
Abstract
The effect of ambulatory oxygen use during pulmonary rehabilitation (PR) has not yet been clearly established, but many studies have shown benefit from oxygen acutely. Two small studies to date demonstrated no clear benefit when oxygen was used in patients who desaturated on exertion during a PR programme. One study showed the benefit of using oxygen during PR in patients who were normoxic at rest and desaturated to a minimum of 88% on exertion. We conducted a single-blind, randomised controlled trial comparing PR undertaken either with or without ambulatory oxygen, in those with demonstrable benefit from oxygen at baseline. Subjects from three PR services were recruited who, during baseline assessment, desaturated by more than 4% and to less than 90% on exertion, and walked 10% or more further with ambulatory oxygen on endurance shuttle walk test. Patients were randomised to either room air or oxygen via portable cylinder, titrated to optimise pulse oxygen saturation but up to a maximum flow rate of 6 L/min. All patients then completed a twice weekly, 6- to 7-week PR programme. Data were analysed as per protocol. Totally 51 patients completed the study. At the end of PR, both groups improved with PR, with patients in the oxygen group demonstrating a highly statistically significantly greater mean improvement in endurance walking distance than the controls, 490 m (95% confidence interval 228–750; p ≤ 0.001), as well as clinically, although not statistically, significant changes in quality of life. The use of ambulatory oxygen during a 6- to 7-week PR programme greatly improved endurance walking distance in patients who desaturated on exertion with a positive acute response to ambulatory oxygen at baseline.
Introduction
Pulmonary rehabilitation (PR) is recommended for all patients with chronic obstructive pulmonary disease (COPD) who are functionally disabled by breathlessness. 1 –3 However, many patients with COPD and normal resting oxygen saturation (SpO2) develop hypoxaemia on exertion, and whether or not to use ambulatory oxygen (O2) during PR has not yet been clearly established.
A Cochrane review concludes that O2 improves exercise tolerance and maximal exercise capacity when compared with placebo, 4 and it has been suggested there is now sufficient evidence for the acute effect of supplementary O2 that it is unnecessary to use a placebo during assessment. 4
Two small randomised controlled trials on the use of ambulatory O2 during PR in patients who were hypoxaemic on exertion showed no difference in distance walked demonstrated after a course of PR. 5,6 In a larger study, when given supplemental O2 during exercise, patients with COPD who desaturated to a minimum of 88% on exertion gained greater improvement in exercise capacity from a 7-week high-intensity exercise programme than those who were not given supplemental oxygen. 7
Current British guidance on domiciliary oxygen 8 recommends ambulatory O2 when an improvement in exercise tolerance is demonstrated at assessment following PR. Earlier guidelines 9 suggest a minimum of 10% improvement in exercise tolerance for the provision of ambulatory O2.
The aim of this prospective randomised controlled trial was to determine whether ambulatory O2 during PR provides additional benefit, compared with room air, for patients hypoxaemic only on exertion and who respond to supplemental oxygen at baseline. Additionally, we sought to determine whether the degree of acute response to ambulatory O2 predicted any additional benefit.
Methods
Patient demographics
Patients with COPD were recruited sequentially from three PR services in Surrey. These services provided PR in a mix of community and acute hospital sites. Eligible patients met the criteria for ambulatory oxygen, as set out below. Those with any existing form of home O2 were excluded.
Ethical approval was granted by the Surrey Research Ethics Committee, and all possible participants received written information regarding the study. All those entering the study gave written consent.
Demographic data (age, gender, height (cm), weight (kg), body mass index (BMI), and spirometry (performed with a micromedical microlab 3500 spirometer, Rochester, Kent, UK)) were recorded during the initial PR assessment.
Ambulatory oxygen assessment
Maximum exercise capacity and estimated peak oxygen uptake (VO2 peak) in room air were first established using the incremental shuttle walking test (ISWT) following one practice walk. 10 Eighty-five percent VO2 peak was then used to calculate the speed of the endurance shuttle walking test (ESWT). 11 O2 saturation was monitored continuously using a Nonin 9500 Onyx Finger Pulse Oximeter (Nonin Medical Inc, Plymouth, Minnesota, USA; SpO2).
Those patients who desaturated by more than 4% and to less than 90% 12 during ESWT in room air repeated this walk test with supplemental O2 via nasal cannulae, at 2, 4, and 6 L/min if necessary, until the SpO2 remained above 90% where possible. Higher flow rates via O2 mask were not used for pragmatic reasons, as beyond 6 L/min available portable systems were impractical; cylinders were able to last less than an hour and liquid O2 systems were unable to deliver more than 6 L/min. Appropriate rests (minimum 30 min) were allowed between walks. 11 Throughout all tests the cylinder was carried by another person to eliminate any counter effect of carrying the cylinder and walked behind the patient to avoid influencing speed or duration of the walk.
Patients were eligible if they demonstrated an improvement in ESWT of at least 10% with ambulatory O2.
Randomisation
Those who agreed to enter the study were randomised into two groups, room air (RA) group and oxygen (O2) groups, by random number tables and sealed envelopes.
Intervention
The PR programmes run in this study were cohort programmes with twice weekly sessions for 6–7 weeks, depending on the service, and followed current guidance. 1,3 All participants attended a PR programme that comprised strengthening and endurance exercise tailored to suit individual needs with aerobic exercise (walking) set at 85% estimated VO2 peak alongside an education programme. All were encouraged to exercise and walk at home on the days they were not attending class. The home exercise programme was that used in the class with the exception of specific equipment such as the static bike. Participants in both groups were exercised during PR at as high an intensity as possible that, when in PR, maintained SpO2 above the nadir SpO2 reached during baseline exercise testing.
Participants randomised to the O2 group were asked to use O2 at their prescribed flow rate for the exercise sessions for the duration of the PR programme both in the classes and at home, during all activities that induced dyspnoea but not at rest. Concordance to this advice outside the PR class was not monitored. The majority of participants received oxygen cylinders from the oxygen supplier, although a few were supplied with liquid oxygen. Mode of transport for the O2 cylinder during PR for those in the O2 group was decided on an individual basis and included carrying the cylinder in a carry bag, in a trolley, or in the basket of a three-wheeled walking frame, if clinically indicated. Those participants allocated to the RA group were asked to perform their exercise programme both in the class and at home without the addition of ambulatory oxygen.
Exercise tolerance at the end of PR for all participants was reassessed by FD, with blinding maintained by all participants wearing nasal cannulae with an oxygen cylinder attached, carried in a backpack by an assistant, which was switched off for the RA group. At the end of PR, exercise tolerance was reassessed by FD (blind to group allocation). It was not possible to blind participants to group allocation as sham O2 was not available.
Outcome measures
The endurance shuttle walk test
The ESWT was our primary outcome measure and is an externally paced, steady state walking test. The patient walks at a set pace based on the ISWT at 85% VO2 peak, 11 around a 10-m course at a speed dictated by an audio signal from a compact disc for as long as possible up to a maximum of 20 min. The ESWT has been shown to be more sensitive to change in exercise tolerance than the ISWT. 13
Other outcome measures were as follows and were carried out at baseline and immediately post PR. All questionnaires were self-administered with the exception of the Surrey Information on Function Tool (SIFT) which was administered by the PR clinician. The assessor remained blinded to all participant scores.
Hospital Anxiety and Depression scale
The Hospital Anxiety and Depression scale (HADS) is a self-administered questionnaire comprising seven questions relating to anxiety and seven to depression, each with a score between 0 and 3. 14 A total score for either domain of between 8 and 11 is clinically relevant and more than 11 suggests symptoms of clinical significance.
Self-reported Chronic Respiratory Questionnaire
The self-reported Chronic Respiratory Questionnaire (CRQ-SR) is a validated measure of health status for patients with chronic respiratory disease. 15,16 It comprises four domains: dyspnoea, emotion, fatigue, and mastery measured on a 7-point Likert scale. An increase in score indicates an improvement in health status, with a minimal clinically important difference (MCID) of 0.5 per domain. 12
Surrey Information on Function Tool
The SIFT questionnaire is a newly developed functional outcome measure that was validated as part of this study designed to measure function quickly and easily. The patient identifies three activities that are limited by their respiratory symptoms, scoring each for their perception of their ability to perform the activity (function), and their contentment with their performance, on a 10-point scale. The average of the three scores for both function and contentment is calculated, with an increase in score indicating an improvement. The tool has been shown to be valid and sensitive to change with PR. 17 Validation of this tool is being reported elsewhere.
Subjective perceptions of oxygen
In order to ascertain participants’ a priori beliefs about ambulatory O2, all participants were asked to complete a simple self-administered questionnaire prerandomisation (Appendix A). Those allocated to the O2 group also completed a second questionnaire post PR about post use beliefs and actual ambulatory O2 usage and, if it was not used as advised, reasons for this (Appendix A).
Statistical analysis
Statistical analysis and advice were provided by a statistician from the University of Surrey and the local strategic health authority (KC). A power calculation based on the ESWT identified the need for a sample size of 52 patients to achieve a difference of 80% between groups; significance was set at α = 0.05. A large difference was set due to the limited resources of the study and to ensure clinically and statistically significant differences were seen. Data were analysed using PASW Statistics Base (formerly SPSS) v18, from IBM. Data were normally distributed with descriptive data shown as mean and standard deviation (SD). Differences between groups are shown as a mean with 95% confidence intervals (95% CIs). Within group analysis was performed using a two-tailed paired t test and for between groups using a two-tailed t test. To determine the differences between more than two variables, a fixed one-way analysis of variance (ANOVA) was used. The relationship between the acute response to oxygen at baseline and change in walking distance post PR was determined using the Pearson product–moment correlation coefficient (r).
Results
Data collection took place between September 2007 and June 2009. Of the 66 eligible patients, 47 participants completed the study: 11 declined to participate, largely due to their own established opinion of O2; 8 patients did not want to use O2; 3 did not wish to risk being randomised to the room air group (Figure 1). Of the 55 consenting participants, 8 withdrew or were withdrawn from the study: only 1 person chose to withdraw as he wished to have O2 during PR; 7 dropped out of PR (3 due to an exacerbation of their condition, 1 due to other medical problems, and 3 for social reasons). The remaining person was withdrawn by the therapist responsible for that programme because he was not able to use O2 safely. Dropout was equal in both groups (Figure 1).

Study design and experimental protocol.
Baseline characteristics are shown in Table 1. The two groups are similar at the start of PR except for BMI which was higher in the RA group.
Baseline characteristics of participants who completed the study a
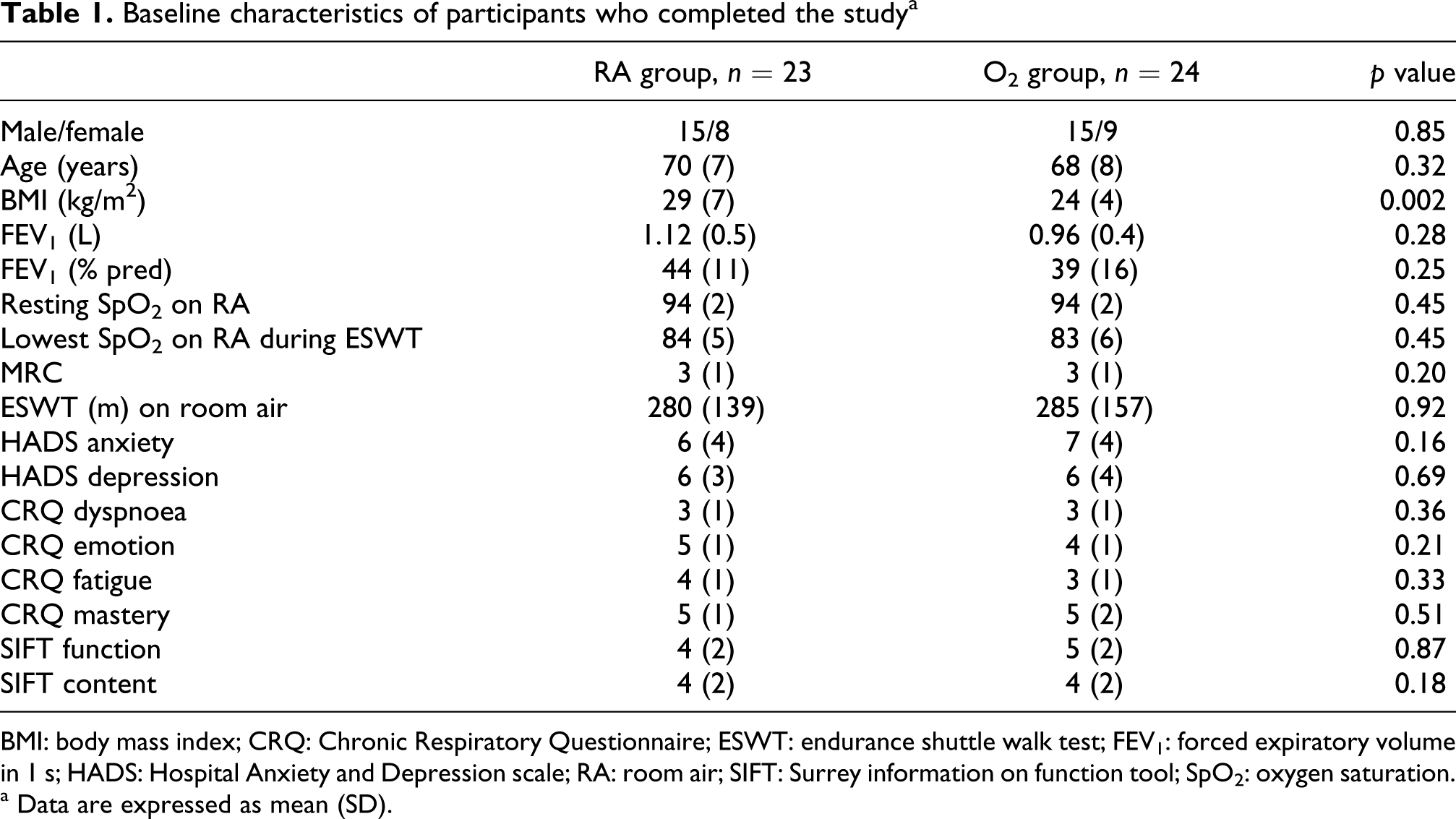
BMI: body mass index; CRQ: Chronic Respiratory Questionnaire; ESWT: endurance shuttle walk test; FEV1: forced expiratory volume in 1 s; HADS: Hospital Anxiety and Depression scale; RA: room air; SIFT: Surrey information on function tool; SpO2: oxygen saturation.
a Data are expressed as mean (SD).
Acute effect of O2 on ESWT at baseline
Compared with room air, the use of supplemental O2 significantly improved exercise tolerance at baseline for all patients, mean difference 275 m (95% CI 197–352 m). 49% of all oxygen responder participants required 4–6 L/min to maintain SpO2 above 90% during exertion and 51% required only 2 L/min.
Effect of ambulatory oxygen during PR on ESWT
Both groups showed a statistically significant improvement in exercise tolerance with PR, with an overall mean improvement of 516 (552) m (p ≤ 0.0001), baseline mean 283 (146) m and post PR 926 (534) m. There was no variation between venues (ANOVA p = 0.45). However, there was a clinically and statistically significant difference between groups in favour of the oxygen group (490 m, 95% CI 228–750, p ≤ 0.001; Table 2). A weak negative correlation (r = −0.19; p = 0.197) was identified between the magnitude of the acute response to ambulatory oxygen at baseline and change in ESWT post PR but did not reach the statistical significance.
Change in endurance shuttle walking test with PR

PR: pulmonary rehabilitation; RA: room air.
a Change in exercise tolerance is expressed in seconds (the recommended method to report change in ESWT), allowing for differences in severity of disability.
b Change in exercise tolerance is expressed in metres to demonstrate change in distance walked allowing for differences in severity of disability.
c Change in exercise tolerance is expressed in percentage change.
Change in secondary outcome measures
For the CRQ-SR dyspnoea domain, there was no statistical difference between the groups. The difference in change in the mastery domain between groups reached statistical significance (p = 0.006) in favour of the oxygen group but there was no difference in the emotion or fatigue domains. However, the change in the emotion, fatigue, and mastery domains met the MCID in the oxygen group but not in the RA group (Table 3). It should be noted that the difference between groups for these three domains also met the MCID, despite not all being statistically significant. There is no difference in HADS or SIFT scores between groups (Table 3).
Change in health status, emotion, and function

CRQ: Chronic Respiratory Questionnaire; HADS: Hospital Anxiety and Depression scale; MCID: minimal clinically important difference; RA: room air; SIFT: Surrey information on function tool.
a MCID for CRQ-SR (0.5 per domain) reached.
Patient perception of ambulatory oxygen
Following ambulatory oxygen assessment prerandomisation, almost 70% of the participants felt that oxygen would enable them to do more and almost half thought they would use ambulatory O2 during all activity even when out of the home environment, with 22% feeling they would use it during exercise only. Post PR, the O2 group still generally believed O2 to be beneficial, although 69% had used it only when doing their exercises. The main reasons for not taking the O2 out with them were that they found it awkward and difficult to carry, along with feeling embarrassed to use it (for further detail see Appendix A).
Do patients still desaturate post PR?
Of those in the RA group, all but one participant still desaturated significantly post PR with a mean (SD) nadir SpO2 of 82(5)%. Additionally, there was no difference in the extent of desaturation between pre- and post PR (p = 0.17).
Discussion
This study has shown that for patients with COPD, who are normoxic at rest but who desaturate on exertion by more than 4% and to less than 90% and who responded positively to oxygen at baseline, ambulatory oxygen significantly improves the effectiveness of PR on endurance exercise tolerance. Despite wide CIs, the lower CI still reflects a clinically important improvement. Although these results contrast with those found by Rooyakers et al. 6 and Garrod et al., 5 they do support the findings of Emtner et al. 7 However, their study included a different cohort of patients who desaturated to not less than 88% on exertion, whereas our cohort desaturated to an average of 83% (with a range 69–89%). This is the first study to solely include oxygen-naive patients who desaturate significantly on exertion and not some patients already on long-term oxygen therapy (LTOT) or requiring LTOT assessment.
Our results make it clear that participants who desaturated and responded to oxygen, but who undertook PR without oxygen, gained less benefit from PR than those who used ambulatory oxygen. This may be due to undertraining, since even at the start of PR the oxygen group were, with supplemental oxygen, able to walk 289 (229) m further than the room air group. It is worthy of note, too, that participants exercising in room air did not desaturate any less at the end of PR than at the start. We did not measure SpO2 at isotime and this is a potential limitation of these results.
A significant difference between the two groups in the mastery domain of the CRQ-SR was noted. This could suggest that those who used oxygen on exertion felt more in control of their condition compared to those who did not use oxygen. This is an important finding as self-efficacy improves self-management and may promote longer term behaviour change. 18 The difference in the dyspnoea domain between groups is interesting and does not seem to be in keeping with our other results, and may be a feature of power. However, participants in the oxygen group despite being more breathless could do significantly more than those in the air group.
Even when the acute effect of oxygen at baseline is removed from our results, there is still an 81% difference in distance walked between groups. This does not meet statistical significance probably due to the wide CIs seen. Such a large difference, however, is likely to be clinically significant and should not be discounted, since walking distance has been shown to directly affect the outcome of COPD. 19 This study was carried out in a clinical service over a finite period and it was not possible to extend the study duration. It was therefore not feasible to study sufficient numbers so that smaller differences between groups could have been identified and is a limitation of our study. Lack of an intention to treat analysis will be considered a limitation of this study. However, the decision to use an efficacy analysis was based on the need to determine whether, in clinical practice, if a patient who meets these study criteria will gain benefit from using ambulatory oxygen during PR.
In line with the other studies, 5,6 there appeared to be greater improvement in health status in the oxygen group which also did not meet statistical significance. It is conceivable that significant improvements in quality of life, emotion, or function may have been seen with a greater number of participants.
Another limitation of this study may have been the absence of a true placebo group but as described earlier there is contradictory evidence for the placebo effect. It is now felt that within a clinical service, use of placebo or sham oxygen is not necessary when assessing for ambulatory oxygen but whether a placebo could affect outcome of training is unknown. As stated previously, we attempted to obtain sham oxygen but this was not possible due to limited study resources but should be considered in future studies. End assessments were completed in the group they were allocated and therefore the groups were assessed under different conditions and is a criticism of the methodology.
It was not known whether BMI influences the outcome of PR, however recent data indicated that it makes no difference. 20
This study primarily examined the effect of ambulatory oxygen within PR and compliance with ambulatory oxygen use at home was not objectively measured. A recent article found that patients were more likely to go out without taking a portable cylinder and those with cylinders went out less frequently than those without. 21 In addition, another study reported that oxygen improved the quality of life in patients with COPD in day-to-day life, but at the end of the study 41% did not wish to continue with oxygen as they felt the benefit did not outweigh the inconvenience. 22 It would be interesting to determine whether the increased availability of liquid O2 will have an effect on this since it is more portable and lasts longer, enabling people requiring O2 to stay out for longer periods of time. Few of our subjects used liquid oxygen as it was not readily available during the study period. However, despite patients not using it a great deal beyond the formal exercises, it helped them achieve a major enhancement to the change in exercise capacity with PR.
The results of this study will help inform future recommendations for ambulatory oxygen, since our data show that the majority of patients in the air group still desaturated significantly post PR despite a good increase in exercise tolerance. The oxygen group was not retested on air post PR to see whether this differed between groups.
Further research is needed on the long-term effect and use of ambulatory oxygen in this select patient group to see whether patients continue to use it and whether the increased benefits gained are better maintained.
Conclusion
This randomised controlled trial strongly supports the use of ambulatory oxygen in PR in selected patients with COPD who desaturated at baseline by more than 4% and to below 90%, and who respond favourably to oxygen with an improvement in exercise endurance of at least 10%.
Footnotes
Appendix A
Acknowledgements
We are very grateful to the service managers and clinical leads in Surrey Community Health and the Royal Surrey County Hospital for their support of the project and to David Lovell for performing the power calculation. We would like to thank all the PR staff whose patients were study participants; Helen Best, Laura Cornish, Annelies Klinker, Caroline Marsden, Pam Marriner, Abby Smith, Ruth Thompson, Emma Ward, Chris Grimley and Laura Webb, and our colleagues in the Respiratory Care Team for their moral and practical support.
This study was partially funded (£15 000) by The British Lung Foundation through the Trevor Clay memorial fund.