
Abstract
Pulmonary rehabilitation and palliative care are two important components of the integrated care of the patient with chronic respiratory disease such as chronic obstructive pulmonary disease (COPD). These two interventions are remarkably similar in many respects. Both utilize a multidisciplinary team that focuses on the specific needs of the individual patient. Care in both is goal defined and includes relief of symptoms and improvements in functional status and quality of life. Pulmonary rehabilitation is commonly given in a specific setting, such as a hospital-based outpatient setting, while palliative care is often hospital based, with its services extending into the home setting in the form of hospice. Components of pulmonary rehabilitation and palliative care should be administered as part of good medical care. Both pulmonary rehabilitation and palliative care are currently underutilized in the respiratory patient, and often provided relatively late in the patient’s clinical course. The case provided illustrates the often-overwhelming symptom burden of advanced COPD and demonstrates opportunities for the application of these twin interventions.
Introduction
Although the definition of chronic obstructive pulmonary disease (COPD) describes it as preventable and treatable, 1 the irreversible nature of this chronic disease forces us to focus on management rather than cure. Optimal care in this regard requires integration of interventions and disciplines – in essence, this involves giving the right treatment to the right patient at the right time. 2 Two important components of the integrated care model in the patient with chronic respiratory disease are pulmonary rehabilitation and palliative care. These two complex interventions are, in reality, remarkably similar in concept in many respects. This discussion will highlight these similarities.
Definitions
Pulmonary rehabilitation
The American Thoracic Society (ATS)–European Respiratory Society defines pulmonary rehabilitation as “…an evidence-based, multidisciplinary, and comprehensive intervention for patients with chronic respiratory diseases who are symptomatic and often have decreased daily life activities. Integrated into the individualized treatment of the patient, pulmonary rehabilitation is designed to reduce symptoms, optimize functional status, increase participation, and reduce health care costs through stabilizing or reversing systemic manifestations of the disease.” 3
Pulmonary rehabilitation programs involve comprehensive patient assessment, exercise training, self-management education, nutritional intervention (when indicated), and psychosocial support. 3 Pulmonary rehabilitation requires collaboration among the patient, family, and health care providers. Although pulmonary rehabilitation has no direct effect on the underlying physiologic derangements, it results in substantial improvements in dyspnea, exercise tolerance, health status, and health care utilization. 4 This effectiveness results from positive effects on primary and secondary impairments associated with the respiratory condition. Examples of these impairments include physical deconditioning and peripheral muscle weakness in COPD patients.
Palliative care
Palliative care was initially developed in response to the needs of the cancer patient, although it now is applicable to all patients with chronic severe disease who remain symptomatic and have functional limitations. It can be applied to any stage of illness: acute, chronic, or terminal. 5 The World Health Organization (WHO) defines palliative care for adults as “…an approach that improves the quality of life of patients and their families facing the problems associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, including physical, psychosocial, and spiritual issues.” 6 Hospice is a form of palliative care for patients with a life expectancy of 1 year or less who no longer wish curative efforts. Non-hospice palliative care, on the other hand, can begin even before a diagnosis is established but certainly once it seems the patient has a life-threatening illness.
The following list adapted from the WHO definition outlines the following features of the palliative care approach:
provides relief from pain and other distressing symptoms;
affirms life and regards dying as a normal process;
integrates the psychological and spiritual aspects of patient care;
offers a support system to help patients live as actively as possible until death;
offers a support system to help the family cope during the patient’s illness and with their own bereavement;
uses a team approach to address the needs of patients and their families, including bereavement counseling, if indicated;
will enhance quality of life and may also positively influence the course of illness;
is applicable early in the course of illness, in conjunction with other therapies that are intended to prolong life, such as chemotherapy or radiation therapy, and includes those investigations needed to better understand and manage distressing clinical complications.
A comparison of pulmonary rehabilitation and palliative care
Both pulmonary rehabilitation and palliative care are considered important in the management of patients with chronic respiratory disease such as COPD, as evidenced by official clinical statements by ATS and European Respiratory Society for pulmonary rehabilitation, 3 and by the ATS for palliative care. 5 Both disciplines strive to reduce distressing symptoms, improve functional status, and enhance quality of life. Additionally, both statements endorse the concept that the application of their respective interventions should be given, when needed, despite the stage of the disease, and that the interventions should be individualized based on the needs and goals of the individual patient.
Subtle differences between pulmonary rehabilitation and palliative care are suggested by the derivations of the terms: palliation comes from the past participle of the Latin root word, palliare, which means “to cloak or conceal,” while rehabilitate comes from the past participle of the Latin verb, rehabilitare, to habilitate (make fit or capable). 7 Both interventions strive to reduce symptoms and restore functional status and quality of life, but perhaps palliation focuses more on symptom relief (cloaking the distressing symptom of dyspnea), while rehabilitation focuses more on raising functional status (making fit through exercise training, etc.). This is undoubtedly an oversimplification but probably does reflect a subtle difference in their approach. Pulmonary rehabilitation is commonly given in a specific setting, such as a hospital-based outpatient setting, while palliative care transcends physical settings. 5
Table 1 provides our perspective on the similarities and differences of these two complex, patient-centered interventions. It should be noted that this very subjective analysis represents the authors’ opinions, based on their clinical experiences in the management of the patient with chronic respiratory disease. Most features listed are actually components of both disciplines, and both disciplines recommend their application based on the needs of the individual patient. In essence, this is providing the right care for the right patient at the right time, regardless of whether it is called pulmonary rehabilitation, palliative care, or just good medical therapy.
Features of pulmonary rehabilitation and palliative care
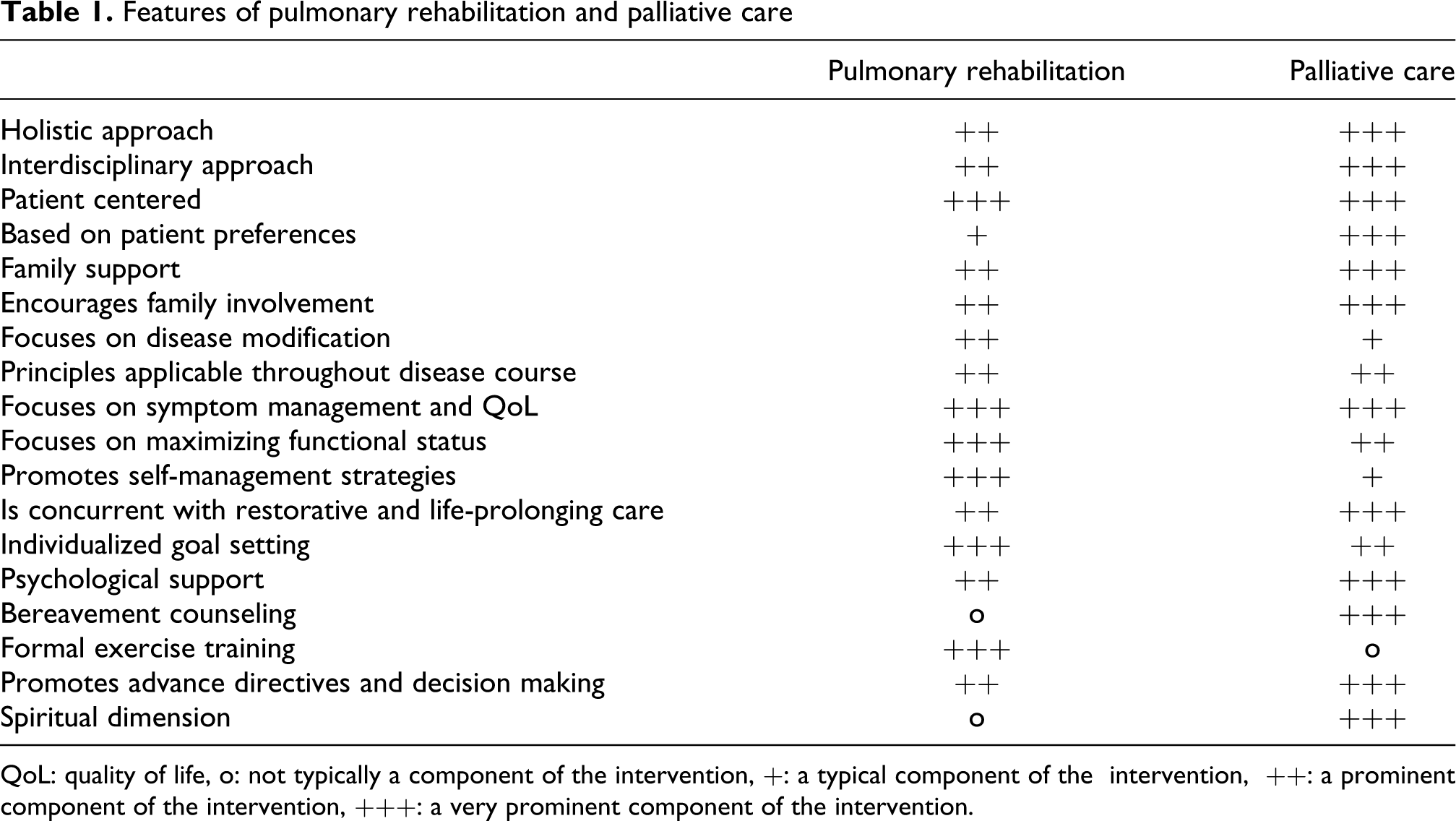
QoL: quality of life, o: not typically a component of the intervention, +: a typical component of the intervention, ++: a prominent component of the intervention, +++: a very prominent component of the intervention.
Disease burden of the patient with chronic respiratory illness
Chronic respiratory diseases such as COPD, although treatable, are incurable. Consequently, while disease-modifying and life-prolonging strategies are provided whenever possible, most interventions aim at reducing symptom burden, increasing functional status, and enhancing health related quality of life while reducing the potential side effects of the therapies. Palliation of the negative effects of the disease, its comorbidity and treatment, therefore, are paramount. The following discussion will focus on severe COPD, the most common respiratory condition leading to disability.
COPD is a leading cause of death in the developed world and has profound effects on health status, especially with advanced disease. Dyspnea and fatigue with resultant sedentarism, exercise intolerance, functional status limitations, common and important comorbid conditions, and effects of exacerbations contribute to this impairment in health status. 8 In one study of patients with advanced disease requiring supplemental oxygen therapy, 76% admitted to breathlessness ambulating at home and only 47% were able to go out. 9 In another study, 10 patients with severe COPD, as defined by an forced expiratory volume in 1 s (FEV1) <0.75 L and at least one hospitalization for respiratory failure, had more impairment in activities of daily living and physical, social, and emotional functioning than a comparison group of patients with lung cancer. The COPD group also had more anxiety and depression symptoms.
Barriers common to providing palliative care and pulmonary rehabilitation
Although pulmonary rehabilitation is effective across multiple outcome areas, its availability in the United States and worldwide remains dismal. 11 Despite the paucity of programs, principles of medical care central to pulmonary rehabilitation, such as promotion of healthy lifestyle (including regular exercise), and collaborative self-management strategies should be given as part of comprehensive medical care.
Most medical centers have established palliative care programs, but they are probably underutilized in the patient with chronic respiratory disease. Late referrals are probably due to several barriers. Patients, professional caregivers, and patients’ families often underappreciate the profound effect COPD has on the individual. Patients may not consider their limitations to be abnormal and may not realize there are treatments that might reduce their symptoms. 12 For example, a qualitative study 13 that involved interviewing patients with COPD found that they often admitted to having dyspnea severe enough to disrupt their lives, yet they accepted this as a way of life rather than as part of an illness. Thus, they were often unable to distinguish between their “disease stories” and their “life stories.” This, in part, reflects their gradual increase in symptoms and disability 14 and their gradual assumption of a sedentary lifestyle. 15 Additionally, some patients believe they caused their COPD and therefore do not deserve to have their symptoms relieved.
There is a difficulty among COPD patients and their health care providers not only in identifying the onset of the disease but also in clearly predicting its end. 13 This uncertainty also pertains to the short-term prognosis after the acute exacerbation of severe COPD; consequently palliative care services are underutilized even in this setting. 16 This uncertainty supports the argument that a specific point in time for transitioning to palliative care is meaningless and may lead to “prognostic paralysis.” 17 Rather, a progressive integration of palliative care over the course of the disease is more reasonable. 13
A case presentation: Mr LV
The following case presentation of an individual with COPD may provide some insight into the use of pulmonary rehabilitation and palliative care.
Initial pulmonary evaluation, 1996
Mr LV was first seen in pulmonary consultation in 1996. At that time, he was a 74-year-old retired engineer who had a chief complaint of a bothersome cough which had been present for several years. He had been told by his primary care physician that he had “bronchitis, asthma and a touch of emphysema.” He had smoked 1 pack of cigarettes from age 25 to 50, then cigars for 10 additional years until quitting tobacco completely at approximately age 60. The cough was productive of approximately 15 ml of mucoid sputum every morning. He also had occasional wheezing on most days and had breathlessness after walking up one flight of stairs. On “bad days,” he would get breathless walking across the room. His respiratory medications were ipratropium, three inhalations three times daily and albuterol, two inhalations as needed. He had about one exacerbation of his respiratory disease yearly. He also had a history of hypertension, treated with lisinopril, doxazosin, and amlodipine, and carotid artery disease which had been successfully treated surgically.
On examination, his blood pressure was normal and his oxygen saturation by pulse oximetry was 94% while breathing room air. His thorax appeared hyperexpanded and his breath sounds were considerably diminished throughout. He had no adventitious sounds on auscultation of his chest. The remainder of his examination was unremarkable. Spirometry was as follows: FEV1/forced vital capacity (FVC) 0.46, FEV1 1.28 L, which was 39% of predicted. There was no improvement in airflow following bronchodilator administration. This was consistent with severe COPD. His arterial blood gases showed a pH of 7.40, partial pressure of oxygen in the blood (PaO2) 61 mm Hg, and partial pressure of carbon dioxide in the blood (PaCO2) 34.5 mm Hg. His chest X-ray showed hyperinflation consistent with COPD and a computed tomography (CT) scan of the chest showed homogeneous emphysema.
After the initial consultation, the patient was given a diagnosis of severe COPD and this disease and its therapy were discussed with the patient. He brought in his advance directive, stating he did not wish cardiopulmonary resuscitation, artificial respiration, or artificial means of nutrition and hydration. Salmeterol, a long-acting beta agonist, two inhalations (90 mcg) twice daily, was added to his respiratory therapy. He then was referred to pulmonary rehabilitation.
Pulmonary rehabilitation
Pulmonary rehabilitation at that time was a 12-session outpatient program in a community hospital. The interdisciplinary team consisted of a pulmonary rehabilitation nurse, medical director, exercise physiologist, pharmacist, and respiratory therapist. His initial dyspnea assessment was Medical Research Council (MRC) 4 – breathless when dressing or undressing. His stated goal upon entering pulmonary rehabilitation was “to be able to function normally.”
Exercise training, which lasted approximately 1 h per session, included treadmill walking, stationary cycle exercise, rowing machine exercise, stair climbing, upper extremity training with elastic bands, and inspiratory resistance training. His exercise intensity and duration was initially set by the exercise physiologist, then adjusted depending on the level of perceived dyspnea. He required supplemental oxygen during the treadmill training. Twelve group education sessions were also given. His 6-min walk distance at baseline was 274 m; this increased by 31 m after the 6-week intervention. Following pulmonary rehabilitation, he was offered twice-weekly maintenance exercise training sessions at the institution, which he attended sporadically over the next several years.
Clinical course 1997–2005
Mr LV had a reduction in his exertional dyspnea following pulmonary rehabilitation that lasted several months. However, his clinical condition gradually deteriorated over the ensuing years. His dyspnea increased to the point where he was breathless at virtually all times despite bronchodilator therapy and continuous supplemental oxygen at 4 L/min flow. He experienced two–three respiratory exacerbations per year, resulting in three hospitalizations. His postbronchodilator FEV1 decreased to 0.74 L, 23% of predicted, in October 2000; no further spirometry tests were performed after that date. He developed signs of right ventricular failure in March 2004, and in August of that year he required wheelchair assistance to go to the physician’s office. Compounding this problem was his wife’s deteriorating health status. He reiterated his advance directive desire: “Pull all the plugs” when that time came. He was referred to hospice on 15 May 2005.
Hospice care 2005–2007
Mr LV was 83 at the time of his referral to hospice. He had had a sudden decrease in his performance status: he had gone from taking his wife out to lunch to having considerable difficulty walking from room to room. Although he agreed with the philosophy of hospice, he was reluctant to utilize many hospice services. For instance, he would see the nurse only every 2 weeks (the minimal requirement for hospice patients), and he would not permit other members of the team to visit. Two nurses shared his care, only rarely relying on other nurses for coverage. A kit of emergency medications was delivered to his home, and he was instructed to use sublingual morphine for dyspnea. However, he was reluctant to try the medication, saying he would wait until he was closer to death.
During his first month on hospice, he had problems with increasing peripheral edema from congestive heart failure but was too short of breath to see his cardiologist. His pulmonologist started him on furosemide. Two months after his referral to hospice, the patient’s wife was admitted to the hospital for a dislocated hip. The hospice team was concerned about his ability to manage at home alone and repeatedly offered more help (home health aide or volunteer), but he was steadfast in his refusal of these services. After not leaving the house in more than 2 months, he was able to attend a picnic for the Breathing Club (his old buddies from pulmonary rehabilitation). He was able to speak with his pulmonologist who increased his prednisone because of his increased dyspnea. He remained very dyspneic and his situation was quite tenuous. At one point, he lost power and he was without a working phone to call the oxygen company to provide backup tanks. His nurse offered to help him get a cell phone but he refused. On another occasion, the house cleaner blew a fuse when vacuuming, leaving the oxygen concentrator without power. This led to getting additional backup tanks. At the end of his first 3 months on hospice, he was readily recertified as continuing to have a prognosis of 6 months or less if his illness ran its usual course.
Over the next 3 months his prednisone dose was frequently adjusted as was his oral furosemide. He was treated with antibiotics for exacerbation of his COPD. He was using his nebulizers four times a day with inhalers at night. His dyspnea on exertion increased to the point that he was speechless for 5–10 min after the effort of walking across the room to the door to admit the hospice nurse. It took him 1–2 h to do personal care each morning since he had to pace himself very carefully and rest frequently. Once he was ready for the day, he spent most of his time sitting at a table facing an open window. Periods of hot and humid weather exacerbated his breathlessness. He was frequently urged to try low-dose morphine to help with his disabling dyspnea, but he remained reluctant. Eventually he agreed to try alprazolam 0.25 mg 3 times a day. He also was bothered about urinary frequency but was too short of breath to see his urologist. He got his annual flu vaccine. Offers of a home health aide to assist with personal care were politely declined. Both the patient and his wife wanted to be as independent as possible.
After his first 6 months on hospice, his wife dislocated her hip again, and surgery was planned. The team offered additional services, but the couple declined. His niece was able to stay with him while his wife was in the hospital. Nine months after his admission to hospice, he finally agreed to try 5 mg of sublingual morphine. He did well with this medication and came to rely on it in the morning to help with personal care. He never significantly increased his morphine dose, but eventually took a second dose on Saturday afternoons, prior to his weekly shower. Shortly afterward, his wife fell out of bed and broke her humerus and had to return to the rehabilitation facility. The hospice nurses provided emotional support for the niece and again suggested more services for Mr LV.
Over the ensuing months, he responded to his increasing disability not with as-needed medications but with a further decrease in his activities. His life became more and more constricted and he never went out. The letter carrier would pass his letters in through the window so he would not have to go to the door. The effort of microwaving the food brought by neighbors sometimes left him too tired to eat. His wife continued in and out of the hospital and rehabilitation. One day when he had been on hospice for 20 months, he developed severe respiratory distress and his wife remembered to call hospice rather than 911. The nurse found him sitting in a chair with agonal respirations and edema to the upper thighs. She gave him 5 mg of sublingual morphine but he had only transient relief. He was clearly too symptomatic to be managed at home, so he was admitted to the hospital for end-of-life care. He was brought by ambulance directly to a private room on the oncology floor, where he died within a few hours, with a family member at his side. A week later, his nurse made a bereavement visit to his wife. She subsequently became a patient of the same hospice agency.
Pulmonary rehabilitation and palliative care for Mr LV
Mr LV was first referred for his respiratory disease when he was 74 years old and had an FEV1 of 39% of predicted value. Obviously, optimal management for him would have been to begin the only significant disease-modifying strategy in COPD – smoking cessation – at a much earlier age. However, within the reality of his initial presentation, the treatment approach must focus on preventing further disease progression, reducing the frequency of exacerbations, reducing symptom burden, increasing functional status, improving quality of life, and – if possible – increasing life expectancy.
Pulmonary rehabilitation led to significant improvements in exertional dyspnea and exercise tolerance in this patient. However, the anticipated duration of benefit of a short-term pulmonary rehabilitation intervention is about 1–2 years. 18,19 Incorporating pulmonary rehabilitation principles (such as regular exercise) or offering a postrehabilitation exercise maintenance program might prolong these positive effects, although there is currently little evidence for this. 4 Mr LV did participate in maintenance exercise for several months, but his clinical course was that of gradual deterioration in symptom burden and functional status, punctuated by several exacerbations per year. Repeated courses of abbreviated pulmonary rehabilitation following exacerbations may be helpful in this situation, and there is evidence that it improves outcome in this setting. 20
As Mr LV’s disease progressed, a change in the focus of care toward the principles of palliative care was in order. It became clear that his dyspnea increased in severity and was sustained despite standard medical care (including pulmonary rehabilitation), and this resulted in substantial deterioration in functional status and quality of life. An earlier (palliative) focus on dyspnea relief, 21,22 possibly with opiates, 23 would have been beneficial in this patient with irreversible, progressive disease. The added support from the holistic and family-centered approach would also have been helpful. Certainly, the referral to hospice care eased the suffering of this patient and his family.
The timing of hospice referral in patients with advanced lung disease such as Mr LV is often challenging. In general, patients are referred to hospice when they are thought to have a life expectancy of 6 months or less if the disease runs its usual course. Decline in the patient with COPD is often signaled by multiple hospitalizations or ED visits, declining functional status (dependence in at least three of the six activities of daily living: dressing, bathing, transferring, ambulating, eating, and continence), disabling dyspnea, an FEV1 of <30%, an oxygen saturation of <88%, a pCO2 >50 mm Hg, a resting tachycardia of >100 beats/min, or uncompensated cor pulmonale. 24
Mr LV had an FEV1 of 23% predicted 5 years before his hospice referral, and he developed right ventricular failure more than 12 months before his referral. In the weeks prior to his referral, he had a marked decrease in his performance status to the point that he had trouble walking from one room to another in his house. Despite all this (and the fact that his physicians would not have been surprised if he had died at any time during his hospice care) he survived for 20 months. His unexpectedly long survival does not indicate that he had been referred too soon but highlights the difficulties of prognostication. The “surprise question” (Would I be surprised if this patient died in the next year?) has been shown to identify cancer patients with poor prognosis. 25 It is also suggested in a consensus report from the Center to Advance Palliative Care as a tool to identify newly admitted patients in need of palliative care assessment. 26
Mr LV made clear his goals of care – he wanted to live at home for as long as he could. Even prior to his hospice referral, he stated he did not want any attempts at resuscitation or intubation for respiratory distress. This decision was the result of ongoing frank discussions with his pulmonologist about the progression of his disease and the fact that interventions, including emergent noninvasive ventilation, would not result in better health. Establishing goals of care and the treatment modalities that support them is an example of primary palliative care, which should be a component of general good medical care. The necessary discussions may be the exception rather than the rule. In a study of outpatients with COPD, all end-of-life communication topics were underaddressed by clinicians and 4 of the 7 topics were addressed less than 25% of the time. Asking the question that was addressed least often (what things in life are important to you?) was correlated with a 40% increase in patient satisfaction. 27
As stated earlier, a major aim of palliative medicine is to prevent and relieve suffering. Mr LV was clearly suffering in several domains: from the sensation of breathlessness, from the resulting severe limitation of his activities, and from severe social isolation. His hospice team tried hard to treat his dyspnea, but he would only accept small amounts of morphine, resorting instead to decreasing his energy expenditure to reduce the impact of this symptom. He never used more than 10 mg of oral morphine a day, so it was not feasible to use an extended release formulation. His reluctance to take morphine was not fully understood. He simply stated that he would wait to use it until he was closer to death. Some patients fear that if they use opioid medications “early” in their illness, the medications will not be effective when they are sicker. Others fear addiction or just having narcotics in their home. Perhaps Mr LV believed that if he could limit his morphine to a small dose, it would mean that he was not close to dying. A discussion of the use of opioids for dyspnea during pulmonary rehabilitation might have helped overcome his resistance.
Although relatively easy when the patient is admitted or under the care of a hospice team, introducing opioids for dyspnea in the outpatient patient with COPD requires caution. A protocol by Rocker and colleagues 28 has been provided for this setting. This advocates starting with 1 mg of oral morphine a day, increasing over the first week to 1–2.5 mg of morphine every 4 h and then increasing by 25% weekly over the next 3–4 weeks if needed until dyspnea is acceptable. Once the patient reaches a stable dose, it is converted to a twice-daily sustained-release preparation. For patients who need episodic relief only, we use as-needed doses of sublingual oxycodone or morphine. This form has the advantage of allowing flexible dosing. For hospital patients with ongoing dyspnea, we often use a low dose of sublingual morphine (2.5 mg morphine) every 6 h with as-needed doses available every 2 h.
Pulmonary rehabilitation as a formal intervention usually ends when a patient becomes homebound. For patients too sick to visit the doctors who have cared for them for many years, the loss of contact with a trusted physician is another painful loss and patients can feel abandoned. Through the efforts of the hospice staff, Mr LV’s pulmonologist remained involved in care during his 20 months on hospice. One of the goals of palliative medicine is to provide continuity of care across care sites, and for this patient it was the pulmonologist who provided continuity.
Another goal of palliative care is to relieve the suffering and improve the quality of life of patients’ families. In the case of Mr LV, one of the primary roles of the hospice team was to support his wife and his niece. Both were viewed as collaborating members of the team.
Spiritual issues are very important at end of life. Patients want physicians to be aware of their spiritual needs and to be comfortable addressing these needs. 29 Hospice teams are required to include chaplains, who minister to the needs of all patients, including those with particular religious affiliations, those who consider themselves spiritual but not religious, and those who identify themselves as agnostic or atheist. Mr LV was unwilling to see the chaplain. A chaplain might have been able to explore the difference between curing and healing, the relationship of breath and spirit, and might have reduced the patient’s reluctance to begin opioids.
This case also illustrates a potential tension between the ethical principles of autonomy and beneficence. The hospice staff remained very respectful of Mr LV’s decision to remain at home, even when they disagreed. Accordingly, they made it possible for him to stay home alone despite his tenuous situation, recognizing that autonomy was more important to the patient than any increase in safety. Since undermining autonomy is associated with feelings of hopelessness, the maintenance of autonomy is a prominent part of dignity-conserving care. 30
Our recommendations
Both pulmonary rehabilitation and palliative care are now accepted and recommended interventions in the treatment of patients with chronic respiratory disease such as COPD. As treatment options for COPD, they complement otherwise standard medical care. Principles of pulmonary rehabilitation and palliative care, which overlap considerably, should be provided to the individual patient as part of good medical care.
In reality, pulmonologists and pulmonary rehabilitation specialists already provide primary palliative care by managing symptoms, discussing goals of care, encouraging advance directives, and referring patients for more specialized palliative care, including hospice care. Secondary palliative care is provided by physicians who specialize in hospice and palliative medicine. They work with other physicians and health care professionals to improve quality of life for patients and their families. By listening carefully to patients, they are able to help patients and families navigate the complex health care system to align treatments with what is important to them.
Communication is a key component of palliative care, and much of palliative medicine involves finding words that work. A valuable resource for pulmonologists in this regard is a series of articles published in JAMA from 2002 through 2009, Perspectives on care at the close of life. Several of these articles have direct relevance to the clinical management of respiratory patients such as Mr LV. 31 –46 These articles have been updated with recent evidence as a book and published as Care at the close of life: Evidence and experience. 47 Its 42 chapters are rich with examples of words that clinicians can utilize. These include open-ended questions (As you think about the future, what matters most to you?) and ways to introduce difficult topics (I would like to talk with you about the kind of care you would want if you became more ill. In particular, I wanted to talk with you about ….). Finally, the Center to Advance Palliative Care (www.capc.org) and the American Academy of Hospice and Palliative Medicine (www.aahpm.org) also offer many resources.
In summary, pulmonary rehabilitation and palliative care, provided as part of comprehensive, multidisciplinary interventions, should be considered earlier in the course of COPD than is typical current practice. Whether the referral is for rehabilitation or palliation (or both) will depend on individual patient needs and program availability. In general, pulmonary rehabilitation focuses on increasing exercise tolerance and functional status through exercise training and self-efficacy promotion, while palliative care focuses on relief of distressing symptoms through comprehensive interventions. Both bring in a team of professionals to optimize care and extend their therapeutic approach to include the patient’s family. Finally, there should be more integration of pulmonary rehabilitation and palliative care services for patients with chronic respiratory disease. For instance, pulmonary rehabilitation staff should consider earlier referral to palliative care, when indicated, in their patients who remain symptomatic despite comprehensive rehabilitation therapy.
Footnotes
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.