
Abstract
Fatigue is a debilitating symptom in patients with cystic fibrosis (CF). Although fatigue is commonly reported in these patients, an effective treatment for this symptom has not been found. The factors associated with fatigue in CF have not been investigated. We conducted a prospective, case–control study in adult patients with CF. All the patients were chronically infected with Pseudomonas aeruginosa and were enrolled in the study during disease stability. A gender and age-matched control group was also recruited. Subjective assessment included three questionnaires: the Chalder fatigue questionnaire, St Mary’s Hospital sleep questionnaire (SQ), and the scaled general health and Hillier questionnaire (GHQ). For patients with CF, spirometry, body mass index (BMI), haemoglobin level, C-reactive protein, and the burden of pulmonary exacerbations (PExs) were assessed. The control group completed all the three questionnaires, and their BMI was measured. A total of 78 participants were enrolled in the study (44 patients with CF and 34 control). Female patients with CF received antibiotics for more days than male patients with CF. The fatigue score did not differ between female and male participants in either the patients with CF or the control group; however, the fatigue score was greater for both the sexes in the patients with CF compared with the control group: p = 0.038 for female and p = 0.048 for male. The scores for the SQ and the GHQ did not differ between the two study groups. The fatigue score correlated with the total score for SQ (p < 0.0001) in patients with CF, but not in control participants. In patients with CF and the individuals in the control group, a close correlation was found between the fatigue score and the GHQ domain-specific scores and with the total score; p < 0.0001 for patients with CF and p = 0.001 for control. No correlations were found between the fatigue score and any of the objective parameters studied.
Introduction
The number of adult cystic fibrosis (CF) patients are increasing due to improvement of care during childhood that has led to increased longevity. Adult patients with CF experience several somatic and psychological symptoms. Fatigue is one of the most common symptoms described by the patients with CF, for which no specific treatment has been developed.
Fatigue was found to be a common symptom that was reported in 20% of adults in the general population. 3 It was also shown to increase in patients with other respiratory disorders. It was found to be common in patients with chronic obstructive pulmonary disease (COPD), particularly in those with severe lung disease and greater impairment of exercise tolerance. 4 Furthermore, in a cohort of patients with bronchiectasis, fatigue was reported in 74% of the patients. 5
We previously noted that when patients scored their symptoms using an electronic diary on a daily basis for 180 days, fatigue was reported on 73% of days during disease stability and on 98% of days during exacerbations. 6 Similar results were found in a prospective, longitudinal study of 303 adult patients with CF, wherein the prevalence of fatigue, along with cough and breathlessness, was reported by 77% of the total patients. 7 As the patients’ health progressively declines, fatigue increases the disease burden on patients and on their carers. In one observation, caregivers reported fatigue to be present in 96% of patients with CF, who are in their last week of life with fatigue being the second most distressing symptom after breathlessness. 8
Fatigue is often difficult to describe. To some patients, it represents the inability to perform day-to-day activities. To others, it is a combination of tiredness, decreased muscle activity, and lower mood. Therefore, several terms are often used to describe fatigue, such as lack of energy, tiredness, and muscle weakness. The causes for fatigue in patients with CF have not been fully understood, but may include chronic pulmonary and systemic inflammation, sleep disturbances, impaired neurocognitive function, and low mood. 9–11
This study aimed at formally and prospectively examining factors associated with fatigue in a cohort of adult patients with CF during disease stability. We hypothesised that the factors associated with fatigue in adult patients with CF involved a combination of objective and subjective factors. The objective factors included female gender, number of days the antibiotics for pulmonary exacerbations (PExs) was prescribed during the study year, increased pulmonary disease severity, low body mass index (BMI), and raised circulatory inflammatory markers (C-reactive protein (CRP)). The subjective factors investigated were perception of impaired sleep quality, overall perception of low general health, and increased depression.
Patients and methods
General study design
This was a prospective, case–control, cross-sectional study. The research was approved by the South Bristol Research Ethics Committee. The inclusion criteria specified that the study participants were consenting patients with CF aged ≥18 years with chronic infection of Pseudomonas aeruginosa who had not experienced any PExs requiring either oral or intravenous (IV) antibiotics in the past 4 weeks. The exclusion criteria included patients who had organ transplantation, pregnancy, and patients on long-term corticosteroids (mainly administered for concomitant asthma or allergic bronchopulmonary aspergillosis).
The control group included people aged 18–40 years with no known chronic disease and who were not on any long-term medications. They were mainly medical students and staff members of the respiratory department. The participants were included if they had not experienced any viral or bacterial infection in the past 4 weeks. Female participants who were receiving oral contraceptive agents were not excluded from the study (both in the control and CF groups). Most invited control subjects agreed to participate in the study.
The three questionnaires
After obtaining informed consent, CF patients and individuals in the control group were asked to complete three questionnaires: the fatigue questionnaire described by Chalder et al., 12 St Mary’s Hospital sleep questionnaire (SQ) that examined the participants’ perception of their quality of sleep, 13 and the scaled general health and Hillier questionnaire (GHQ) that was designed to measure the participants’ perception of their health status. 14 The three questionnaires were selected by one of the authors (K.B.) with the assistance of The Academic Unit of Psychology, Medical Research Council and Bristol University, Bristol, UK.
The three questionnaires were self-administered, but an operator, a research scientist, or a doctor for CF was available to explain any aspect that was not clear to the study participants. The fatigue questionnaire was chosen as it was described previously and applied to patients with chronic fatigue syndrome – a group with similar age as that of the CF population. The questionnaire was developed and validated by Chalder et al. 12 It includes 14 items, each of which is scored at four levels: not at all (0), no more than usual (1), rather more than usual (2), and more than usual (3). Therefore, the scoring system was a 56-point scale, and the scores ranged from 0 to 42, with a higher score representing a greater perception of fatigue.
The SQ is a seven-stem questionnaire describing the patient’s perception of his/her quality of sleep during an average night. 13 The items in this questionnaire did not overlap with the items of the other two questionnaires. The number of options for each stem varied from two options (yes or no, one stem), four options (one stem), five options (one stem), six options (two stems), and nine options (two stems). Therefore, the scale consisted of 41 points, with a greater score representing a lower quality of sleep as perceived by the patient. Only the scores from these questions were included in the analyses. The questionnaire also contained questions that asked the participants to numerically estimate the average time taken to settle down for the night, the time before falling asleep, the time of wake-up in the morning, and the time of getting out of bed in the morning. Other items sought to assess the duration of sleep during the night and that during the day. None of these numerical items were included in the estimation of the total score. The questionnaire did not query the consequences of sleep the following day in the form of daytime hypersomnolence.
The GHQ was developed by Goldberg and Hillier. 14 It contains four domains, each of which comprises seven stems with the answers for each ranging from: ‘not at all’ to ‘more than usual’ using similar wording, order, and degree of marks to the fatigue scale described above. The first domain addresses somatic symptoms, whereas the questions in the second domain are on anxiety and insomnia. The stems in the third domain include social functions, such as being able to carry out tasks and make decisions. The fourth domain contains seven items, each of which concerns depression. Thus, this questionnaire had an 84-point scale, with a greater score indicating a lower perception of general health.
At the time of publication of these questionnaires, the concept of minimal clinically important difference (MCID) 15 was not yet usually used in the literature, and therefore, none of the questionnaires had an identifiable MCID.
Other assessments
In addition to the subjective questionnaires, several objective assessments were used to examine factors associated with increased fatigue. These included severity of lung disease, circulatory inflammatory markers, BMI, and the frequency of exacerbations. These parameters were chosen because we previously found them to correlate with reduced forced expiratory volume in 1 second (FEV1) and increased need for IV antibiotics. 16,17 Haemoglobin level was added due to the relationship between fatigue and anaemia.
At enrolment, a venous sample was withdrawn from the patients with CF and analysed for the levels of haemoglobin and the high-sensitive CRP. Those analysing the samples were blinded to the study or to the samples whether they were obtained from the patients with CF or controls. All the patients with CF underwent spirometry, and their BMIs were calculated. The CF exacerbations burden was assessed by calculating the number of days the patients received antibiotics (both oral and IV) for PExs during the year of the study.
All the spirometry measurements were performed according to the recommendations of the British Thoracic Society/Association of Respiratory Technicians and Physiologists guidelines and by qualified and experienced lung physiologists, who were unaware of the purpose of the study. 18 FEV1 was the parameter used for analysis. The percentage of predicted values using the adult reference obtained by the European Community of Steel and Coal workers was calculated and used for the analysis. 19
For the control group, information on age, gender, and BMI were obtained. The participants completed the three questionnaires. Blood tests and spirometry were not performed as the local ethics committee objected to this.
Statistical analysis
Statistical analysis was performed with the assistance of the Biomedical Statistics Department staff at our institution. The GraphPad Prism 4 statistics and graphing package was used for the analysis. Standard analyses were applied.
First, the data were inspected for normality of distribution. As the scores of the three questionnaires were not normally distributed, nonparametric methods using the Mann–Whitney U test were used to compare the two study groups. For the same reason, all the correlations between the fatigue score and the other study parameters were made using Spearman’s correlation coefficient. For age, BMI, FEV1, and CRP, comparisons were made using the two-tailed Student’s t–test.
Finally, multivariate methods using multiple regression analysis were applied to examine the contribution of candidate factors to the fatigue score. The fatigue score was the dependent factor, and the candidate parameters were the independent factors. Differences were considered significant if the two-tailed p values were <0.05.
Results
A total of 78 participants, 44 patients with CF and 34 control subjects, were enrolled in the study. Table 1 shows their demographic data. The two groups were matched for age. The control group had more female participants, and their BMI was greater than that of the patients with CF.
Demographic data

CF: cystic fibrosis; BMI: body mass index; M: male; F: female.
a p = 0.008.
Table 2 provides a comparison of the male and female study subjects. The number of days the antibiotics for PExs was prescribed in the study year was greater for female patients compared with male patients with CF. However, no differences were observed in BMI or in pulmonary disease severity as assessed by FEV1 between the male and female patients with CF.
Parameters of the female and male participants in the two study groups

SQ: sleep questionnaire; GHQ: general health and Hillier questionnaire; NA: not assessed; CF: cystic fibrosis; IV: intravenous; BMI: body mass index; FEV1: forced expiratory volume in 1second.
a p = 0.034 for female patients with CF compared with male patients with CF.
b p = 0.048 for female patients with CF compared with male patients with CF.
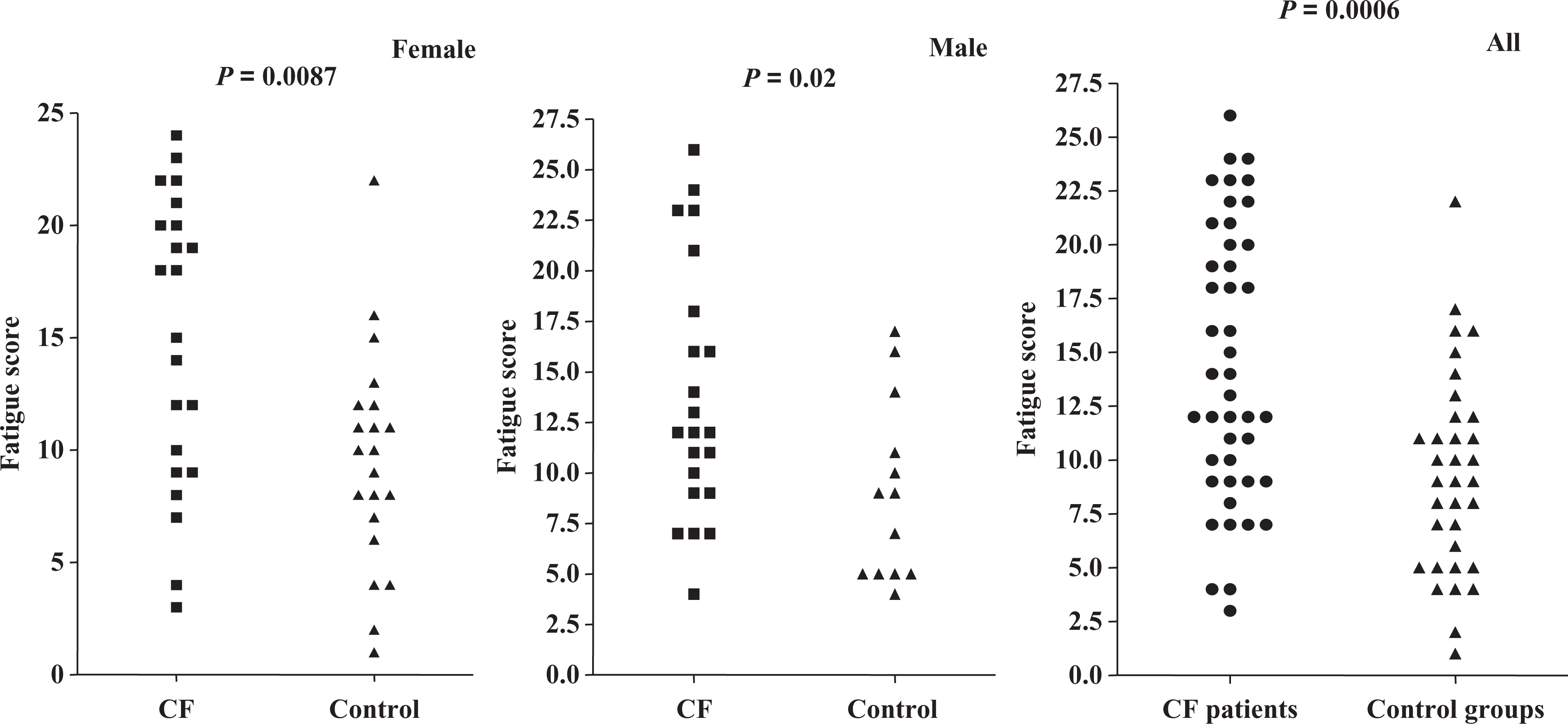
c p = 0.0087 for female patients with CF compared with female controls, p = 0.02 for male patients with CF compared with male control (see also Figure 1).
d p = 0.015 for female CF compared with male control patients.
The fatigue score for all of the patients with CF was greater than that of all of the control participants (Figure 1). On further comparison of gender differences, we found that the fatigue scores of the male and female patients with CF were greater than those of the male and female control subjects, respectively (Table 2 and Figure 1). However, no differences were found between the fatigue scores in female and male patients for either the patients with CF or the control group.
Fatigue scores of the two study groups for males, females, and all patients.
The SQ and GHQ scores did not differ significantly for each gender between the CF and control groups. GHQ was greater in patients with CF compared with controls for all groups but only reached a statistical significance when female patients with CF were compared with male control participants, p = 0.015 (Table 2 and Figure 2).

SQ and GHQ scores for the two study groups. For gender differences, refer Table 2. SQ: sleep questionnaire; GHQ: general health questionnaire.
No correlation was observed between the fatigue score and any of the subjective parameters (Table 3). The fatigue score moderately correlated with the SQ score (Figure 3(a)) in the patients with CF, but not in the control subjects (Table 3). In the patients with CF, there was a moderate correlation between the fatigue score and the total score of the GHQ (Figure 3(b)) as well as with the scores of each domain (Table 4). Similar findings were observed in the control group, but the degree of correlations were weaker than those in the CF group, with the exception of the depression domain, which did not correlate with the fatigue score (Table 4).

Relationship between the fatigue score and the SQ score (a) and the GHQ score (b) in patients with CF. CF: cystic fibrosis; SQ: sleep questionnaire; GHQ: general health questionnaire.
Spearman’s correlation coefficient between the fatigue score and other measurements in patients with CF and control participants

CF: cystic fibrosis; FEV1: forced expiratory volume in 1second; NA: not assessed; IV: intravenous; BMI: body mass index.
Spearman’s correlation coefficient between the fatigue score and the score of each GHQ domain in patients with CF and control participants
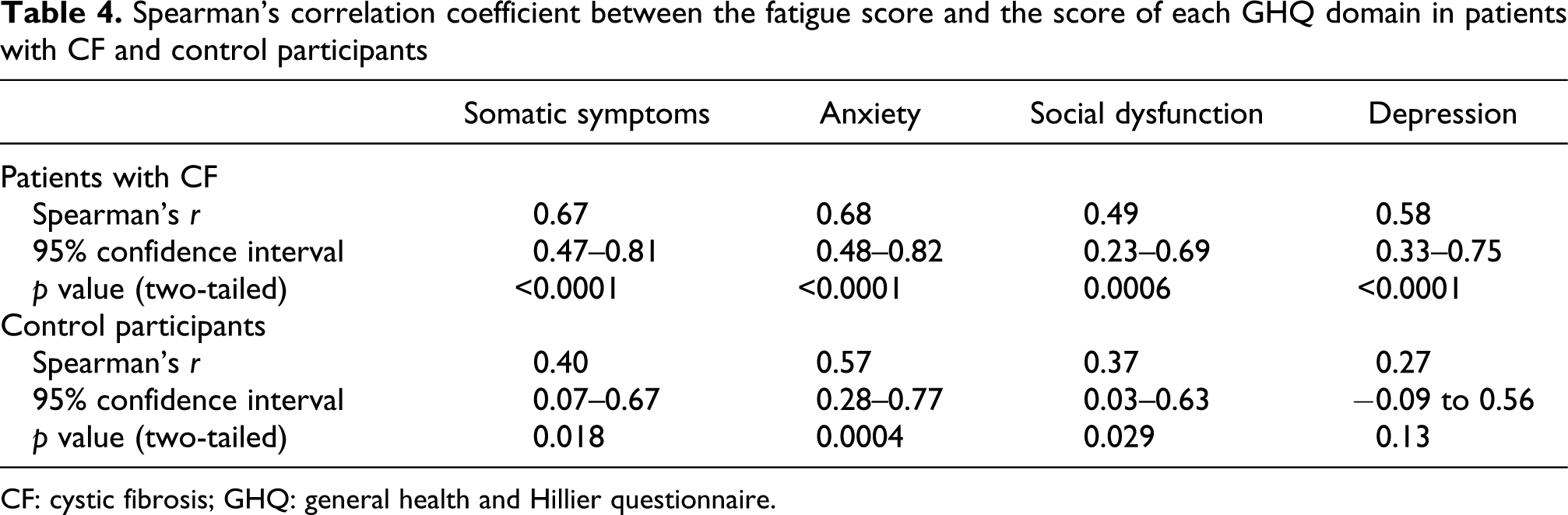
CF: cystic fibrosis; GHQ: general health and Hillier questionnaire.
Despite disease stability, 12 (28.6%) of 42 patients with CF exhibited increase in CRP values, which is greater than the levels that is considered abnormal at our institution (i.e. 10 mg/L). The fatigue score did not differ in the patients with CF with raised CRP levels (median fatigue score, 13 (range, 3–24)) compared with patients with CF exhibiting normal CRP levels (median fatigue score, 14 (range, 4–26)).
Multiple regression analysis was performed with the fatigue score as the dependent factor and the scores for each of the two questionnaires as the independent factors. The analysis confirmed that the fatigue score correlated with the SQ and GHQ scores in patients with CF and with the GHQ score, but not the SQ score, in control subjects (Table 5).
Multiple regression analysis for patients with CF and control participantsa

CF: cystic fibrosis; SQ: sleep questionnaire; GHQ: general health and Hillier questionnaire.
aThe fatigue score is the dependant factor, and the total score of each of the two other questionnaires used in this study are the independent factors.
Discussion
To our knowledge, this is the first study to specifically examine factors associated with fatigue in adult patients with CF. Therefore, we chose objective and subjective components that we hypothesised may contribute to the perception of fatigue.
The choice of participants and parameters
We specified the inclusion criteria of patients with chronic P. aeruginosa infection (more than two positive sputum cultures per year) in order to decrease the variability among the CF study participants. This group also constituted 78% of all the adult patients in our unit.
Several scoring systems were chosen for this study. As mentioned previously, the fatigue score was selected because it was validated in patients aged 18–45 years, a similar age range as that of our patients with CF. 12 The perception of quality of sleep was semiquantified by the SQ 13 in order to investigate the contribution of sleep quality to daytime fatigue. This particular questionnaire was chosen because it did not include any items that might overlap with those in the fatigue questionnaire. To account for anxiety and depression, as well as the perception of general well-being, we chose the validated and widely used GHQ. 14 The items of this questionnaire also did not overlap with those of the fatigue questionnaire or the SQ.
The choice of objective parameters was based on the findings of two previous studies, wherein adverse outcomes in adult patients with CF were observed in female patients, in patients with worse FEV1 and frequent PExs, and in patients with low BMI. 16,17 To these, we added haemoglobin and CRP to account for any residual systemic inflammation during disease stability. We did not include CF-related diabetes because patients with this complication would have lower FEV1 16 and would have spent an increased number of days the antibiotics was prescribed, 17 both of which were already included as risk factors for fatigue.
Key findings of the study
As expected, female patients with CF were generally sicker and tended to receive more courses of antibiotics than male patients. This observation is consistent with registry data1,2 and data reported in other studies. 16,17 Despite this, the fatigue score was not significantly different between the two gender groups in either the patients with CF or the control participants. Similarly, and despite the high level of CRP during disease stability in nearly one-quarter of the patients with CF, the fatigue score was not increased in patients with higher CRP levels. These observations and the lack of correlation of the fatigue score with all other objective factors were remarkable and contrary to our original hypothesis. The previously noted contrast between perception of symptoms and changes in biomarkers in CF was one reason for Goss and Quittner 20 advocating the introduction of validated patient-reported outcome in clinical trials.
The strong correlation between the fatigue score and the SQ score in patients with CF, but not in the control group participants, was notable. This may have been because the factors affecting the quality of sleep in both the study groups were different. In patients with CF, the disturbance of sleep architecture has been reported 21 and was found to be due to the symptoms of CF, including cough, sputum production, breathlessness, and pain. 21–24 In addition, drugs such as inhaled short-acting and long-acting β2 agonists and theophyllines would impair the quality of sleep. Therefore, it is plausible that these factors per se as well as impairment of sleep might have contributed to an increase in fatigue. In case of the control participants of this age group, the impairment in the quality of sleep score may have been due to life style or psychological factors.
The close correlation of the fatigue score with the domain-specific and total GHQ scores suggested that the subjective aspects of patient’s with CF somatic and psychological symptoms would be the main causes of the perception of increased fatigue.
Limitations of the study and suggestions for future research
The study has limitations. The number of participants is modest and the sample size is a convenience sample based on the availability of participants. This may account for the nonsignificant statistical difference for GHQ between CF and the control group who has had lower scores.
Although the control group were age-matched with patients with CF, they were all in employment and probably have greater educational attainments compared with the patients with CF. Despite these shortcomings, one key message from this research is that the management of fatigue in patients with CF may require additional to conventional management. These measures involve focusing on methods that are likely to improve quality of sleep, anxiety, and depression, as well as increasing perception of self-worth among the patients.
Very few studies have attempted to manage fatigue as a symptom, none of which included patients with CF. In a group of patients with chronic fatigue syndrome, a small dose of hydrocortisone (5 or 10 mg) was found to reduce the fatigue score compared with placebo. In some patients, the score decreased to a level similar to that observed in the normal population. 25
Another prospective randomised study of 60 patients with COPD compared a 10-day course of breathing exercises (i.e. pursued lip respiration and effective coughing) performed four times daily with usual care. The study reported a significant improvement of the fatigue score in the breathing exercise group compared with the usual care group. 26
Adding short courses of oral corticosteroids for patients with CF as the case in chronic fatigue syndrome would require a formal investigation given the difference in disease process and the susceptibility of this group to osteoporosis and diabetes mellitus.
Due to the great impact of fatigue as a symptom on patients, this study could form a basis of future work particularly in evaluating pharmacological and nonpharmacological management methods on fatigue as a unique symptom or in conjunction with other patients-reported outcome.
Footnotes
Funding
This research was supported by an unrestricted grant from the David Telling Charitable Trust, Bristol.