
Abstract
Background
Coronary heart disease (CHD) is a prevalent complication associated with type 2 diabetes mellitus (T2DM), and the incidence of T2DM with CHD has seen a steady rise over the preceding years.
Objective
To investigate the altered expression of LINC00893 and miR-103a-3p in T2DM and T2DM with CHD, as well as to assess their clinical significance in T2DM-CHD.
Methods
The LINC00893 and miR-103a-3p expression was detected by RT-qPCR. ROC curves were used to analyze the diagnostic significance of LINC00893 and miR-103a-3p in T2DM patients with CHD. The Kaplan-Meier curve was used to analyze the prognostic significance of LINC00893 in the occurrence of Major Adverse Cardiovascular Events (MACEs) of T2DM with CHD patients. Dual-luciferase reporter assay was used to confirm the regulatory relationship between LINC00893 and miR-103a-3p.
Result
LINC00893 and miR-103a-3p were down-regulated and up-regulated in T2DM with CHD patients, respectively and had diagnostic value in T2DM with CHD patients. In addition, patients with low levels of LINC00893 are more likely to develop MACE, and LINC00893 could regulate the expression of miR-103a-3p.
Conclusion
LINC00893 may affect disease progression in T2DM patients with CHD by regulating miR-103a-3p.
Introduction
In recent years, there has been a notable increase in the prevalence of type 2 diabetes mellitus (T2DM), which has now become the ninth leading cause of death worldwide. This disease is a multifactorial condition that arises from the interaction of genetic susceptibility, prenatal developmental factors, dietary habits, and a sedentary lifestyle. 1 The incidence of cardiovascular diseases among adult individuals with diabetes is approximately twofold to threefold higher compared to individuals without diabetes. Furthermore, cardiovascular conditions are the primary contributor to early mortality in individuals suffering from diabetes. 2 Coronary heart disease (CHD) commonly occurs as a complication in individuals with T2DM, and the incidence of T2DM with CHD has seen a steady rise over the preceding years. The disease dynamics become more intricate, fostering disease progression and elevating the challenges in treatment modalities. 3 Despite significant advancements in the management of T2DM coexisting with CHD, the identification of viable biomarkers and elucidation of relevant risk factors continues to be of substantial importance for enhancing therapeutic approaches. 4
Recently, the involvement of long non-coding RNAs (lncRNAs) in the pathogenesis of T2DM and CHD has become a subject of growing interest. For instance, a research investigation identified a total of 62 lncRNAs and 332 miRNAs that exhibited altered expression levels between patients with CHD and healthy individuals. 5 Elevated levels of LINC01018 were observed in individuals with T2DM, with high glucose levels being responsible for the upregulation of LINC01018 in islet β cells. 6 Decreased levels of serum miR-199-3p were found to be associated with the progression of T2DM-CHD and served as a biomarker for predicting unfavorable outcomes in patients with T2DM-CHD. 7
Previous studies have reported a role for LINC00893 in a variety of cancers8,9 and it has been identified as an immune biomarker for sepsis. 10 Furthermore, research has suggested that LINC00893 could serve as a biomarker for inflammation in T2DM. 11 miR-103a-3p is also associated with the progression of multiple tumors.12,13 Patients with pulmonary hypertension related to CHD exhibited a substantial increase in the expression of miR-103a-3p. 14 Furthermore, several investigations have revealed that the expression of miR-103a-3p is increased in individuals suffering from type 1 diabetes.15,16 However, the level of LINC00893 and miR-103a-3p in T2DM and their clinical value in T2DM patients with CHD have not been clarified.
The current research aimed to examine the altered expression of LINC00893 and miR-103a-3p in T2DM and T2DM with CHD, as well as to assess their significance in diagnosing T2DM-CHD. Additionally, the study investigated the correlation between the expression levels of LINC00893 and the incidence of Major Adverse Cardiovascular Events (MACEs) in patients with T2DM-CHD.
Materials and methods
Study subjects
A total of three groups of subjects were involved in this investigation. The control group included 93 healthy people who underwent routine physical examinations in Qinhuangdao Hospital of Traditional Chinese Medicine. In addition, 93 T2DM patients and 90 T2DM patients with CHD treated at Qinhuangdao Hospital of Traditional Chinese Medicine were included. Fasting venous blood was taken from all participants in the study in the morning, and serum was collected after centrifugation and stored at −80°C for reserve. All patients signed informed consent, and this study has been approved by Qinhuangdao Hospital of Traditional Chinese Medicine Ethics Committee.
Inclusion criteria:1) Participants were required to be above the age of 18. (2) The patients with T2DM conformed to the diagnostic standards outlined in the Chinese Guidelines for the Prevention and Treatment of Type 2 diabetes (2020 Edition). 17 (3) CHD patients meet the diagnostic criteria of Chinese Coronary heart disease diagnosis and treatment guidelines. 18
Exclusion criteria: (1) Patients with type 1 diabetes mellitus. (2) Patients with congenital heart disease. (3) Patients with hematologic diseases or comorbid malignancies.4) Patients who are pregnant or nursing.
The following essential patient information was documented: age, sex, body mass index (BMI), total cholesterol (TC), triglycerides (TG), low-density lipoprotein cholesterol (LDL), high-density lipoprotein cholesterol (HDL), fasting blood glucose (FBG), hemoglobin A1c (HbA1c), homoeostatic model assessment - insulin resistance (HOMA-IR), diastolic blood pressure (DBP), systolic blood pressure (SBP), and the duration of T2DM.
Clinicopathological data were gathered, and a 1-year follow-up was conducted via telephone interviews or outpatient visits to track the incidence of MACEs and to assess patient prognosis. The MACEs was defined as target lesion revascularization, nonfatal myocardial infarction, all-cause deaths, recurrent angina pectoris, and acute heart failure.
Real-time quantitative polymerase chain reaction (RT-qPCR)
The isolation of total RNA was used with TRIzol reagent (Invitrogen, Carlsbad, CA, USA) and total RNA was converted into complementary DNA (cDNA) through reverse transcription with the QuantiTect Reverse Transcription Kit (Qiagen, China). RT-qPCR was carried out employing SYBR® Premix Ex Taq™ II (Takara, Tokyo, Japan) and the Bio-Rad CFX96 TM Real-Time PCR System (Bio-Rad, Hercules, CA, USA). The quantification of RNA expression was determined using the 2−ΔΔCt method, with GAPDH serving as the endogenous control.
Cell culture and treatment
The human cardiomyocyte (AC16 cell) was sourced from Meiyan Biotechnology Co. (Shanghai, China) and was cultured in DMEM medium (Bioind, Haemek, Israel) with 10% FBS (Gibco, MD, USA) at a temperature of 37°C. To emulate the injury to cardiomyocytes observed in T2DM, these AC16 cells were exposed to a concentration of 30 mmol/L of glucose. 19
The LINC00893 overexpression vector (oe-LINC00893), negative control (oe-NC), miR-103a-3p inhibitor, miR-103a-3p mimics, and the negative controls were all obtained from GenePharma (shanghai, China). Cell transfection was conducted by Lipofectamine 3000 (Invitrogen, Carlsbad, CA, USA) for a duration of 48 h.
Dual-luciferase reporter assay
The interaction sites between LINC00893 and miR-103a-3p were predicted via starBase database. Synthetic wild-type (wt) or variant (mut) variants of LINC00893 encompassing the binding or target sequences for miR-103a-3p were cloned into the pmirGLO dual-luciferase reporter vector. Subsequently, AC16 cells were co-transfected with miR-NC, miR-103a-3p mimics, or miR-103a-3p inhibitors, along with the reporter plasmids. Thereafter, the luciferase activity was measured using the Dual-luciferase reporter assay kit (Promega).
Statistical analysis
Data were presented as the mean ± standard deviation (SD). Difference comparison was performed with t test, one-way or two-way ANOVA analysis (p < 0.05). Receiver operating characteristic (ROC) curve was used to evaluate the diagnostic value of LINC00893 in CHD patients. The sensitivity and specificity of the ROC curve were determined by the Youden index. The correlation between the expression levels of LINC00893 and miR-103a-3p was analyzed using the Pearson correlation coefficient. The correlation between the expression levels of LINC00893 or miR-103a-3p and clinical indicators was analyzed using the chi-square test. The Kaplan-Meier curve was used to analyze the relationship between LINC00893 expression and the occurrence of MACE in patients with T2DM-CHD. Schoenfeld residuals were used to test the proportional hazards assumption of the Cox model. After the proportional hazards assumption was satisfied, a multivariable Cox regression analysis was used to explore the risk factors for the occurrence of MACE in T2DM with CHD patients. In the Cox regression model, each variable has been dichotomized and encoded as 0 and 1 (Supplemental Table 1). The in vitro experimental results in this study were derived from n = 3 independent biological replicate samples. A P value of less than 0.05 was considered statistically significant.
Result
Basic characteristics of the three groups of people
Basic information statistics of subjects.
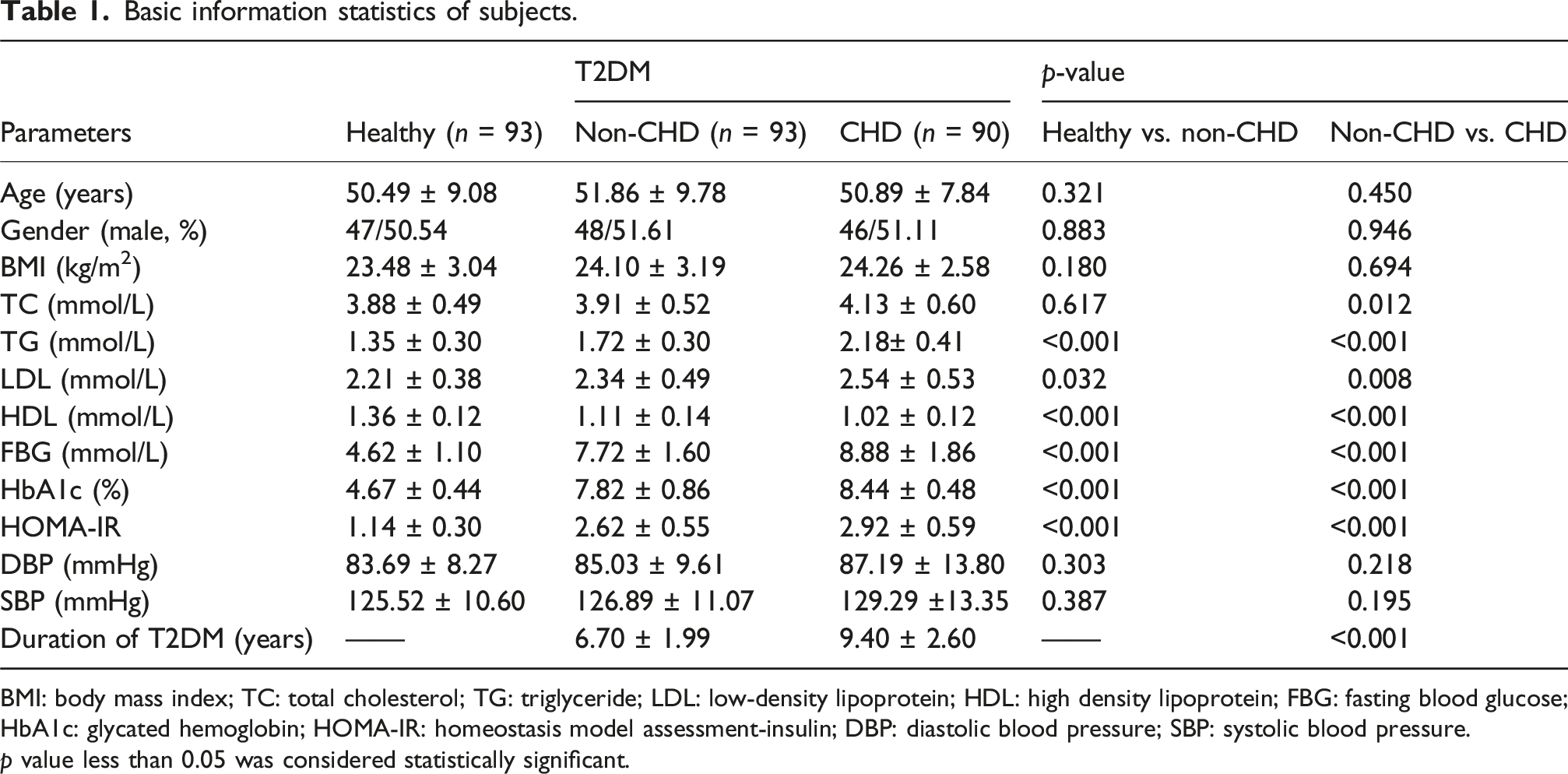
BMI: body mass index; TC: total cholesterol; TG: triglyceride; LDL: low-density lipoprotein; HDL: high density lipoprotein; FBG: fasting blood glucose; HbA1c: glycated hemoglobin; HOMA-IR: homeostasis model assessment-insulin; DBP: diastolic blood pressure; SBP: systolic blood pressure.
p value less than 0.05 was considered statistically significant.
The expression of LINC00893 and miR-103a-3p
The expression level of LINC00893 was observed to be decreased in patients suffering fromT2DM when contrasted with healthy controls (p < 0.001). Furthermore, this downregulation was more pronounced in T2DM patients with CHD (p < 0.001) (Figure 1(a)). The expression of miR-103a-3p was up-regulated in T2DM patients (p < 0.001), and patients with CHD showed a higher level of miR-103a-3p (p < 0.001) (Figure 1(b)). Furthermore, a notable negative correlation was observed between the levels of LINC00893 and miR-103a-3p expression in T2DM patients accompanied by CHD (r = −0.7387, p < 0.001) (Figure 1(c)). The expression of LINC00893 and miR-103a-3p. Expression of LINC00893 in control (n = 93), T2DM (n = 93), and T2DM-CHD (n = 90) group (a). Expression of miR-103a-3p in control (n = 93), T2DM (n = 93), and T2DM-CHD (n = 90) group (b). Correlation between expression levels of LINC00893 and miR-103a-3p (c).
Diagnostic value of LINC00893 and miR-103a-3p in T2DM with CHD patients
LINC00893 was found to distinguish between T2DM and T2DM with CHD patients, with an area under the curve (AUC) of 0.890, sensitivity of 84.4%, and specificity of 77.4% (Figure 2(a)). Moreover, miR-103a-3p demonstrated a strong diagnostic potential in T2DM patients with CHD, yielding an AUC of 0.826, a sensitivity of 76.7%, and a specificity of 75.3% (Figure 2(b)). In addition, 5-fold cross-validation was conducted. The expression levels of LINC00893 and miR-103a-3p in T2DM and T2DM-CHD patients were randomly divided into 5 equal subsets while maintaining the proportion of each category. The model was trained on 4 subsets and validated on the remaining one, repeated 5 times. The average AUC was 0.885 ± 0.036 and 0.826 ± 0.037, indicating stable performance across all partitions (Supplemental Table 1). In addition, we conducted a combined diagnostic analysis of HbA1c with the two key biomarkers, LINC00893 and miR-103a-3p, and found that the diagnostic performance was significantly improved. The AUC of the combined ROC curve reached 0.953, with a sensitivity of 92.2% and a specificity increased to 86.0% (Supplemental Figure 1). This result indicates that the combined use of HbA1c with LINC00893 and miR-103a-3p may significantly enhance the ability to identify T2DM-CHD. Diagnostic value of LINC00893 and miR-103a-3p in T2DM patients with CHD. LINC00893 (a) and miR-103a-3p (b) distinguished patients with and without CHD in T2DM patients.
LINC00893 and miR-103a-3p were associated with the development of T2DM-CHD
Correlation of LINC00893 with T2DM-CHD patients’ clinicopathological features.

BMI: body mass index; TC: total cholesterol; TG: triglyceride; LDL: low-density lipoprotein; HDL: high density lipoprotein; FBG: fasting blood glucose; HbA1c: glycated hemoglobin; HOMA-IR: homeostasis model assessment-insulin; DBP: diastolic blood pressure; SBP: systolic blood pressure.
p value less than 0.05 was considered statistically significant.
Correlation of miR-103a-3p with T2DM-CHD patients’ clinicopathological features.

BMI: body mass index; TC: total cholesterol; TG: triglyceride; LDL: low-density lipoprotein; HDL: high density lipoprotein; FBG: fasting blood glucose; HbA1c: glycated hemoglobin; HOMA-IR: homeostasis model assessment-insulin; DBP: diastolic blood pressure; SBP: systolic blood pressure.
p value less than 0.05 was considered statistically significant.
Significance of LINC00893 in predicting the occurrence of MACEs in T2DM-CHD
Among the 90 patients with T2DM complicated with CHD in this study, a total of 23 cases experienced MACEs. The average follow-up was once every 2 months, and the follow-up period was up to 12 months. During these 12 months, no patients were lost to follow-up. The findings indicated that individuals exhibiting low expression of LINC00893 were more susceptible to experiencing MACEs compared to those displaying high expression levels (Figure 3(a), Log Rank p = 0.011). Furthermore, after checking the proportional hazards assumption (Supplemental Table 2), a multivariable Cox regression analysis was conducted. Variables with clear clinical importance, including age, gender, HbA1c, and the two biomarkers LINC00893 and miR-103a-3p that we focused on were included in this model. The chi-square value (−2 times the log-likelihood ratio) of the Cox regression model was 29.43, with p < 0.001, indicating that the model was statistically significant. The Akaike Information Criterion (AIC) for this Cox proportional hazards model was 154.20. Cox regression analysis revealed that LINC00893 (IQR-HR = 0.010, 95%CI = 0.00-0.81, p = 0.01) and miR-103a-3p (IQR-HR = 1.906, 95%CI = 1.3-2.8, p = 0.035) were risk factors for the incidence of MACEs in patients suffering from T2DM with CHD (Figure 3(b)). In addition, we also constructed a multivariable Cox regression model including the 15 variables. In this model, LINC00893 and miR-103a-3p remained independent influencing factors for patient prognosis (Supplemental Figure 2). Hazard ratios from the multivariable Cox regression models are presented as interquartile hazard ratios for continuous variables, representing the change in hazard for an IQR increase in the predictor. Results are visualized in a forest plot with a logarithmically scaled X-axis. Significance of LINC00893 in predicting the occurrence of MACEs in T2DM-CHD patients. The value of LINC00893 expression in predicting the occurrence of MACEs in T2DM patients with CHD (a). Cox analysis of risk factors for MACEs in T2DM patients with CHD (b).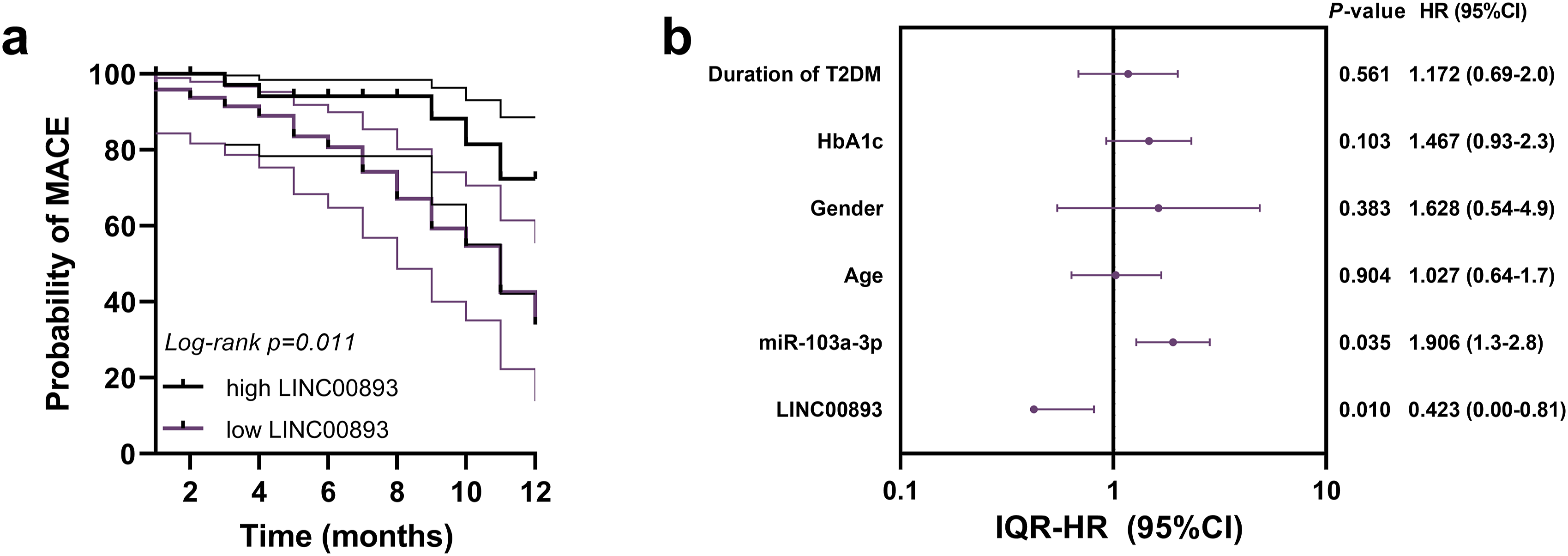
LINC00893 regulated the expression of miR-103a-3p
Overexpression of miR-103a-3p significantly inhibited luciferase activity of LINC00893 (p = 0.004), while inhibition of miR-103a-3p showed the opposite effect (p = 0.007) (Figure 4(a)). Moreover, the level of LINC00893 was down-regulated in cardiomyocytes treated with high glucose (p < 0.001), while the expression of miR-103a-3p was up-regulated (p < 0.001). The level of miR-103a-3p was down-regulated after overexpression of LINC00893 (p < 0.001), and this trend was reversed after miR-103a-3p mimic transfection (p = 0.006) (Figure 4(b) and (c)). LINC00893 regulated the expression of miR-103a-3p. Dual luciferase reporter gene assay verified the binding relationship between LINC00893 and miR-103a-3p (a). miR-103a-3p mimic showed no effect on the expression of LINC00893, but LINC00893 could modulate the expression of miR-103a-3p (b–c).
Discussion
T2DM is associated with significant microvascular complications, which are a leading cause of morbidity and mortality in individuals with diabetes. The primary contributors to diabetes-related deaths are macrovascular complications such as CHD and stroke. For years, diabetes has been identified as a significant risk factor for cardiovascular diseases (CVDs). 4 Individuals with T2DM experience a higher frequency of CHD than individuals without diabetes. 20
There is increasing evidence that lncRNAs and miRNAs are involved in the pathogenesis of human diabetes and cardiovascular diseases.21,22 In our investigation, we explored the participation of LINC00893 and miR-103a-3p in T2DM and T2DM-CHD patients. Our experimental results also validate previous related studies.11,14 It was discovered that the levels of LINC00893 and miR-103a-3p were altered in the individuals with T2DM, and there is a distinct abnormal expression in CHD patients that differentiates them from those with only T2DM, indicating its possible role in forecasting the incidence of CHD among individuals with T2DM. Moreover, the research revealed a significant relationship between the expression of LINC00893 and miR-103a-3p in T2DM patients with CHD and a list of clinical indicators. Increased levels of non-conventional lipid parameters were found to be significantly linked with prediabetes and T2DM in patients with CHD, particularly the ratio of TG to HDL (TG/HDL). A high TG/HDL ratio emerged as a potent risk factor, exhibiting a strong association with the incidence of prediabetes and T2DM. 23 Alterations in lipid metabolism among individuals with T2DM result in irregularities within blood lipids, which heighten the likelihood of suffering from CHD. 7 HbA1c serves as a distinct predictor of MACEs in individuals suffering from T2DM with CHD. 24 Levels of HbA1c are significantly correlated with the occurrence of carotid artery plaques, as well as plaque echogenicity in CHD patients. This suggests that varying levels of HbA1c could serve as a marker for the presence of carotid artery plaques. 25 The duration of T2DM is a crucial risk factor for CHD in patients with T2DM. 26 Therefore, the expression of LINC00893 and miR-103a-3p may be related to the development of T2DM-CHD patients.
The occurrence of MACEs is the main manifestation of an unfavorable clinical course in individuals with CHD. 7 In this study, the incidence of MACE in T2DM with CHD patients was recorded and its relationship with the expression of LINC00893 was analyzed. Previous research has identified several lncRNAs that serve as predictors for MACE in CHD. For instance, lncRNA ANRIL exhibits a considerable predictive role for MACEs in patients with CHD. 27 The level of lncRNA THRIL effectively forecasted an increased risk of CHD. Additionally, it was linked to an enhanced risk of MACEs in CHD patients. 28 In this study, a marked decrease in serum LINC00893 levels was found to be significantly correlated with a higher incidence of MACEs. LINC00893 was identified as a determinant of MACEs risk in patients with T2DM with CHD. Nevertheless, due to the individuation of patient treatments, the prognosis for individuals also differs from one patient to another. Consequently, the prognostic significance of LINC00893 should be explored within the context of diverse therapeutic approaches. In addition, the potential mechanism of LINC00893 action in T2DM combined with CHD needs to be further investigated.
Previous studies have reported that LINC00893 could regulate the expression of miR-3173-5p and affect the progression of prostate cancer. 8 LINC00893 affects colon cancer progression by binding to miR-146b-3p. 29 Although the regulatory relationship between LINC00893 and miR-103a-3p has not been explored, we found the binding sites of the two through the online database. Moreover, we confirmed the regulatory relationship between LINC00893 and miR-103a-3p in actual experiments. Studies have found that the level of lncRNA FA2H-2 in CHD patients is decreased, which is negatively correlated with inflammation-related factors. 30 LncRNA PVT1 inhibits apoptosis in coronary endothelial cells. 31 LncRNA UCA1 enhances the repair function of hyperglycemic smooth muscle cells. 32 This suggests that lncRNAs may affect the progression of T2DM and CHD through multiple mechanisms. As for the mechanism of LINC00893 affecting T2DM with CHD, more in vitro experiments are needed to be proven.
In summary, this study explored the expression and diagnostic significance of LINC00893and miR-103a-3p in T2DM patients with CHD and analyzed the predictive value of LINC00893 in the occurrence of MACEs in T2DM-CHD patients. This study also has some limitations, for example, the sample size is not large enough, resulting in a relatively small number of events. This does not meet the minimum event number requirement for decision curve analysis. Although we provided stable and reliable estimates by constructing a parsimonious model, the exploratory analysis retained models with more variables, which may carry the risk of overfitting. This is due to our relatively small sample size and the low ratio of the number of events to the number of variables. Therefore, the conclusions need to be further validated in prospective studies or larger independent cohorts. In the future, multi-center studies with a larger sample size should be conducted, and decision curve analysis should be performed to evaluate the utility of the proposed biomarkers in practice and provide important insights for clinical applicability. In addition, more experiments are needed to explore the regulatory mechanisms of LINC00893 and miR-103a-3p.
Supplemental Material
Supplemental material - Clinical significance of LINC00893 and miR-103a-3p in type 2 diabetes mellitus patients with coronary heart disease
Supplemental material for Clinical significance of LINC00893 and miR-103a-3p in type 2 diabetes mellitus patients with coronary heart disease by Huansong Fang, Xiaoli Han, Jiaoding Tian and Donghua Liang in Diabetes & Vascular Disease Research
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.