
Abstract
Chronic obstructive pulmonary disease (COPD) is not only associated with respiratory system involvement but also with systemic consequences leading to chronic comorbidities. In this study, we aimed to investigate the effect of comorbidity severity on pulmonary rehabilitation (PR) outcomes in COPD patients. We conducted a retrospective cohort study to compare the effectiveness of PR in COPD patients who completed an 8-week PR program. There were at least one comorbid in 120 of 211 patients and we divided them into the groups according to Charlson Comorbidity Index (CCI) scores (1 points, group 1 (n = 54); 2 points, group 2 (n = 41); 3 points, group 3 (n = 25)). We compared 6-minute walk distance (MWD), dyspnea perception, pulmonary function tests, blood gases analysis, quality of life, anxiety, and depression scores which were recorded before and after PR between the groups. Before PR 6-MWD distance was significantly lower in group 2 (p = 0.033). Improvements in 6-MWD, blood gas values, dyspnea perception, quality of life, and anxiety were determined in all groups after PR (p < 0.05). When the gains after PR were compared, there were no significant differences between groups (p > 0.05). COPD patients benefit from PR independent from their comorbidity severity. Comorbidity severity has no effect on PR gains. Therefore, patients with comorbidities should not be excluded from PR programs and encouraged to participate.
Clinical Trial Number:
NCT03319108.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) does not only remain to be an important cause of mortality and morbidity in the world but also poses an important public health issue with its increasing prevalence. 1 COPD is characterized by avoidance of physical activity due to dyspnea, therefore with reduced exercise capacity, impaired quality of life, and psychological problems. 2 COPD does not only affect lungs, it is also a complicated, systemic disease with important extra-pulmonary effects. The most frequent comorbidities encountered in COPD patients are arterial hypertension, coronary artery disease, heart failure, and lung cancer. 3 These comorbidities increase the severity of the disease and worsen the quality of life and prognosis. The cause of mortality in the majority of the COPD patients is due to comorbidities. 3,4
Pulmonary rehabilitation (PR) has been defined as an evidence-based, multidisciplinary, and comprehensive intervention for patients with chronic respiratory diseases who are symptomatic and often have decreased daily life activities. 5 –7 Exercise training is the cornerstone of the PR. 3 The other components of PR are education, self-management training, nutritional, and psychological support. 7
PR has been demonstrated to increase the exercise tolerance, lower the dyspnea perception, and improve the quality of life in COPD patients. 7 However, the patients’ responses to PR differ, and no improvement can be achieved in some patients. 8 Especially, the presence and number of comorbidities may decrease the positive effects of PR on dyspnea perception, functional exercise capacity, and quality of life. 9,10 However, the results are inconsistent and, while classifications were frequently made based on the number of comorbidities in the previous studies, the effect of the comorbidity severity was not explored and more advanced diseases did not compare with milder diseases. Therefore, the aim of our study is to determine the effect of comorbidity severity on PR outcomes in COPD patients participating PR program.
Methods
We conducted a retrospective database study to investigate the effect of comorbidity severity on PR outcomes in COPD patients who completed an 8-week supervised outpatient PR program in the PR Unit at Dr. Suat Seren Chest Diseases and Surgery Training and Research Hospital in Izmir in Turkey. The study was approved by the local institutional review board on the date of January 6, 2017 (protocol number: 49109414/806.02.02). Patients included in the study completed an informed written consent form.
Subject selection
In total, 211 COPD patients diagnosed according to Global Initiative for Chronic Obstructive Lung Disease (GOLD) definition, who had completed PR program between 2013 and 2017 participated in this study. The inclusion criteria from the database to our study were a ratio of forced expiratory volume in 1 second (FEV1) to forced vital capacity (FVC) of 0.7 or less after bronchodilator use and a history of 10 or more pack-years of smoking. 11 The severity of COPD was graded according to the stages of disease defined by the GOLD. 12 We excluded patients who were diagnosed with other pulmonary diseases (asthma, interstitial lung disease), lost to follow-up, or were repeating PR from the study 13 (Figure 1).

Flowchart of the study.
Measurements
Demographics (age, gender, body mass index (BMI)), clinics (smoking history, long-term oxygen therapy, using noninvasive ventilation, emergency admission, and hospitalization in the last year) were recorded.
Comorbidity severity
We collected comorbid conditions from the patient’s medical file records and the patient’s medication list. We calculated the comorbidity severity according to the modified Charlson Comorbidity Index (CCI) 14 but excluding age as previously suggested because it would affect the results of PR. 15 In this index, the each comorbidities are scored as 1, 2, 3, and 6 from mild disease to serious disease (comorbid conditions with a weight of one include coronary heart disease, congestive heart failure, peripheral vascular disease, cerebrovascular disease, dementia, connective tissue disease, ulcer disease, mild liver disease, and diabetes. Hemiplegia, diabetes with end-organ damage, any tumor, leukemia, and lymphoma have a weight of two. Moderate or severe liver disease has a weight of three. Metastatic solid tumor and AIDS have a weight of six). And comorbidity severity is calculated according to the weighted score which is obtained by summing up the scores of comorbidities.
According to our data, we grouped our patients, those with the CCI of 1 as group 1, CCI of 2 as group 2, and CCI of
Respiratory functions
Body plethysmography (Zan 500, Germany) and carbon monoxide diffusion capacity (Zan 300, Germany) are routinely measured for all patients who are attending to our hospital’s PR program. 17 We took all pulmonary function test results from our hospitals’ database. We recorded the % predicted values of FEV1, FVC, FEV1/FVC ratio, and carbon monoxide diffusion capacity (TLCO) before and after PR program.
Assessment of dyspnea
We used “Modified Medical Research Council (MMRC)” dyspnea scale, which consists of 5 items ranging between 1 and 5, to determine the severity of patients’ shortness of breath. The score “1” represents the best level, where the score “5” indicates the poorest. 18
Exercise capacity
We recorded the walking distance in the 6-minute walk test (6-MWT) performed according to the American thoracic society (ATS) guidelines before and after PR. 19
Quality of life
We used St. George’s Respiratory Questionnaire (SGRQ) to determine disease-specific quality of life. 20 At this scale, high scores define worsened disease and increased symptoms. We assessed the overall quality of life by 36 Item Short Form Survey (SF-36) in which increased scores were considered in favor of improved quality of life. 21
Interventions
We conducted pulmonary physiotherapy and rehabilitation sessions, lasting 2 hours, twice a week for 8 weeks to all patients that joined the program. Exercise program included breathing exercises consisted of pursed-lip breathing, diaphragmatic breathing and thoracic expansion exercises, relaxation and stretching exercises, aerobic exercises, and peripheral muscle strength training. Patients performed aerobic exercises for 30 minutes, which consisted of the treadmill and static bicycle ergometer. We calculated both workloads for cycling and walking speed for treadmill from 6-MWT. Treadmill walking speed was calculated using the following formula: (6-MWT distance × 10)/1000 × 0.8 km/h. Cycling workload was calculated with the formula (Watt = 103.217 + (30.500 × sex) + (−1.613 × age) + ((0.002 × distance × weight)) sex; male = 1 female = 0). 22 We were careful to keep the peak heart rate between 60% and90% of maximal heart rate. Exercise intensity increased according to patient progress. We used pulse oximetry to supervise patients during exercises, and, if the SpO2 fell below 90%, oxygen supplementation was provided. Patients performed upper and lower extremity strengthening exercises using free weights, with resistance gauged to their tolerance. The number of repetitions was progressed from 8 to 10. When the patient was able to perform the load for 1 or 2 repetitions over the target number, we increased it by 2–10%. Rest periods were 2 minutes between sets and 1 d between sessions. In addition, we regulated exercise intensity for both aerobic and strengthening program by modified BORG dyspnea scores (between 4 and 6). 5,7,19
Statistical analysis
Statistical analysis of the data obtained in the study was performed using “Statistical Package for Social Science for Windows version 17” statistics software. Distribution normality of the data was checked by Kolmogorov–Smirnov test. Since the data were not normally distributed, continuous variables were expressed as median (interquartile range (IQR)), and categorical variables as percentage (%). Wilcoxon signed-ranks test was used for the comparison of the pretreatment and posttreatment measurable values of the same group. Kruskal–Wallis H test was conducted to compare the data between groups. The Mann–Whitney U test performed to test the significance of pairwise differences using Bonferroni correction to adjust for multiple comparisons. The analysis of categorical data was performed using χ2 test. The value of p < 0.05 is considered as statistically significant.
Results
In total, 211 COPD patients with a median age of 64 included in our study. The demographic and clinical characteristics of the patients are shown in Table 1. At least one comorbidity was found in 120 patients (56.8%) of the study participants.
Comparison of baseline values of the patients with and without comorbidity.a

FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity; TLCO: carbon monoxide diffusion capacity; PaO2: partial arterial oxygen pressure; PaCO2: partial arterial carbon dioxide pressure; SaO2: arterial saturation; MMRC: modified Medical Research Council; SGRQ: St George Respiratory Questionnaire, SF-36: 36 Item Short Form Survey; HADa: Hospital Anxiety Depression anxiety score; HADd: Hospital Anxiety Depression depression score; BMI: body mass index.
a Data are presented as median (interquartile range) or percentage (%).
b Kruskal-Wallis H Test and χ2 Square Test.
*Mann–Whitney U test.
Compared with baseline measurements of patients with and without comorbidities, patients in the comorbid group had significantly higher age (p < 0.001), disease duration (p = 0.018), BMI (p < 0.001), and significantly lower 6-minute walking distances (6-MWD) (p = 0.020, Table 1).
In terms of respiratory function tests, FEV1/FVC, TLCO values, and the number of stage 2 patients were higher in the comorbid group (p < 0.05, Table 1).
The most frequent comorbidities were hypertension (n = 39, 32.5%), diabetes mellitus (n = 17, 14.2%), coronary artery disease (n = 12, 10.0%), osteoporosis (n = 12, 10.0%), and lung cancer (n = 11, 9.2%), respectively. The other comorbidities were osteoarthritis (n = 8, 6.6%), goiter (n = 7, 5.8%), cancer (n = 6, 5.0%), benign prostatic hyperplasia (n = 5, 4.1%), rheumatoid arthritis (n = 1, 0.8%), ankylosing spondylitis (n = 1, 0.8%), depression (n = 1, 0.8%), and panic attack (n = 1, 0.8%) (Table 2).
Comparison of baseline values of groups according to severity of comorbidity.a

FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity; TLCO: carbon monoxide diffusion capacity; PaO2: partial arterial oxygen pressure; PaCO2: partial arterial carbon dioxide pressure; SaO2: arterial saturation; MMRC: Modified Medical Research Council; SGRQ: St George Respiratory Questionnaire; SF-36: 36 Item Short Form Survey; HADa: Hospital Anxiety Depression anxiety score; HADd: Hospital Anxiety Depression depression score; BMI: body mass index; 6-MWT: 6-minute walk test.
a Data are presented as median (interquartile range) or percentage (%).
b Kruskal-Wallis H Test and χ2 Square Test.
*Mann–Whitney U test.
When the baseline demographic and clinical features of the groups were compared, data for age, gender, disease duration, COPD stage, amount of cigarette consumption, emergency admission and hospitalization in the last year, and number of patients using long-term oxygen therapy were similar (p > 0.05, Table 2). Patients in the group 2 had higher BMI than group 1 (p < 0.001, Table 2). In addition, the number of patients using noninvasive mechanical ventilation was significantly higher in group 2 (p = 0.037, Table 2). The groups were similar in terms of pulmonary function tests, arterial blood gas results, MMRC dyspnea scores, overall and disease-specific quality of life subscores, anxiety, and depression (p > 0.05, Table 2). The median value of 6-MWD was lower in group 2 than the other groups (p = 0.033).
After PR, median FEV1% were significantly increased only in group 2 (p = 0.017, Table 3), no significant change was detected in none of the pulmonary function test parameters in group 3 (p > 0.05, Table 3). PaO2, SaO2, 6-MWD, dyspnea perception, anxiety, and many parameters in the SGRQ and in the SF-36 questionnaire were significantly improved in all three groups (p < 0.05, Table 3).
Results of the groups before and after PR.a

RFT: respiratory function test; ABG: arterial blood gas; FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity; TLCO: carbon monoxide diffusion capacity; PaO2: partial arterial oxygen pressure; PaCO2: partial arterial carbon dioxide pressure; SaO2: arterial saturation; MMRC: Modified Medical Research Council; SGRQ: St George Respiratory Questionnaire; SF-36: 36 Item Short Form Survey; HADa: Hospital Anxiety Depression anxiety score; HADd: Hospital Anxiety Depression depression score; 6-MWT: 6-minute walk test; PR: pulmonary rehabilitation.
a Data are presented as median (interquartile range).
b Wilcoxon signed-ranks test.
When the gains of the groups after PR were compared, there were no significant differences between groups according to the changes in PR outcomes (p > 0.05, Table 4).
Comparison of the improvements of the groups after PR.a
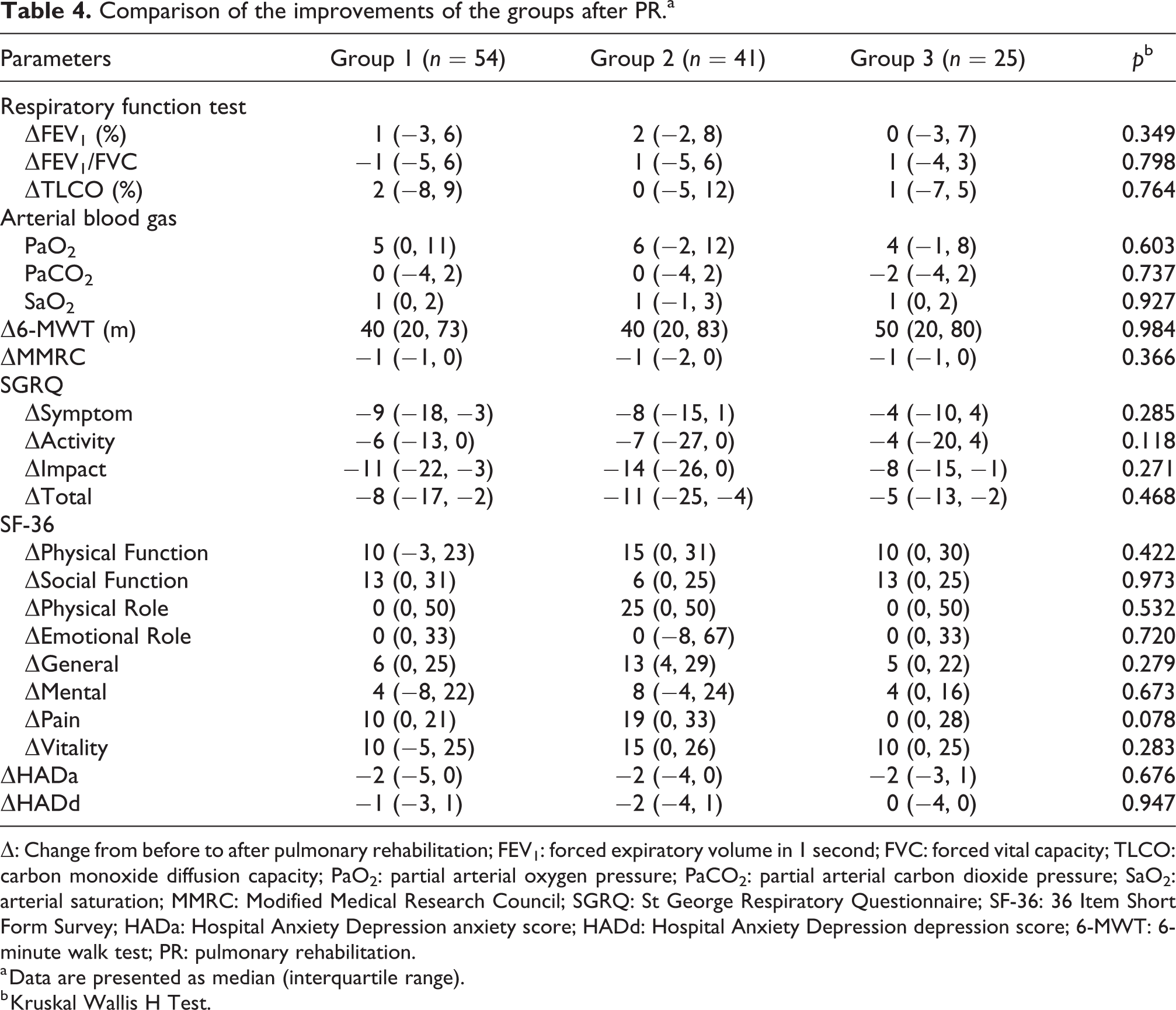
Δ: Change from before to after pulmonary rehabilitation; FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity; TLCO: carbon monoxide diffusion capacity; PaO2: partial arterial oxygen pressure; PaCO2: partial arterial carbon dioxide pressure; SaO2: arterial saturation; MMRC: Modified Medical Research Council; SGRQ: St George Respiratory Questionnaire; SF-36: 36 Item Short Form Survey; HADa: Hospital Anxiety Depression anxiety score; HADd: Hospital Anxiety Depression depression score; 6-MWT: 6-minute walk test; PR: pulmonary rehabilitation.
a Data are presented as median (interquartile range).
b Kruskal Wallis H Test.
As shown in Table 5, there was no significant difference in the number of patients reaching the minimal clinically important difference (MCID) between the groups.
Patients with positive response (MCID) to PR in terms of improvement in exercise tolerance, dyspnea, and quality of life.a
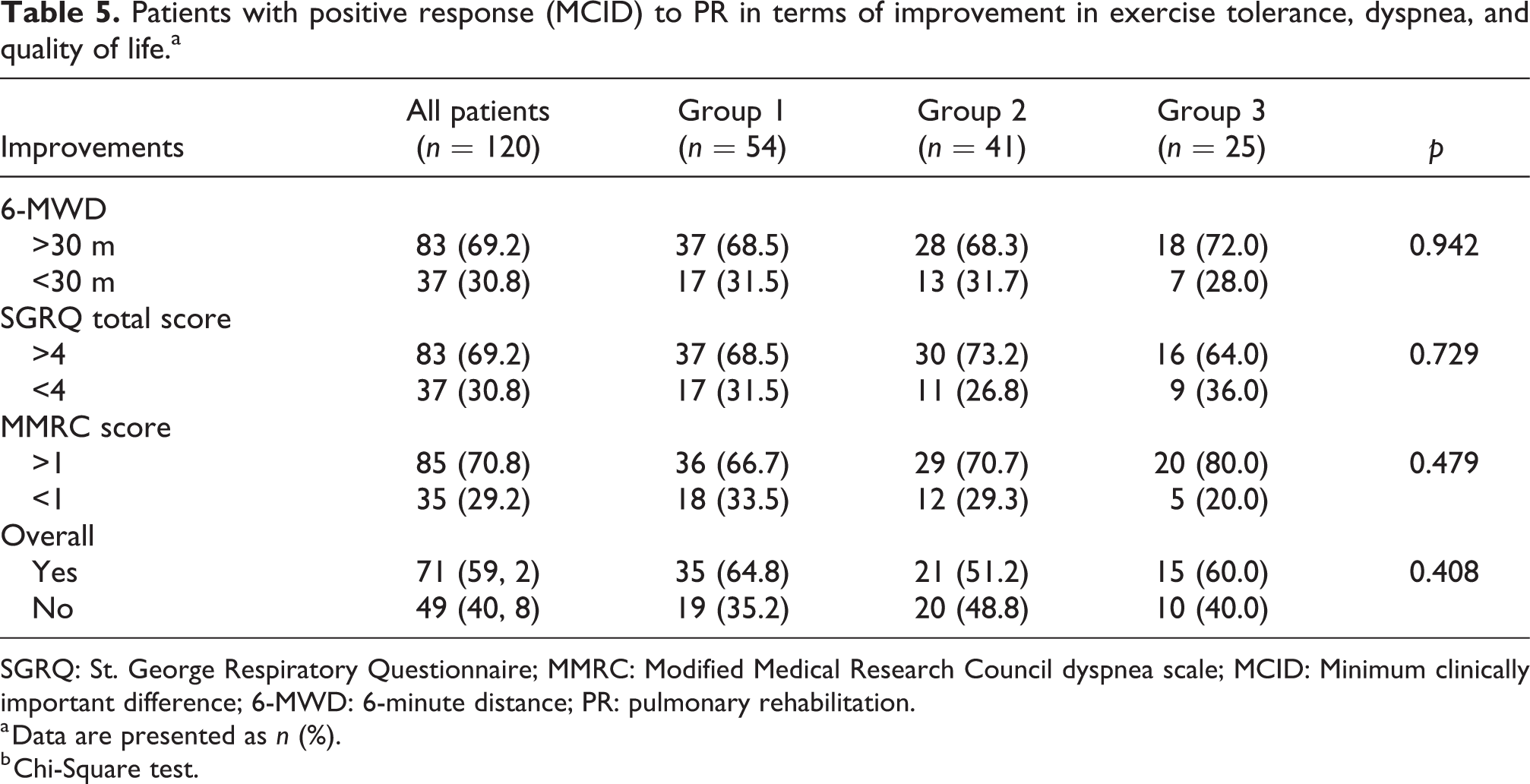
SGRQ: St. George Respiratory Questionnaire; MMRC: Modified Medical Research Council dyspnea scale; MCID: Minimum clinically important difference; 6-MWD: 6-minute distance; PR: pulmonary rehabilitation.
a Data are presented as n (%).
b Chi-Square test.
Discussion
In our study which we aimed to determine the effect of comorbidity on PR outcomes in COPD patients, we found that gains of PR were not related to comorbidity severity. When we compared the gains of PR between all groups, we observed that the improvements were similar in patients with different severity of comorbidities.
The results of our study are similar to some studies in the literature. In a previous study by Tunsupon et al., patients were classified according to their number of comorbidities and the results showed that the number of comorbidities had little effect on the gains after PR. Moreover, in that study, there was no difference in the number of comorbidities between those reaching and not reaching the MCID in 6-MWD and in the disease-specific quality of life scores. 13 In the two other studies which used the same grouping, similar improvements were obtained in all groups after PR. From these studies, Hassan et al. stated that the number of comorbidities between responders and nonresponders for 6-MWD, MMRC, SGRQ, and VO2max measured after PR did not differ. 3,23 In another study by Higashimoto et al., it has been shown that the individual comorbidities have no relation to the PR results and PR has equal efficacy in young and elderly patients with COPD. 24 In contrast to our results, Crisafulli concluded that exercise tolerance and quality of life in COPD patients might be reduced due to comorbidity, and the CCI score was negatively correlated with the 6-MWD increase. 4
In many studies examining the effect of comorbidity on PR outcomes in COPD patients, they grouped patient according to the number of comorbidities as with no comorbidity, with only one comorbidity and with two or more comorbidities. 3,4,13,23 Unlike other studies, we examined the effect of comorbidity severity on PR outcomes. For this aim, we used the CCI that is a reliable, valid, and well correlated with mortality. 14 This index scores the severity of comorbidities of patients in the framework of certain diagnoses. However, pathologies such as hypertension, osteoporosis, goiter, and loss of muscle strength which are very common in the clinic are skipped in this scoring. In our study, although patients had additional comorbidities, they were not scored. When using such a scoring system, we show that the PR gains are independent of the severity of the comorbidity, so it might be more appropriate to interpret the effect and gains according to the systemic effects of the types of the comorbidities.
In one form of the CCI, a point is added for every decade over the age of 40, so the CCI score increased with the advancing age. 25 When we include age in the calculation, the groups were separated into older and younger rather than the burden of comorbidities. Therefore, in our study, we thought that this form was not appropriate for grouping and not included age to the calculation because the age would affect the results of PR.
Extrapulmonary comorbidities are very common in COPD patients, and they usually have important effects on symptoms, exacerbations, hospital admissions, and mortality. 26 Systemic inflammation may be responsible for the concurrence of COPD and comorbidities. 10,26 Moreover, physical inactivity plays an important role in this concurrence. 10 Also, smoking, socioeconomic status, and occupational exposure are the common causes of COPD and accompanying comorbidities. 27
In our study, we first examined the data of patients with and without comorbidities, and we found that the exercise capacity of the patients with at least one comorbidity was worse. Besides, patients with comorbidity had a higher age and disease duration. This supported the idea that comorbidities were related to increasing age and pathophysiology of COPD leading to an increase in functional disability. 27 –30
In many studies, 6-MWD was found to be significantly lower in patients with two or more comorbidities. 4,8 In our study, the walking distance was significantly lower in the group with intermediate comorbidity index scores (CCI score = 1) compared to the group with low comorbidity index score. We think that this is because of the number of patients with different comorbid conditions as diabetes mellitus, coronary artery disease, and higher BMI. Moreover, one of the reasons for the high functional scores of the group with high comorbidity severity might be that it was not in the active periods of cancer patients and the clinical conditions were under control.
When we analyzed the distribution of disease stage among the groups in our study, especially in the comorbid group, stage 2 patients were intensive. This may be the answer to the question of why obstruction and TLCO ratio are higher in the comorbid group, although FEV1% values are similar. In fact our results about the distribution of disease states are consistent with the some new literature, which stated that comorbidity can occur in patients with any degree of airflow limitation and is not restricted to patients with advanced COPD. The excessive number or severity of comorbidity cannot always be explained by poorer physical or respiratory function and GOLD stage is not an independent predictor of comorbidity. 9,16
In COPD patients, the results of the comorbidity effect on quality of life are contradictory. 4,29,31 In our study, we observed that the quality of life did not change with the presence of comorbidity and its severity. We think that the reason for this is the development of patients’ compliance with chronic comorbidities and especially the difficulties experienced by COPD are similar.
The most frequent comorbidities seen with COPD are cardiovascular diseases being in the first place, followed by metabolic diseases, osteoarticular, and oncological disease. 4,27–30 There was at least one comorbidity in 56.3% of our patients in this study. Similar to the literature, the first five comorbidities seen together with COPD in our study are hypertension, coronary artery disease, osteoporosis, diabetes mellitus, and lung cancer.
In our PR unit, a detailed medical history is taken and comorbid conditions are questioned and, a detailed cardiac examination is performed for patient safety before the PR program. For this reason, the possibility of omitting the comorbid conditions in the index which we used in our patient records is very low. One of the most important limitations of our retrospective study might be the omission of diagnosis of osteoporosis which is not examined by bone mineral density even though it is questioned in patient interviews. However, we think that osteoporosis does not affect the results because it is not included in comorbidity severity calculation.
In this study, walking distance was significantly increased and dyspnea perception was significantly decreased in all groups after PR. While significant improvements were observed for FEV1% in group 2, no significant improvement was detected in any of the respiratory function parameters in the others. Although the difference was not significant, in group 2, FEV1% was lower and the number of stage 4 patients was higher than the other groups before PR. Therefore, the result that FEV1% gain after PR is only significant in group 2 could be explained by the view that the patients with worse respiratory functions benefit more from the PR program. We thought that the FEV1% gain was associated with the PR program because all patients participating in the study were receiving bronchodilator therapy and no changes were made in medical treatment during the PR program.
When we evaluated our results by considering the minimal clinical significance levels, we found that in all three groups, walking distance gain over 30 metrics, change of MMRC dyspnea scale more than 1 unit and a decrease of 4 units of SGRQ quality of life total score in the majority of patients. In general, 60% of the patients showed improvement in all scores. Again, in this analysis, we concluded that the severity of comorbidity did not lead to a significant difference for the positive response.
Consequently, this study shows that COPD patients benefit from PR independent from their comorbidity severity. Therefore, we believe that all patients with different severity comorbidities should not be excluded from PR programs and encouraged to participate.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.