
Abstract
Background:
The aim of this study was to analyse the economic impact of nonadherence to the Global Initiative for Obstructive Lung Disease (GOLD) guidelines in patients with chronic obstructive pulmonary disease (COPD).
Methods:
A retrospective analysis was carried out on a claim database. Patients aged at least 40 years with a diagnosis of COPD were eligible for this analysis. Demographics, medical data and use of resources were collected and direct and indirect costs were analysed (from January 2008 to June 2009). A probabilistic multivariate sensitivity analysis of avoided costs was carried out. All results are presented in annualized form and costs are expressed in Euros (2009).
Results:
A total of 1365 patients were included, 79.5% were men. The mean age (±standard deviation) was 71.4 (±10.3) years, the mean forced expiratory volume in 1 s (FEV1) was 65.3% and they had a COPD history of 5.5 (±2.9) years. Patients were divided into an adherent group and a nonadherent group depending on whether therapeutic recommendations according to severity defined in the GOLD guidelines (2007) were followed. Patients in both groups were also classified as having stage II (FEV1 < 80% and < 50%) or stage III disease (FEV1 < 50% and ≥ 30%). The total annual drug cost per patient in the nonadherent group was €771.5 while it was only €426.4 for the adherent group. The average direct cost per patient per year in the nonadherent stage II group was €1465 (±971) and it rose to €2942 (±1918) for patients in the nonadherent group with stage III disease. The potential saving from the implementation of the GOLD guidelines in stage II COPD amounted to €758 per patient per year (68% saving on drug cost). In contrast, the cost for patients with stage III disease was higher in the adherent group versus the nonadherent group (€2468).
Conclusions:
The cost of COPD may vary according to compliance with the GOLD guidelines. The cost observed for patients with stage II disease is higher than expected in patients who adhere to treatment, but patients with stage III disease treated according to the GOLD guidelines had significantly higher treatment costs.
Introduction
The prevalence of chronic obstructive pulmonary disease (COPD) in the general population is believed to be between 1% and 10% [Halbert et al. 2006; Chapman et al. 2006; Peña et al. 2000] and it is estimated that around 10.2% of people aged 40–80 in Spain have this condition [Peña et al. 2000; Miravitlles et al. 2009b]. COPD is the fifth biggest cause of death among men in Spain and the seventh among women, with annual rates of 61 per 100,000 people and 20 per 100,000 people respectively in 2005 [Centro Nacional de Epidemiología, 2009].
The high prevalence and associated healthcare costs, especially those generated by hospital admissions [Strassels et al. 1996; Grasso et al. 1998; Sullivan et al. 2000; Miravitlles et al. 2003], have prompted guidelines to be established at an international level to improve the management of these patients. In fact, a recent audit of admitted patients in Spain has provided information about the great variability in patterns of treatment and outcomes [Pozo-Rodríguez et al. 2012]. This variability may be more relevant in patients with high risk of readmission, those with increased dyspnoea, and impaired lung function and exercise capacity [García-Polo et al. 2012; Alcázar et al. 2012].
Currently, the Global Initiative for Obstructive Lung Disease (GOLD) guidelines are the most widely recognized [GOLD, 2011]. However, dissemination of and compliance with guidelines is not optimal and treatment patterns do not always comply with existing guidelines. This would explain the variability in the use and costs of treatment for COPD [Miravitlles et al. 2003, 2009a; Miravitlles and Figueras, 2001; de Miguel Díez, 2005; Masa et al. 2004] and, in turn, the increasing interest in identifying the actual patterns of use in these patients [Miravitlles et al. 2008]. The objective of this study was to evaluate the real costs associated with COPD according to adherence to the GOLD recommendations.
Materials and methods
Design
A multicentre, retrospective, observational study estimated the annual cost of treating patients with COPD using the records in a medical database of patients treated in primary care in Spain. The patients were classified into two groups: those in whom the GOLD guideline recommendations were adhered to (adherent group) and those in whom they were not (nonadherent group). The analysis was carried out from a healthcare perspective but was broadened to reflect the social perspective (direct and indirect costs). The follow-up period for the observational study as a whole was 18 months (from January 2008 to June 2009), although the results were annualized. The costs have been expressed in Euros (2009) and the costs of all drugs analysed were reimbursed by the National Security System.
Sample size
Approximately 61% of patients with COPD in Spain are treated in the primary care setting, with an average of 5.3 [standard deviation (SD) 12.4] visits per year. Of these, 1.3 (SD 4.7) are to specialists, 0.7 (SD 3.0) to emergency services and patients spend an average of 1 day in hospital (SD 5.3) [Izquierdo-Alonso and de Miguel-Díez, 2004]. From these figures, it was estimated that a sample of 624 patients would allow a difference of 2 days to be detected in the calculation of the mean total number of visits, assuming a maximum SD of 25.5 days and a confidence interval of 95%. The sample was then overestimated by an additional 10% to avoid any possible bias caused by assuming that the resources followed a normal distribution.
Ethics Committee
The study was approved by the Ethics Committee of the Hospital Clínic de Barcelona and patient anonymity and data confidentiality were preserved. Data were extracted for analysis from the medical records so that the patients being assessed could not be identified.
Study population
The study population consisted of men and women belonging to six primary care centres (EAP Martí Julià, EAP La Riera, EAP Montigalà, EAP La Morera, EAP Nova Lloreda and EAP Montgat-Tiana), managed by Badalona Serveis Assistencials SA. These centres provide healthcare coverage to 107,208 people, 15.6% of whom are over the age of 64, in a medium-to-low socioeconomic, predominantly industrial, urban setting. The patients had an established clinical diagnosis of COPD plus a postbronchodilator forced expiratory volume in 1 s (FEV1) of less than 80% of the predicted value. They were aged 40 years or above and were registered in the centres’ long-term repeat-prescription schemes. Patients with a history of asthma, allergic rhinitis or atopy were excluded, as were those on treatment with antiallergy drugs (antihistamines, cromones).
The computerized medical records were created using the OMI-AP tool (software package for primary care), which is a patient-centred, problem-orientated record model which allows patient progress to be recorded according to episodes, reasons for consultation or diagnoses for care. Demographic data (date of birth and sex), FEV1 measurements and certain elements of previous medical history (conditions at the time of inclusion) which might affect the use of resources by patients with COPD were obtained from the medical records at the different centres. The healthcare resources compiled were primary care appointments, specialist referrals, diagnostic tests ordered, visits to emergency services, hospitalizations (number of admissions and duration of stay in days), days of temporary sick leave, prescribing of oxygen therapy and drugs administered during the 18-month study period. This database has been validated and used in previous studies [Rubio Gil et al. 2011].
There was no information available on the database on the FEV1/forced vital capacity ratio or the number of exacerbations for each patient. The number of exacerbations was therefore defined as the maximum number among the number of visits to the emergency services, hospital admissions and the number of prescriptions for systemic corticosteroids or antibiotics.
Drug treatment for chronic obstructive pulmonary disease according to the Global Initiative for Obstructive Lung Disease
Although a new GOLD document was launched in November 2011 [GOLD, 2011], the lack of information on Modified Medical Research Council Dyspnea Scale and COPD Assessment Test scores does not allow us to investigate adherence to these recommendations. Moreover, the guidelines in place at the time of data collection were the previous GOLD guidelines [Rabe, 2007]. The GOLD 2007 recommendations were based on stepwise drug treatment according to the FEV1, with the first treatment step in any stage being smoking cessation [Rabe, 2007]. For patients with stage II disease, when the FEV1 is between 50% and 80%, the recommended treatment is the addition of one or more long-acting bronchodilators. In patients with severe stage disease (III and IV), if they have more than two exacerbations per year, the addition of inhaled corticosteroids is justified. For patients with stage III disease (FEV1 between 30% and 50%), theophylline is the next bronchodilator to add and in patients with stage IV disease, with FEV1 less than 30%, the option is to combine all the therapeutic groups.
Distribution of treatment according to the Global Initiative for Obstructive Lung Disease
Considering the pharmacological recommendations according to stage and the number of exacerbations, the patients with COPD were classified as ‘as per guidelines’ (adherent group) or ‘not as per guidelines’ (nonadherent group) as follows:
Patients with stage II disease were included as adherent except when they had prescriptions of fixed combinations of β2-adrenergic agonists and inhaled glucocorticoids or inhaled glucocorticoids alone.
Patients with stage III disease with two or fewer exacerbations per year were subject to the same classification criteria as patients with stage II disease.
Patients with stage III disease with two or more exacerbations per year were included as adherent except when they had prescriptions of systemic glucocorticoids or systemic antibiotics.
Costs
To assess direct costs, the drug cost [Consejo General de Colegios Oficiales de Farmacéuticos, Base de datos del Medicamento, 2009] and the unit cost applied to each resource [Gisbert and Brosa, 2009] were used. The indirect costs were calculated using the human capital method, which consists of applying the gross earnings standardized by sex and age group using official data from the Instituto Nacional de Estadística (INE; National Statistics Institute) 2007 salary structure survey for each day of work lost [INE, 2007]. The gross earnings refer to the income, in cash and in kind, paid to workers for time worked or work done, along with payment for periods of time not worked, such as vacation leave and public holidays. The costs coming from other years were updated to 2009 according to the Spanish consumer price index [INE, 2009].
Although it was possible to identify patients with oxygen therapy, as there was no record of the actual amounts used, the annual consumption and corresponding cost had to be estimated on the basis of the average cost of oxygen therapy per session [Gisbert and Brosa, 2009], multiplied by the number of sessions in a year adjusted by the level of compliance observed in the Spanish study by Pérez de Alejo and colleagues [Pérez de Alejo et al. 2009].
Statistical analysis
Descriptive and inferential statistics were used to analyse the data, with the χ2 test or Fisher’s exact test to compare qualitative variables and Student’s t test, analysis of variance, Mann–Whitney U test or Kruskall–Wallis test, depending on the application conditions, for quantitative variables. Prior to the comparisons, the application of parametric methods was studied (Kolmogorov–Smirnov), and if this was not possible, nonparametric tests were performed. To evaluate the cost comparisons, they were first normalized by Box–Cox transformation. The statistical analysis was carried out with the SPSS 15.0 statistics package and p value less than 0.05 was chosen as the level of significance a priori.
A probabilistic sensitivity analysis was carried out using the bootstrap simulation technique to be able to incorporate the uncertainty of the model parameters into the results of the study. This type of simulation allowed us to validate the results by generating 1000 samples of the same size (n = 500) and obtaining a measure of the variability of our results. We were thus able to carry out an internal validation (robustness) of our results, thereby observing how modifying the type of patient cohort studied would change the result.
Results
The study rationale and the patient characteristics according to COPD stage are shown in Figure 1. A total of 1365 patients, primarily men (79.5%), were included (Table 1 and Figure 1) with a mean age of 71.4 years (SD 10.3) and time since COPD diagnosis of 5.6 years (SD 3.0). The mean FEV1 was 65.3% (SD 11.0%), with 7.5% (n = 103) of the patients having a FEV1 between 30% and 50% and none having an FEV1 less than 30%. The majority of patients had some type of associated comorbidity (89.6%) in addition to COPD, the most common being hypertension (52.7%) and dyslipidaemia (41.2%). Among the patients with stage III COPD, there was a higher trend in the number with ischaemic heart disease (15.5% versus 22.3%, p = 0.071).

Study flowchart. COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 s; GOLD, Global Initiative for Obstructive Lung Disease.
Demographic characteristics of the population studied.

COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 s; SD, standard deviation. *statistically significant.
Approximately 18.0% of the patients included belonged to the Adherent group, which had 7.7% more men than the nonadherent group (p = 0.007).In terms of risk factors, it was observed that the percentage of smokers in the nonadherent group was significantly lower than in the adherent group (24.9% versus 34.2%, p = 0.003) (Table 1).
Use of resources
The patients made a total of 16,824 visits per year, with a mean of 8.3 (SD 4.4) and 7.8 (SD 4.2) visits per patient per year (to primary care, interdisciplinary consultations and visits to specialists) for the nonadherent group and adherent group patients respectively (p = 0.103) (Table 2). The annual mean for visits to specialists was higher in the nonadherent group than in the adherent group (p = 0.008) (Table 2). A closer look at patients with stage II disease showed that the adherent group had less access to specialists (18.8% versus 35.3%; p < 0.001) and made fewer visits (p < 0.001).
Annual use and unit costs of resources.

Data presented as mean (standard deviation).
p < 0.01
INE, Instituto Nacional de Estadística (National Institute of Statistics).
The adherent patients required admission to hospital for an annual mean of 1.6 days. In contrast, the annual mean for nonadherent patient admissions was 0.3 days (p < 0.001).
In terms of diagnostic tests, spirometry was only performed an average of 0.19 times per year in adherent patients while the figure for nonadherent patients was 0.23 (p = 0.076). The oxygen therapy prescribing rate for adherent patients was double that for nonadherent patients (24.1 versus 11.1, p < 0.001).
Moreover, it was found that 2.8% of adherent patients and 5.5% of nonadherent patients took time off work (p = 0.081), although no significant differences were observed between the two groups with respect to the number of days on sick leave. Nevertheless, while not significant, overall, the mean number of days on sick leave was higher for the adherent group than for the nonadherent group (Table 2).
Drug treatment
COPD-related drug use is shown in Table 3. The most widely used treatments were cough and cold remedies (73.2%), anticholinergics (61.5%), β2-adrenergic agonists (61.2%), systemic antibiotics (61.0%) and β2-adrenergic agonists and inhaled glucocorticoids (53.3%). In the Adherent group, β2-adrenergic agonists (71.9% versus 58.8%, p < 0.001) and anticholinergics (72.4% versus 59.1%, p < 0.001) were prescribed most often. In contrast, inhaled glucocorticoids (6.5% versus 34.5%, p < 0.001) were prescribed less. It was found that 14.6% of adherent patients were prescribed β2-adrenergic agonists with inhaled glucocorticoids, as opposed to 61.8% of nonadherent patients (p < 0.001), which was due in part to the way in which patients were classified. Prescribing theophylline, which according to the GOLD guidelines is only recommended for patients with stage III–IV disease, was found for 4.8% of the nonadherent patients with stage II disease.
Description of treatments used (%) in the two study groups and in total.

Cost of clinical practice
The annual drug cost for nonadherent patients was essentially due to the use of fixed combinations of β2-adrenergic agonists and inhaled glucocorticoids (€404.97) and anticholinergics (€198.05). For adherent patients, the annual drug cost was primarily due to anticholinergics (€200.77) and β2-adrenergic agonists (€123.49). Consequently, the nonadherent group annual drug cost was €771.47 per patient/year (median €657.63) and that of the Adherent group was €426.40 per patient/year (median €153.29), €345.07 less (Table 4).
Mean drug costs per patient (€) (18 months).

Data presented as mean (standard deviation).
The mean direct cost per patient and year for the nonadherent patients with stage II disease was €1465 (SD €971; median €1291) and, in nonadherent patients with stage III disease it was €2942 (SD €1918; median €2595). The relative weight of resource use over the total costs differed among the nonadherent patients according to the severity of the COPD. While the mean direct costs in patients with stage II disease were due to drugs (50.9%) and visits and diagnostic tests (41.5%), for patients with stage III disease, the direct costs mainly came from hospitalizations (29.7%), drugs (29.1%), and to a lesser extent, from visits and diagnostic tests (22.6%) (Figure 2).
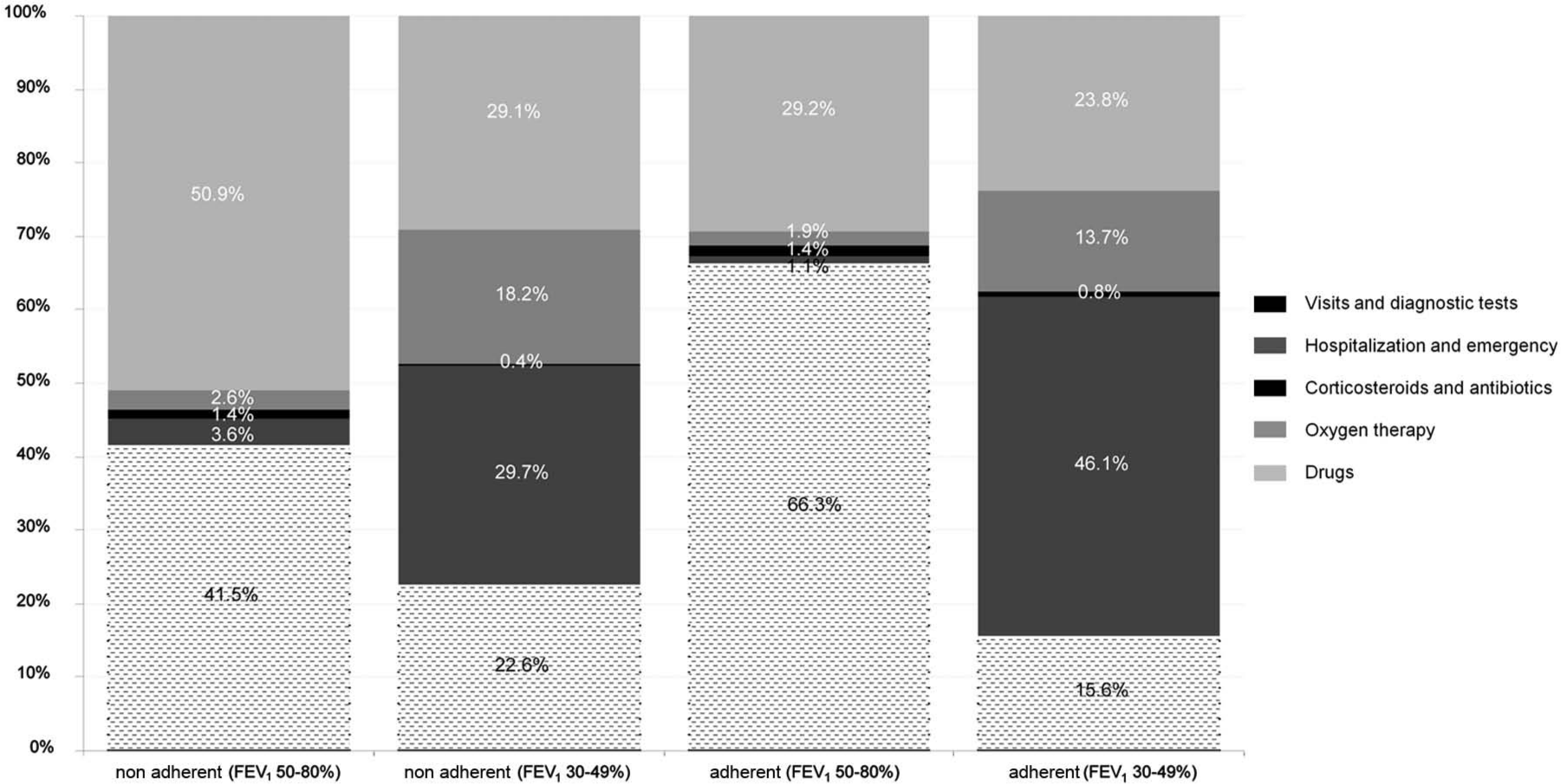
Distribution of annual direct costs according to adherent stage and patient. COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 s; adherent Global Initiative for Obstructive Lung Disease.
The indirect costs for nonadherent patients represented 9.4% and 16.9% of the total cost for stages II and III disease respectively. In Adherent patients with stage III disease, the indirect costs represented 12.9% of total costs (Table 5).
Annual cost per patient (€) of the clinical practice, GOLD costs and nonadherent costs.

Data presented as mean (standard deviation) or mean (95% confidence interval).
Cost difference is nonadherent costs minus adherent costs.
Cost differences
The results for the overall annual cost (direct plus indirect costs) per patient in the defined scenarios and the calculation of the difference in costs are shown in Table 5. It can be seen that the mean total annual cost per patient with stage II disease was €859 (median €706) for the Adherent group and €1617 (median €1336) for the nonadherent group. The costs for the Adherent patients were therefore €758 less than for the nonadherent patients (68% of the savings were from drug costs). Analysis of the cost of the Adherent patients with stage III disease showed that the direct costs for the nonadherent patients were €2294 less than those for the adherent patients and the increase in total costs was €2468. This difference was due to the increase in hospitalization costs observed (58%) in the adherent group. In short, from the simulation of 1000 bootstrap scenarios with 500 patients, it was found that with both scenarios, greater adherence to the GOLD guidelines would produce average savings of approximately €501–996 for stage II disease and an increase in costs of €1496–3277 for stage III disease (Figure 3).

Costs avoided according to forced expiratory volume in 1 s (1000 bootstrap simulations of 500 samples). Nonparametric bootstrapping draws samples (1000) from our sampled data. The figure shows the distribution of avoided costs between the Adherent group and the nonadherent group for each bootstrap sample generated. Adherence to the GOLD guideline produces savings for stage II and increases costs for stage III. GOLD, Global Initiative for Obstructive Lung Disease.
Discussion
Strict adherence to the GOLD guideline treatment recommendations is associated with drug savings for the health service when the patients have stage II disease. However, we have to be aware that there may be patients who received more treatment than recommended because their symptoms were more severe. In contrast, when patients with stage III disease were treated according to guidelines, this led to an increase in total costs, mainly due to an increase in the number of hospitalizations and hospitalization days. The cost of extra exacerbations or admissions cannot therefore be attributed to being ‘as per guidelines’ or ‘not as per guidelines’. Because this is not a randomized study, we cannot rule out a bias due to indication, when patients with more severe disease were treated according to guidelines compared with patients with fewer risk factors for admission who could have received treatment that does not follow GOLD guidelines. It has to be borne in mind that exacerbations are responsible for a large part of the direct and indirect costs of COPD [Miravitlles et al. 2003] and for the greater perception of reduced quality of life for the patients [Miravitlles et al. 2004].
To date, the only comparison made in our area between the GOLD recommendations and clinical practice looked at drug costs using a theoretical method [Miravitlles et al. 2009a]. This study identified that the mean annual cost of drug treatment for a patient with COPD was €1218–1314 and the potential savings derived from adherence to the GOLD recommendations was on average between €198 and €293. In contrast, in our study, the drug cost from the retrospective analysis was lower (€709) than previously estimated. Moreover, when we considered the costs of treatment according to GOLD recommendations, an additional saving of €283 patient/year on average was seen.
Although the potential drug savings are of the same order, the difference in average drug cost between our study and a previous analysis [Miravitlles et al. 2009a] may be due to the fact that, in our case, 92.5% of patients had an FEV1 above 50%
Aside from the possible comparison with the GOLD guidelines, various studies in recent years have estimated the economic burden of this disease in Spain, showing that the total annual direct cost of COPD per patient varies between €1100 and €3400, with a mean of approximately €2000 [Miravitlles and Figueras, 2001; Miravitlles et al. 2003; de Miguel Díez, 2005; Masa et al. 2004; Izquierdo-Alonso and de Miguel-Díez, 2004; de Miguel Díez et al. 2008]. In our study we found the costs for patients with stage II disease to be in line with previous estimations, but the direct cost observed for patients with stage III disease was around €1900 higher than the average. This point should be taken into account when interpreting the results because of the small number of patients included with stage III disease.
When looking at the cost distribution pattern, our results confirm the well known fact that the more severe the COPD, the higher the proportion of hospital costs and the lower the proportion of drug costs. In one initial study, also performed in primary care, drug costs were responsible for 42% of the costs associated with mild COPD, 44% of those associated with moderate COPD and 40% of those associated with severe COPD [Miravitlles et al. 2003]. The study by Izquierdo-Alonso and de Miguel-Díez showed that the drug costs represented 43% of the total direct costs in patients with stage II COPD, while this figure went down to 37.6% and 28.4% for COPD stages III and IV respectively [Izquierdo-Alonso and Miguel-Díez, 2004]. These data are similar to those from the recent study by de Miguel Díez and colleagues which found drug costs to be 26% [de Miguel Díez et al. 2008]. In our study, it was observed that the weight of the drug costs over the direct costs for patients with stage II disease was similar to that found by Izquierdo-Alonso and de Miguel-Díez [Izquierdo-Alonso and de Miguel-Díez, 2004]. Part of this extra cost in GOLD II is due to the inadequate prescription of inhaled corticosteroids (Izquierdo-Alonso and Rodríguez-González Moro, 2012). However, the relative drug cost for patients with stage III disease in the nonadherent group in our study was closer to that observed for patients with stage disease in the Izquierdo-Alonso and Miguel-Díez study [Izquierdo-Alonso and de Miguel-Díez, 2004].
We also found the prescribing rate for theophylline to be lower among patients included in our study compared with other studies in Spain, possibly due to the fact that only 103 patients with FEV1 between 30% and 50% were included in the study and there were no patients with FEV1 below 30%, these patients being the main recipients of that treatment. Along the same lines, looking at the figures from the inhaled steroids in obstructive lung disease in Europe (ISOLDE) [Jones et al. 2003] and IMpacto de las agudizaciones de la EPOC (IMPAC) [Miravitlles et al. 2004] studies, a higher percentage of patients had two or more exacerbations (mean of 34.4%) than in our study (23.3%); however, these studies showed similar average costs. One of the limitations of our study is the fact that we were unable to identify exacerbations in the clinical records and had to work with an estimate. This may have led us to underestimate the frequency of exacerbations. Even so, in our study, the patients who were admitted spent an average of 11.3 days in hospital, somewhat longer than that observed in the recent study by Almagro and colleagues where, in a population with an FEV1 of 43.2% and mean age of 73.7 years, patient admissions lasted an average of 9.8 days [Almagro et al. 2010].
Apart from those discussed above, another important limitation of this study was the unavoidably subjective classification of patients with COPD on the basis of the therapeutic recommendations of the GOLD guidelines. Furthermore, while essentially specifying drug recommendations, the GOLD guidelines do not identify follow-up regimens, which would make it possible to define the ‘ideal’ use of healthcare resources in the management of COPD. This explains our decision to identify and classify the patients according to their drug use. Moreover, in comparison with the GOLD guidelines, it was observed that one of the first recommendations, namely smoking cessation as a first treatment step to prevent exacerbations in patients with COPD, was not adhered to. In our population, although the percentage of smokers in the most severe cases was low, it was found that, overall, 26.6% were still smoking. Since this study was performed in a limited geographic area, the results may not be fully extrapolated to the rest of the country.
As a result, we believe that this type of study needs to be promoted if, in the future, we are to have better information to allow decisionmakers to reliably deal with COPD. As with other chronic smoking-related diseases, the distribution of COPD basically depends on exposure to smoking and the gradual aging of the population [Soriano et al. 2010]. Initiatives such as ours, which are evaluating strategies to improve the management of patients and reduce unnecessary costs, will therefore be of crucial importance for the future control of COPD.
To conclude, our study shows that adherence to the GOLD guideline recommendations could lead to a reduction in drug use which would directly translate into financial savings for the Spanish Health Service of at least €758 per patient per year in those with stage II COPD. The new approach to treatment of COPD based on clinical phenotypes [Miravitlles et al. 2012] may help us to further improve the care of patients with this devastating disease.
Footnotes
Acknowledgements
M. Miravitlles was involved in study design, analysis and interpretation of data, and writing the manuscript. J. Galera, R. Lahoz, M. Riera and M. Lleonart developed the idea for the study, supervised it in its entirety and were involved in its design. A. Sicras provided data, analysis and a critical review of the manuscript. M. Brosa, M. Cuesta and C. Crespo were involved in study design, carried out the research and the data analysis and drafted the manuscript. All the investigators contributed to the final version of the manuscript.
Funding
The study was funded by a grant from Novartis.
Conflict of interest statement
J. Galera, R. Lahoz, M. Riera and M. Lleonart are employees of Novartis Farmacéutica SA (Spain), the company sponsoring this study. M. Brosa, M. Cuesta and C. Crespo worked in an independent consultant company and they received funds from Novartis. Marc Miravitlles has received speaker fees from Boehringer Ingelheim, Pfizer, AstraZeneca, Bayer Schering, Novartis, Talecris, Takeda-Nycomed, Merck, Sharp & Dohme and Novartis, and consulting fees from Boehringer Ingelheim, Pfizer, GSK, AstraZeneca, Bayer Schering, Novartis, Almirall, Merck, Sharp & Dohme and Takeda-Nycomed.