
Abstract
Patient’s attitudes and illness beliefs have shown to be of great importance in chronic obstructive pulmonary disease (COPD). As former qualitative research has mainly focused on patients with end-stage COPD, who are recruited within hospital or pulmonary rehabilitation settings, and excluding patients with disabling comorbidities, this study specifically aims to explore the perspectives of patients with COPD and comorbidities in primary care. This study was designed as a qualitative, explorative study using open patient interviews. The study was conducted at three primary care practices, East Flanders, Belgium. A total number of seven patients, diagnosed with COPD and given a minimum score of 2 on the Charlson Comorbidity Index were included. In-depth interviews were recorded and transcribed verbatim. Thematic analysis was deductive using NVivo software. Researchers’ triangulation was performed. Participants show high adaptation capabilities and report quite positively about their functional status, with an emphasis on social participation and partnership. Knowledge of the causes and consequences of COPD appears rather limited, and participants predominantly show an external locus of control in relation to the reported factors influencing the disease and strategies for self-management. Patients with COPD with comorbidity integrate their illness and symptoms into their lives. However, a lack of knowledge and education may leave them more anxious and more dependent on health care than necessary. Our results indicate that health care workers should adopt a positive approach toward patient’s functioning and empower and inform their patients. We believe that chronic care for patients with COPD should provide personalized rehabilitation taking into account individual patient characteristics and self-management and coping attitudes. We believe that there is a generic core to be identified, which can tackle both COPD and comorbidities. Further research is mandatory to develop these generic programs focusing on patients with complicated needs. Primary care can provide the setting for exploration.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is an important cause of lost life years and its importance is still growing. By 2030, COPD is expected to be the fourth leading cause of mortality, morbidity and disability worldwide. To assess and monitor the impact of the disease and of interventions that tackle it, a relevant measurement of the disease outcomes is of great importance. In the last decades, the use of purely biomedical outcome measures such as pulmonary function results and 6-minute walking tests has gradually shifted toward patient reported outcome (PRO) measures such as functional status and quality of life. 1 In contrast to pulmonary function results, specific quality of life scales focusing on symptoms, activity impacts and total quality of life (Saint Georges Respiratory Questionnaire 2 and COPD Assessment Test (CAT)) 3 have been shown to correlate with disease severity, use of resources, rehospitalization rates and even mortality. 4,5 In this context, patient’s attitudes and illness beliefs 6 play an important role. They are associated with functional status and disability, psychological outcomes and quality of life, and they influence the way patients deal with COPD exacerbations and determine the length and frequency of hospitalizations. 7 –11
However a systematic literature search on COPD and qualitative research (revealing 97 articles) indicated that most qualitative inquiries in patients with COPD have focused on end stage COPD without comorbidity recruiting participants outside of primary care; However, the majority of patients with COPD is at home 12 and has more than one illness. 13 36 articles had a single focus on very severe COPD, end of life, respiratory failure, lung transplantation or oxygen dependence and 31 articles merely recruited in hospitals or pulmonary rehabilitation settings. Only five articles mentioned recruitment in primary care or at population level in their abstract and only one abstract explicitly mentioned the issue of comorbidity in COPD. As former qualitative research has mainly focused on patients with end-stage COPD, recruited within hospital or pulmonary rehabilitation settings, and excluded patients with disabling comorbidities, this study specifically aimed to explore the perspectives of patients with COPD and comorbidities in primary care.
Methods
Study design
To explore perspectives of patients with COPD and comorbidities in primary care, we adopted a qualitative approach using open patient interviews. An inductive analysis revealed core themes. Consequently, the defined themes were linked to previous findings revealed by means of a systematic literature search for qualitative inquiries in patients with COPD. This study was approved by the Ethics Committee of the Ghent University Hospital.
Setting and sampling
General practitioners (GPs) were asked to include patients with COPD and comorbidity. The diagnosis of COPD had to be confirmed by spirometry. Comorbidity was defined by a Charlson Comorbidity Index 14 score of at least 2. A condition was considered relevant when it was the reason for at least one medical encounter or referral within the previous year. After written informed consent, collected by the GP, the respondents were contacted by an interviewer. In a single wave, four men and four women having three to eight chronic diseases (including COPD) were selected from three primary care settings in the Province of East Flanders, Belgium: one single handed practice (two patients), one group practice (three patients) and one community health center (three patients) (Table 1). All invited participants agreed to participate and were interviewed at home between November 2008 and March 2009. One female patient dropped out because of family circumstances.
Patient characteristics
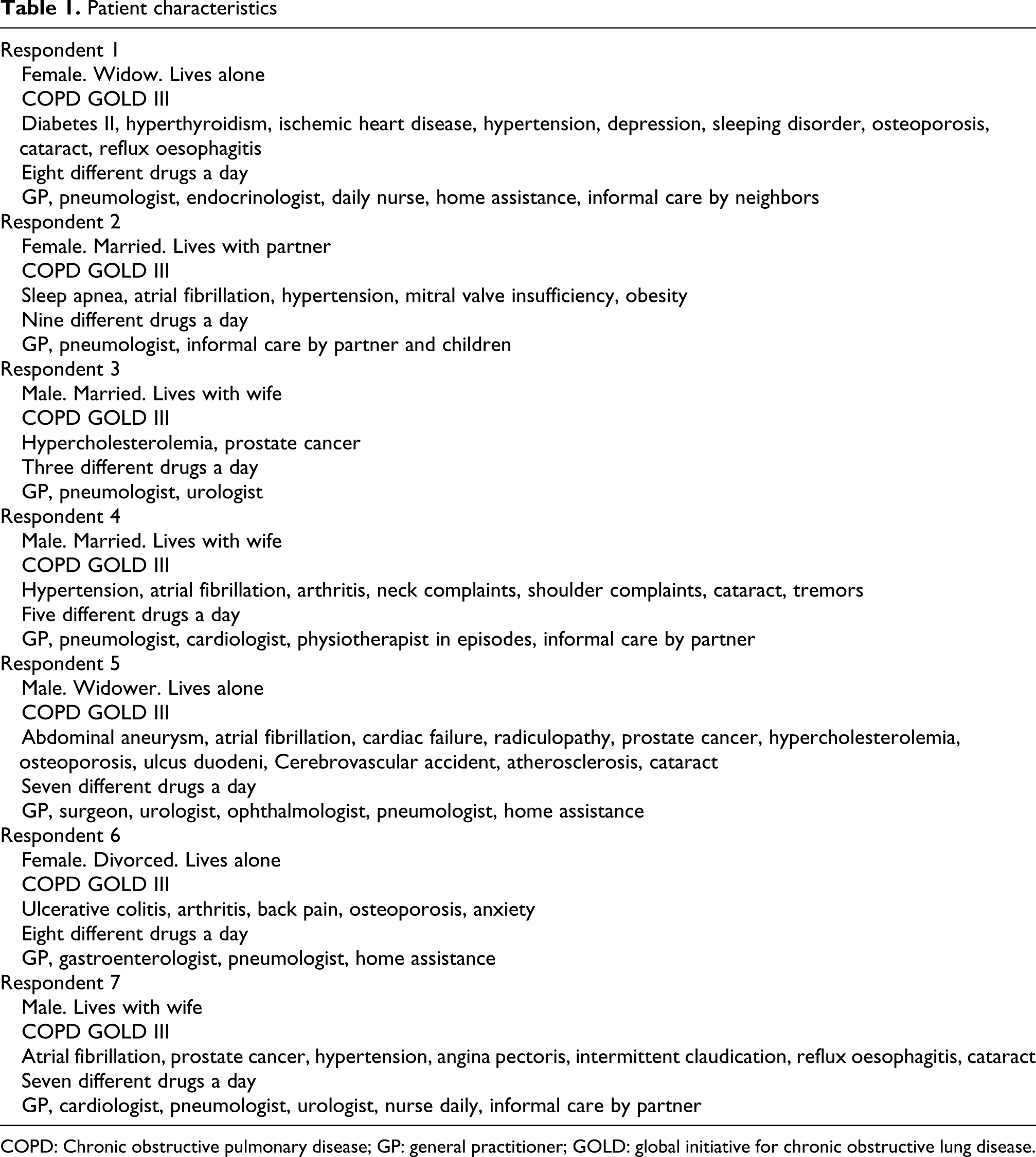
COPD: Chronic obstructive pulmonary disease; GP: general practitioner; GOLD: global initiative for chronic obstructive lung disease.
Patient interviews
The interviewer started the interview with one single question: ‘you were selected to participate because you have COPD combined with some other diseases, can you please tell me something more about this’. The interviewer did not interrupt, except for clarification. The length of the response depended only on the participant. Seven interviews of 30–90 minutes were performed. Despite the fact that a topic list was constructed to support the interview when necessary, the final analysis showed that the interviewers did not need to induce certain topics to keep the interview going.
Coding and analysis
Interviews were audiotaped and transcribed verbatim by the researchers (PB, PV, and MD) using F4 software. The text was fragmented, and each fragment was assigned with one or more codes (e.g. ‘talking to friends about the disease’). Consequently, a careful review of all text fragments categorized under a similar code was performed.
The phase of analysis started with grouping the codes together into larger categories (e.g. ‘coping’) to reveal subtle patterns and to identify key themes in the data. Next, several team discussions served to identify key themes, trends and hypotheses. The first discussion rather aimed to broaden insights into the most complex issues than to reach consensus. Later, all the identified themes and hypotheses were discussed until a consensus was reached on one set of main themes and on the underlying aspects of the themes. During both the phase of coding and the phase of analysis, researchers triangulation was essential. Each step in the process was performed twice, such that each fragmentation, coding, categorization or hypothesis formulated by one researcher was repeated independently by at least one other researcher. In case of differing viewpoints, the issue was thoroughly assessed in a joint meeting of all researchers. The systematic process of coding, sorting and review was supported by NVivo8 software.
Results
Adaptation
Patients with COPD integrate their illness and symptoms into their lives, which often leads to a positive perception of their situation, despite high morbidity. ‘In most cases I can manage’ (R3) ‘I do everything I want’ (R1). We observed adaptation strategies with a main focus on regular rest and planning and pacing activity levels.
Functional status
Functional status appears to be essential. To deepen the analysis of the numerous quotes, we used the International Classification of Functioning and Disability in Health (ICF, 2001). Mobility, domestic life and social participation were the most important chapters or domains. In line with the aforecited adaptation processes, participants remarkably emphasize on what they can achieve. Participants reported how hobbies, feeling useful and taking care of peers, impact on their well-being. ‘I have been doing that for years. If you can help people . . .’ ‘We are happy, aren’t we, the two of us watching television’ (R2) R2 ‘It's a good thing that I can work it off by reading’ (R1) R1 ‘I went to see a football match with my son again’ (R7) R7 ‘Three times a week I go to the clubhouse.’ (R2 R2 to R5). If such participation was lacking, patients felt hampered. Solitude, isolation and conflicts with relatives were frequently reported to be difficult. Self-care issues (e.g. bathing and dressing) were only reported when participants were limited in these functions.
Patients with COPD who is living alone generally seem to perceive their status as more negative and disabling. Informal care by a partner, family or, unexpectedly, by outsiders was highly appreciated. ‘My strongest weapon is my wife’ (R7).
Quotes related to anxiety were not purely related to shortness of breath or COPD but also to impending diagnoses, hospitalization and loss of independence. ‘Well, I was afraid. . . ‘ (R6). ‘Then I am thinking, oh dear, suppose I would get an attack right now, I don’t see anyone, how will I manage to get home then?’—R1 ‘And if I feel something concerning my lungs I always think of the worst’ (R2) ‘My biggest fear is to have to go and lie in the hospital and. . . don’t get out of it again . . .’ (R7).
COPD-related knowledge and attitudes
Participants knowledge of COPD appeared rather limited. ‘They say it is all because of smoking’ (R3). Several respondents report injuries to the lungs—‘It is a scar, isn’t it’ (R1) ‘Those are the alveoli bursting all the time’ (R6) and contest smoking as primary cause of COPD. ‘I had a job as a welder . . . the fumes you take in. . . much worse than a tiny cigarette, isn’t it?’ (R4). Symptoms most frequently reported were dyspnea and limited functional capacity–‘It’s like a tightness you feel’(R7) but participants did not report cough or sputum, or did they focus on exacerbations. Only one patient stated that COPD makes him readily ill, possibly referring to the frequent exacerbations provoked by upper airway infections.
Participants reported great concerns over their use of multiple drugs. ‘And slowly, you have to take more and more’ (R5). Lack of adherence was spontaneously mentioned and reported as being caused by limited effects of the drugs in controlling symptoms or the burden of side effects, such as dry mouth, palpitations and weight gain. Most were worried about habituation and addiction ‘I do not want to get addicted’ (R3) ‘Antibiotics, eventually, they don’t work anymore, do they?’ (R2) and described the financial consequences as considerable. ‘This medicine costs me a lot of money every month doesn’t it’ (R6) ‘In hospital they don’t ask in advance: “Sir, will you be able to pay for it?”’ (R4). Remarkably, inhalation therapy is not at the forefront in patients’ quotes related to medication. Some patients reported poor adherence, whereas others reported high dependence. ‘I very often forget it, don’t I. And I don’t feel any difference’– R7.
External locus of control
Participants seem to have a high external locus of control for disease: the factors reported by patients as influencing disease (such as air quality, weather, occupational activities and medical care) are mostly external factors, beyond the control of the patient. ‘This polluted air, I can feel it very well, can’t I?’ (R5). Less prominent factors were weight gain, age, emotions, restlessness and the use of alternative medicines. Striking is that smoking and physical exercise were not reported.
In line with this observation, we observed little self-management skills. Only one participant reported clearly on self-management, which was related to diabetes–‘I do that all on my own writing it down in my booklet, checking it myself’ (R1). None of the patients reported strategies to tackle exacerbations, other than calling for medical assistance.
Coping
Sense of humor, comparison with others who are worse off, acceptance of limitations, adaptation to changing capacities, changing life pace and regular resting were the most prominent coping strategies reported in the interviews, which confirms the variety in coping styles and illness cognitions in patients with COPD. ‘But you have to make jokes too, don’t you!’ (R5) ‘I wouldn’t live that long, if I wouldn’t be an optimist.’ (R6) ‘Pause a while, and go on a little’ (R1).
Discussion
This study aimed to explore perspectives of patients with COPD and comorbidities at home and relate its findings to what has been described in previous COPD specific research. Our results show significant emotional and physical adaptation that has also been reported in previous studies on COPD. 15 –23
Participants remarkably emphasize what they can achieve, despite multimorbidity, leading to a generally positive perception of functional status. Although we confirm that fear is a central point of attention in patients with COPD, this does not seem to be merely related to dyspnea and fear of suffocating. 24 –27
Patients with multimorbidity seem to be using general adaptation strategies (rest and planning and pacing) over disease specific approaches such as breathing techniques, self-management in exacerbations or medication. Social participation and partnership are most important to patients: Sexton and Munro 28 have been the first to define the consequences of COPD in terms of impact on social interactions, roles and responsibilities, and participation is a core issue in qualitative inquiries in patients with COPD. 15,29 –36 The central role of the spouse has mostly been confirmed in advanced COPD or end of life situations, 16,18,37 –41 where partners safeguard autonomy despite increasing dependency. Our work suggests that partners play an important role before the phase of increasing dependency and decreasing life expectancy.
Compared with what has been described in previous COPD specific research, our participants knowledge on COPD appeared rather limited. Where other authors 42 have shown how the vast majority of patients with COPD acknowledge smoking as the primary cause of COPD, our participants are more reluctant. It seems unlikely that this is merely due to lack of knowledge as patients with COPD are continuously questioned about their smoking history and behavior. Several qualitative studies have indeed described a complex relationship between patients with COPD and their smoking. Patients with COPD tend to look for other causes, such as occupational or environmental factors, in order to minimize their self-responsibility, 43,44 which might also be related to the external locus of control we have observed in our study. Fear of stigmatization may be an underestimated phenomenon in patients with COPD 29,45,46 and influence participants’ reports in qualitative inquiries and patients’ consultation behavior. Patients with COPD, who felt unable to stop smoking, have even been reported to avoid health care. 47
Symptom reporting also differed from previous COPD specific work with little or no reports of cough and sputum—which, however, have been defined as core issues in COPD during the development of the CAT questionnaire. 3 The fact that our respondents did not report on exacerbations is surprising and in great contrast with COPD driven research focusing on the importance of COPD exacerbations. We specifically aimed to include participants in primary care practices 12 at a moment unrelated to an acute exacerbation, hospitalization or even consultation. This could explain why our results differ from qualitative studies that recruited in hospital or immediately related to hospitalizations for exacerbations. 23,27,30,48,49
Participants seem to have a high external locus of control for disease. This is in contrast with previous work that indicates a high capability of patients with COPD to manage their own disease. 15,19,20 One possible explanation for the lack of COPD-specific knowledge and self-management skills in our study sample is the limited referral of patients with COPD to pulmonary rehabilitation programs. Despite the convincing clinical evidence of effectiveness, several thresholds impede optimal utilization of and access to pulmonary rehabilitation in Belgium: lack of referrals, lack of reimbursement and lack of supply, with only a few hospitals and/or pulmonologists being approved to provide pulmonary rehabilitation programs. It is likely that the patient education and counseling provide the knowledge, attitude and confidence to tackle COPD in a more proactive way and may also influence the reporting of disease-related fears as lack of knowledge and education and may leave patients more anxious and more dependent on health care than necessary. More emphasis on education and empowerment in daily practice could encourage self-management intervention and reduce the external locus of control for disease that was observed. However, as a single intervention, patient education on COPD has shown only a minor–but significant–change in health locus of control without any significant gains on physical function, mental health or social participation 50 : the passive nature of the interaction appears insufficient to have an effect on outcomes.
Evidence-based reviews on self-management in COPD have reported how it leads to better outcomes. 51 A recent quantitative study, 52 however, found no effect of a self-management intervention based on symptom monitoring, although the authors could define a group of ‘successful self managers’ (representing 42% of the study group), with significantly reduced readmission rates and mortality. This might indicate how self-management skills are influenced by contextual factors such as intrinsic motivation, social support, deprivation and health literacy. Compared to what has been suggested in previous COPD specific work. We concluded that our respondents generally seem to have a lower level of self-management skills. 50,53 –55 However, if we use the generic definition of self-management as described by Barlow et al. 56 as–‘the ability of patients to manage the symptoms, namely treatment, physical and psychosocial consequences and life style changes inherent in living with a chronic condition’—we might have to acknowledge that our respondents do might meet the criteria of self-management. Self-management requires a focus both on skills, cognition and reasoning as well as on disease knowledge. This lack of disease specific knowledge could explain the limited engagement in COPD specific self-management strategies. However, at the level of constructive and adaptive patterns of thought, our patients seem to show more skills than what COPD-specific research has indicated.
Our explorative work in patients with COPD and with comorbidities illustrates that coping styles are of importance in how patients perceive and experience their illness and seems to support the hypothesis on the existence of maladaptive and adaptive coping patterns. 11 Probably coping mechanisms cross the boundaries of disease. The explorative set up of the study, however, is not suitable to treat this topic in more depth or to determine how these complicated mechanisms shape outcome of medical care for patients with COPD and comorbidities. Further inquiries should define how and whether specific diseases are related to coping styles or whether coping styles are merely patient dependent.
Strengths and limitations
The present study identified some major themes in the perspectives of seven patients with COPD and comorbidity within a primary care setting. The method of convenience sampling resulted unintentionally in a sample with patients with COPD stage III. As COPD specific research clearly indicates the limited relationship between global initiative for chronic obstructive lung disease (GOLD) stage and impact at the level of the individual, 57 we did not broaden our study sample for this purpose. Throughout the analysis, an important impact of life events, such as hospital admissions, social situations and the illness of others, was observed. The impact of acute or personal events seems to predominate over the daily adaptation to disability and complaints of long-lasting and slowly progressing conditions and lead to anecdotal reporting, which did not allow us to treat topics in more depth. Therefore, we decided to limit our inclusion to the single first wave of which the last two interviews could not identify new main themes. Further qualitative inquiries should clarify the topics identified in this study such as coping, stigma and self-management. The fact that both qualitative and quantitative studies are at risk to include mostly patients of high literacy and intrinsic motivation requires particular attention.
Conclusion
Patients with COPD and comorbidity develop emotional and physical adaptation, integrating illness and symptoms into their lives. A lack of knowledge and education, however, may leave them more anxious and more dependent on health care than necessary. More emphasis on education and empowerment in daily practice could encourage self-management and reduce the external locus of control for disease that was observed. Health care providers should be attentive to fear and to smoking related stigmatization of patients with COPD. They should stimulate positive reinforcement within care by acknowledging and encouraging individual capacities, adaptation mechanisms and coping strategies, hereby crossing the boundaries of specific diseases. Social participation and, more specifically, mobility and feeling useful should be special points of attention. Close support by informal care is vital and this should be acknowledged and encouraged where possible. We believe that chronic care for patients with COPD should provide personalized rehabilitation taking into account individual patient characteristics and self-management and coping attitudes. We believe that there is a generic core to be identified, which can tackle both COPD and comorbidities. Further research is mandatory to develop these generic programs focusing on patients with complicated needs. Primary care can provide the setting for exploration.
Footnotes
Funding
The authors would like to gratefully acknowledge the support of Research Foundation Flanders (FWO).