised training and attendance to the evaluation visits, exacerbation in COPD requiring prednisolone and/or antibiotics, all hospital admissions, and deaths. Adherence with supervised training was calculated for the two periods (0–7 weeks and 7–20 weeks). Hours spent with oxygen were taken from the oxygen concentrator meter readings at every attendance.
The SGRQ is a disease-specific questionnaire that comprises three domains (symptoms, impact, and activity) and has been demonstrated to be valid, reproducible, and responsive in patients with COPD. 17
The Danish National Hospital Registry and The Danish National Registry of Deaths provided information on all hospital admissions, visits to emergency department, and vital status during the 33-week study period. Rates of exacerbations and hospital admissions were calculated for the periods: 0–7 weeks, 0–20 weeks, and 0–33 weeks for patients who attended the follow-up visit.
The locally appointed ethics committee has approved the research protocol, and informed consent has been obtained from subjects. The protocol is registered on ClinicalTrials.gov with protocol ID 2007-41-0569.
Sample size
Power calculations determined that 2 groups of 54 participants were required to provide a power of 0.95, at a level of 0.05, to detect a difference of 60 s (considered as clinical important difference (MID) in the primary outcome measure, ESWT. 18
Statistics
Data were analyzed with the statistical package (SPSS) version 13.0 SPSS Inc., Chicago, USA. The chi-square, two-sample t tests and Mann-Whitney U tests were used as appropriate to compare differences between groups, and Wilcoxon and one-sample t test were used to compare difference over time. A two-sided p value of <0.05 was considered significant.
Results
Only 45 of the 165 eligible patients with exertional desaturation wanted to participate in the study. They had severe airflow limitation (89% had FEV1 less than 50% of predicted value) and dyspnoea while walking (82% had at least MRC score 4) (Table 1). Compared to patients who declined participation in the study, those in the study group had higher MRC score, slightly lower saturation after ESWT, and were more often males (Table 1).
Characteristics of eligible patients at baseline according to whether they wanted to participate in the ambulatory oxygen study.

COPD: chronic obstructive pulmonary disease; FEV1: forced expiratory volume in 1 s; ISWT: incremental shuttle walk test; ESWT: endurance shuttle walk test; MRC: Medical Research Council.
Note: Continuous variables are presented as mean (SD) if nothing is stated.
a Hospital admissions due to exacerbation in COPD in patients who had been hospitalized.
In the study group, there were no statistical differences between patients on AO and controls at randomisation (Table 2).
Patient characteristics at baseline according to treatment groups.

AO: ambulatory oxygen; COPD: chronic obstructive pulmonary disease; FEV1: forced expiratory volume in 1 s; ISWT: incremental shuttle walk test; ESWT: endurance shuttle walk test; SGRQ; MRC: Medical Research Council: St. George’s Respiratory Questionnaire.
Note: Continuous variables are presented as mean (SD) if nothing is stated.
a Hospital admissions due to exacerbation in COPD in patients who had been hospitalized.
At baseline, supplemental oxygen, 2 L/min, improved ESWT to the same degree (by 19.2 s; p = 0.2) compared to supplementation of room air (19.9 s; p = 0.3).
Supplemental oxygen improved oxygen saturation during ESWT by 2.3% (95% CI: 1.2–3.5%; p < 0.001) to mean 86.4%, and only 50% of these patients had oxygen saturation <88% compared to 87% in the control group.
Drop-out rates from the rehabilitation program were high in both groups (Figure 3). One patient in each group died during the study period of 33 weeks. Two patients from the AO group withdraw due to lack of subjective effect of supplemental oxygen.

Flow chart of patients randomized to either ambulatory oxygen or control.
Adherence with the supervised training was high: patients participated in 88%% (AO: 89% versus controls: 87%, p = 0.52) of the supervised training sessions the first 7 weeks.
According to the dairy for the first 7 weeks, patients exercised on an average of 4.9 (range 1.5–7.0) days per week (5.0 vs. 4.9 for AO group and controls, respectively; p = 0.83).
According to the meter on the oxygen concentrator, patients spent an average of 7.9 h (0–54 h) per week on oxygen while they were in the study (Table 3). Of the 15 patients, 5 used oxygen less than half an hour on an average in the first 7 weeks, which was considered insufficient. These five patients declared that poor subjective effect of oxygen was the reason for the low usage of oxygen.
Spent hours on ambulatory oxygen in the study period (mean and SEM).

In the whole group, PR improved ESWT by 180 s (95% CI: 101–258 s) and SGRQ score by 2.6 units (95% CI: 0.1–5.1 units) after 7 weeks, and these gains remained at 33 weeks’ evaluation. There were no differences between the AO group and controls (Table 4).
Effect of pulmonary rehabilitation on ESWT, SGRQ, exacerbation in COPD and dropout rate in patients on AO and room air (controls), respectively.
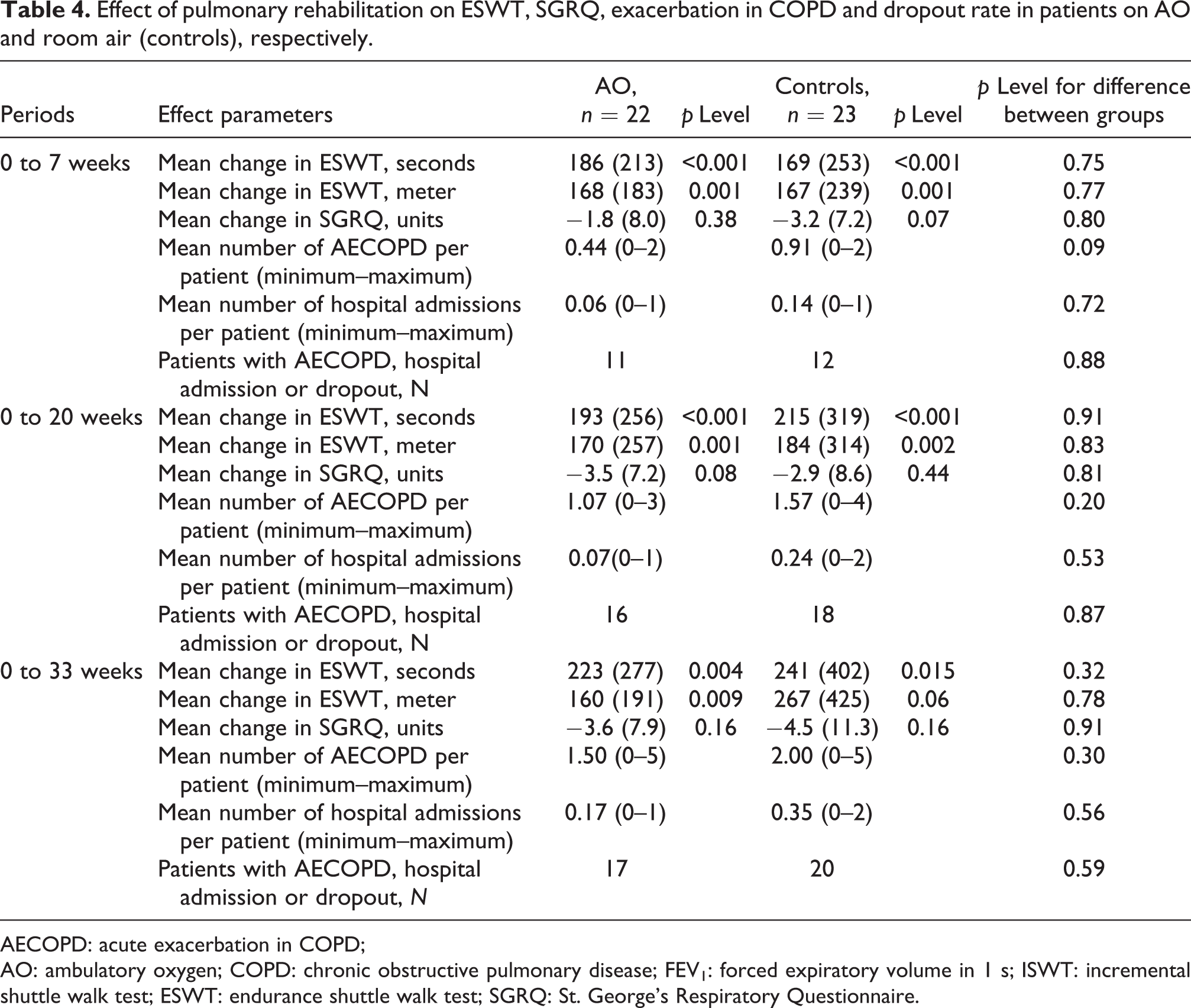
AECOPD: acute exacerbation in COPD; AO: ambulatory oxygen; COPD: chronic obstructive pulmonary disease; FEV1: forced expiratory volume in 1 s; ISWT: incremental shuttle walk test; ESWT: endurance shuttle walk test; SGRQ: St. George’s Respiratory Questionnaire.
There was a tendency towards higher rates of acute exacerbation in COPD and hospital admissions but a lower number of dropouts in the control group compared to the AO group (Table 4). The proportion of patients with acute exacerbation in COPD, hospital admission, or dropout was the same in the two groups.
A clinically relevant increase in ESWT of 60 s was seen in 8 of 15 patients in the AO group after 7 weeks. These “responders” had an acute response from supplemental oxygen of 63 s (−28 to 209 s) compared to 9 s (−18 to 41 seconds) in non-responders; p = 0.18.
Discussion
This is the first long-term study to evaluate the benefit of AO in combination with rehabilitation in COPD patients experiencing exertional desaturation without severe resting hypoxaemia. We found that exertional desaturation was common in non-hypoxaemic COPD patients referred to outpatient rehabilitation (44.4% of the patients), less than one third of the patients were interested in AO. Although AO reduced the degree of desaturation during exercise, it had no acute effect on ESWT or long-term effects on exercise tolerance, disease-specific health-related quality of life, and risk of exacerbation, hospitalization, or dropout.
Although this is the largest study of this kind, it is still small and underpowered to provide clear results. In general, it is very difficult to recruit patients for studies on AO in combination with PR, and previous studies have only included between 20 and 29 patients.10–13 None of these studies have reported the screening procedure and selection of patients, which is very important in order to generalize the findings.
Three studies on AO without scheduled exercise training showed similar high number of patients not interested in participation.19–21 Lacasse et al. studied AO in COPD patients on LTOT. Among 172 eligible patients, 124 declined enrolment in this 1-year trial. 21 In a 6-week trial by Nonoyama et al., 39 of 77 patients did not want to participate. 20 Recently, Moore et al. found 475 eligible patients for a 12-week trial, but 232 of these patients refused to participate. 19
In general, very few patients are prescribed AO in Denmark. Therefore, we expected that many patients would be interested to participate in this study in order to try AO for some months. We have no systematically registered reasons for declining enrolment in our study; but based on the interviews, it is our impression that many patients were embarrassed and disliked being seen using AO, or they found the provided transportable concentrator heavy to carry. 22 We consider that use of AO only at the hospital during supervised training is inferior to use of AO both at hospital and at home. A small economic compensation for one extra visit (test of acute effect of AO) would probably be accepted by the ethics committee and could possibly have improved the enrolment.
Patients in our AO group received supplemental oxygen through, AirSep Freestyle, which is one of the lightest portable oxygen unit available. The same oxygen unit was used in the Canadian study, where patients were asked to use supplemental oxygen during daily activities. 20 In this study, the hours spent on oxygen were only about one third of the numbers seen in our study. In the study by Moore et al., patients had oxygen cylinders weighing 4.2 kg, provided with a trolley/stroller delivering oxygen at a flow rate of 6 L/min. 19 In this study, the average time of oxygen usage was estimated to be approximately 3 h/week compared to about 7 h/week in our study. 19
Although AO significantly reduced desaturation during ESWT in our study, adequate correction of exertional desaturation was not achieved, and half of our patients remained hypoxaemic during exercise. This is in line with several studies,20,23,24 but in contrast to Garrod et al. who found that supplemental oxygen of 4 L/min improved the average oxygen saturation post-6MWT from 82% to 90%. 12 One could speculate that if our patients were provided a higher oxygen flow, they might have benefited from AO. However, the large Australian study using AO 6 L/min does not support this hypothesis. 19
Several studies have shown that supplemental oxygen acutely improves exercise capacity, 4 and that this effect is diminished, when patients have to carry the oxygen system themselves.25–27 Our patients had to carry the oxygen themselves, so this may at least partly explain the lack of acute effect of oxygen on ESWT in our study. There was a tendency towards a relationship between the acute effect of supplemental oxygen and the effect of rehabilitation combined with AO at 7 weeks’ evaluation on ESWT (tested on room air). Therefore, we recommend that future studies on AO exclude patients without an acute effect of supplemental oxygen.
Our patients had frequent exacerbation in COPD. In two cases (one in each group), exacerbation was the cause of dropout. About one third of our patients dropped out within the 6 months of study period, and this rate is higher than that observed in the Australian study of same length (4 of 143 patients). 19 Compared to our patients, the Australian patients had less severe COPD with higher FEV1 and only one third of them desaturated significantly during exercise. 19
In conclusion, this randomised trial found that AO at a flow rate of 2 L/min from a portable concentrator during PR seems not to provide additional benefit in terms of quality of life, exercise performance, risk of exacerbations, or hospitalisations in patients with COPD, without severe resting hypoxaemia, but experiencing exertional desaturation. Our findings do not support the widespread use of AO during PR in this group of patients, but larger, probably multicentre, studies on patients with acute effect of supplemental oxygen are needed.
Footnotes
Authors’ Note
All authors have read and approved the manuscript.
Funding
We have received a grant from The Danish Lung Association.