
Abstract
Background
Arterial stiffness is associated with cardiovascular events. Matrix metalloproteases (MMPs), their tissue inhibitors (TIMPs) and galectin-3 are involved in the pathogenesis of end organ damage. This study aimed to evaluate the contribution of arterial stiffness, MMPs, TIMPs and galectin-3 with the current vascular status in type 2 diabetes mellitus (T2DM).
Methods
74 patients with T2DM, 36 with coronary heart disease (CHD) (T2DM + CHD) and 38 without CHD (T2DM − CHD) were included. Aortic pulse wave velocity (PWVao), aortic and brachial augmentation indices (AIx aortic and AIx brachial) and central-aortic blood pressure values were determined by non-invasive arteriography. MMPs, TIMPs and galectin-3 plasma concentrations were analysed by ELISA.
Results
Patients with T2DM and CHD presented with significantly increased arterial stiffness determined as AIx and significantly elevated values for TIMP-4 and galectin-3. Heterogeneous peripheral vascular status regardless of the CHD status was observed, and increasing severity of CHD was associated with an increased arterial stiffness. TIMP-4 correlated significantly with an elevated PWVao in the whole cohort independently from CHD status.
Conclusion
Determination of arterial stiffness is an effective and, compared to laboratory markers, more reliable method for determining the peripheral vascular situation in patients with T2DM, but it does not clearly depict coronary situation.
Key messages
• In patients with T2DM, peripheral vascular status does not necessarily correspond to the coronary status. • In T2DM, TIMP-4 is significantly elevated in patients with atherosclerotic disease. • In T2DM, TIMP-4 levels are in correlation to peripheral artery status irrespective of CHD status.
Introduction
Patients with diabetes mellitus (DM) are at high risk of developing micro- and macrovascular complications. 1 The risk of developing cardiovascular diseases (CVDs) is increased in patients with type 2 diabetes mellitus (T2DM) even after consideration of common cardiovascular risk factors (CVRFs), nominating DM as CVRF. 2 Patients with T2DM without previous myocardial infarction (MI) have the same risk of MI as non-diabetics with previous MI. The presence of both risk factors, T2DM and past MI, is associated with an even higher incidence of re-MI. 3 Despite this well-known fact, DM is not routinely analysed in many patients with coronary heart disease (CHD), but it appears as a common comorbidity after screening. 4
As a result of biological ageing and arteriosclerosis, arterial stiffness is associated with the risk of cardiovascular events, which has been shown in several studies. 5 The European Society of Hypertension (ESH) and the European Society of Cardiology (ESC) have recommended the measurement of the aortic pulse wave velocity (PWVao) as a marker of end organ damage since 2007. 6 In patients with DM, PWVao is advocated due to its additive predictive value for cardiovascular risk stratification. 6
In addition to common CVRFs, the arteriosclerotic markers matrix metalloproteases (MMPs) and their tissue inhibitors (TIMPs), as well as the fibrosis marker galectin-3 are involved in the pathogenesis of arterial stiffness.5,7,8
The arterial stiffness can be determined by non-invasive arteriography which is based on an oscillometric measurement method. 9 The PWVao is a direct measure and the gold standard for measuring arterial stiffness. 10 The indirect parameters of arterial stiffness include the aortic and brachial augmentation indices (AIx aortic and AIx brachial), as well as the central systolic blood pressure near the aortic root (SBPao) and the aortic pulse pressure (PPao), both as central-aortic blood pressure values. They belong to the pulse wave reflection quantifying as well as to the central hemodynamic indices. 11
MMPs are zinc-containing, proteolytic metalloenzymes that are involved in the remodelling of extracellular macromolecules such as collagen and elastin. 12 Specific to MMP-2 and MMP-9 (gelatinase A and B) are the degradation of type IV collagen, vascular remodelling, angiogenesis and involvement in the inflammatory process and rupture of atherosclerotic plaques. 13 The family of TIMPs comprises four members regulating MMP-activity.
Galectins, proteins of the lectin family, specifically bind ß-galactosidases by means of the C-terminal carbohydrate recognition domain (CRD).14,15 A total of 14 galectins have been identified in mammals. In addition to the CRD, galectin-3 is characterised by an atypical N-terminal domain (ND). 15 It is localised both intracellular in the nucleus and in the cytoplasm and extracellular on the cell surface or in the ECM. Therefore, it is involved in various biological processes such as immune reactions, carcinomas, metabolic disorders including DM and inflammation through to fibrogenesis.15-17 Galectin-3 is present to an increased extent in atherosclerotic plaques and mediates aldosterone-induced vascular fibrosis.18,19
According to the current state of knowledge, the data that can prove the relationship between arterial stiffness, measured by arteriography, and MMPs, TIMPs and galectin-3 is limited in patients with T2DM. Therefore, the primary aim was to look for a correlation between the arteriography parameters and the coronary status in these patients to access the correlation between peripheral vascular and coronary status. Secondary, we aimed to analyse the correlation of laboratory markers with the peripheral vascular status in patients with T2DM.
Methods
Study population
Between July 2012 and April 2013, a total of 74 subjects with T2DM were recruited of whom 36 had additionally CHD based on clinical criteria. These patients were in inpatient or outpatient treatment at the Diabetes Centre of the HDZ NRW, Bad Oeynhausen, Germany. Two clinical groups were built, 38 patients with T2DM and without CHD (T2DM − CHD) and 36 patients with T2DM and with CHD (T2DM + CHD).
Participants with a body mass index (BMI) <40.0 kg/m2, HbA1c <10.5% and blood pressure (with and without pharmacological therapy) <160/100 mmHg were eligible. Participants with peripheral arterial disease (PAD), depression, tumour disease and active nicotine abuse were excluded from the study.
All subjects gave written informed consent for the study after extensive verbal and written information. The ethics committee of the Medical Faculty of the Ruhr-Universität Bochum, based in Bad Oeynhausen, approved the study protocol according to the ethics application (Reg. No. 33/2012), and the study was carried out in accordance with the Helsinki principles.
Study design
This study is a cross-sectional study. Additional blood samples were taken as part of a regular blood sampling and analysed for relevant markers. Patient data such as age and gender, medical history, medication information and blood parameters (HbA1c, LDL-cholesterol, HDL-cholesterol, adiponectin, proinsulin, BNP and CRP) were recorded.
The non-invasive vascular examination was performed using the TensioClinic Arteriograph® (TenisoMed, Budapest, Hungary).
Commercially available enzyme-linked immunosorbent assays (ELISAs) were used for the selective determination of the concentration of the markers MMP-2, MMP-9, TIMP-1, TIMP-2, TIMP-4 (R&D Systems, Abingdon, UK) and galectin-3 (BGM, Inc., Waltham, MA, USA). These were carried out in accordance with the manufacturer’s instructions.
Determination of arterial stiffness using arteriography
The non-invasive arteriography measurement is an oscillometric measurement method that is comparable to conventional blood pressure measurement in terms of scope and duration. The measurement is based on plethysmography and registers pulsatile pressure fluctuations in the arterial vascular system of the upper arm. Fluctuations in the pulsatile pressure in the artery below the inflated blood pressure cuff induce periodic pressure fluctuations (oscillations) in the inflated cuff as an indirect measure of the pulsatile pressure fluctuations in the artery below the cuff. After the upper arm cuff has been inflated, the individual parameters are analysed via the cuff. The registered signals reflect the arterial and aortic circulation system. All arteriography measurements were carried out with the TensioClinic Arteriograph® (TenisoMed, Budapest, Hungary) according to the manufacturer’s instructions.
The blood pressure cuff acts as a sensor through which the arteriograph can oscillometrically measure the current blood pressure. The cuff is then inflated to a systolic blood pressure which is 35 mmHg higher than the initial value measured. The pressure fluctuations in the brachial artery are now detected by the cuff. This information is recorded and analysed as pulse waves.
The arteriograph calculates the pulse wave velocity (PWV) from the time difference between the start of the initial wave and the start of the second reflected wave, in relation to the aortic length, which is determined by the distance between the jugulum and the symphysis. 9
To determine the augmentation index (AIx), the arteriograph relates the difference in amplitude between the reflected (P2) and initial (P1) waves to the pulse pressure (PP). The basis is the formula AIx = [(P2−P1)/PP] x 100. 9
The aortic parameters of arterial stiffness, that is, the AIx aortal, the central-aortic blood pressure values and the PWVao are calculated on the basis of a linear relationship to the brachial recorded parameters. 20
The measurement results of the PWVao (Figure S1) and the AIx brachial (Figure S2) are classified in four value ranges according to the consentual publication of the Arterial Stiffness’ Collaboration. 21 For the sake of simplicity, the evaluation of the measurement results of the PWVao was parametrically combined to “normal” and “elevated.”
Statistical analysis
Data were analysed using GraphPad Prism 8.3.0 (GraphPad Software) and SPSS Vers.24 (IBM Statistics). All measured values were shown as mean value (MV) and standard deviation (±SD). The non-parametric two-sample t-test with Mann–Whitney post-test was used to analyse the MV of the two cohorts examined. Multivariate analysis taking patient specific parameters (age, diastolic blood pressure (DBP), diabetes duration, LDL-cholesterol and BNP for comparison of T2DM − CHD versus T2DM + CHD; age, DBP, diabetes duration, BMI, LDL-cholesterol, HDL-cholesterol and BNP for comparison after grouping for PWVao result) into account was performed to analyse differences between the two groups. In the case of a three-group comparison, a Kruskal–Wallis test for independent samples was carried out if there was no normal distribution of all tested groups. If there was a significant difference, Dunn’s post hoc test was carried out to determine significant differences between the groups. Pearson correlations were calculated on one side if the effect was known and on both sides if the outcome was open. A p-value <0.05 was regarded as statistically significant.
Results
Evaluation according to coronary heart disease-status
Demographic and clinical characteristics of the patient population according to the coronary heart disease-status.
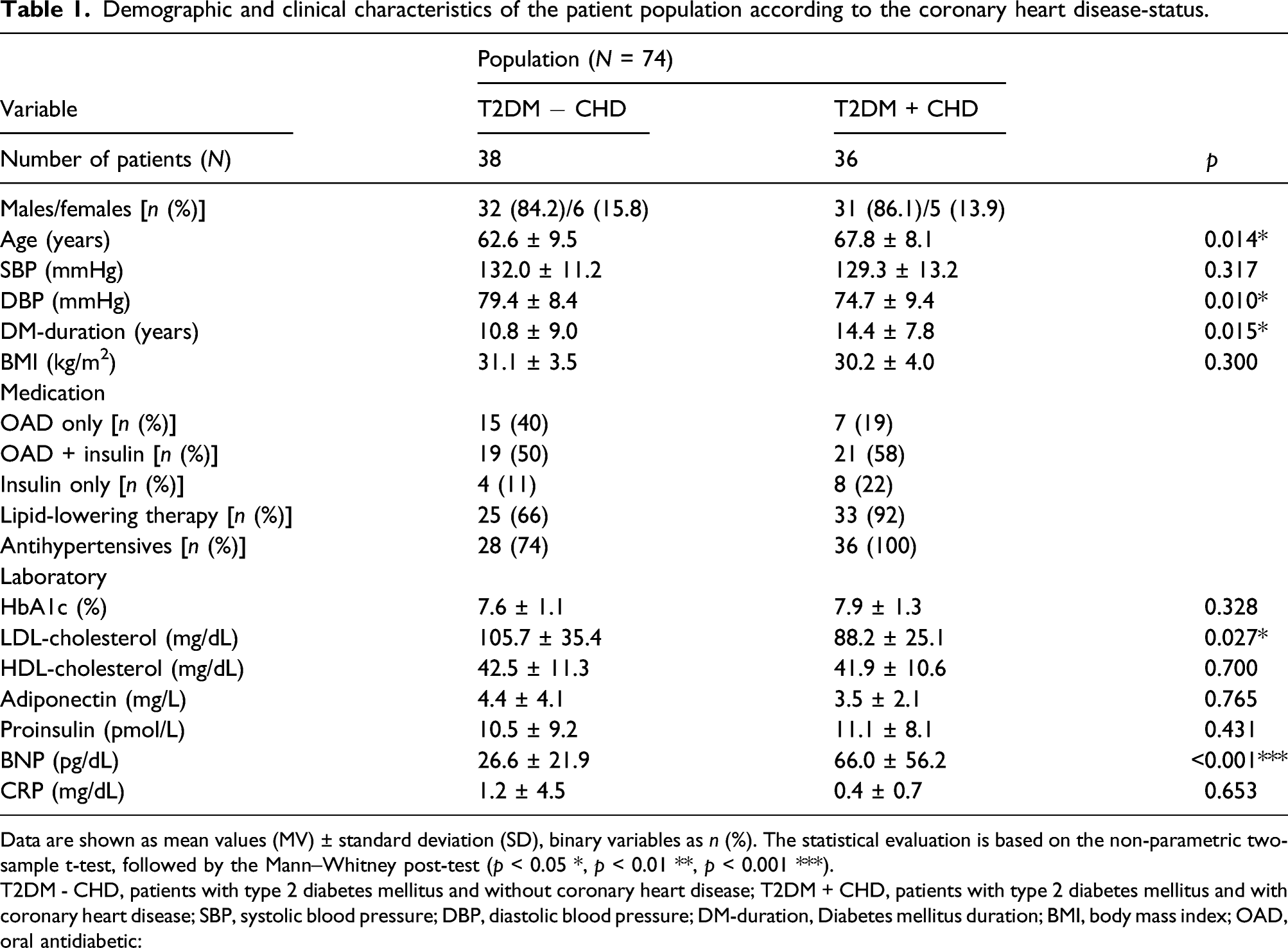
Data are shown as mean values (MV) ± standard deviation (SD), binary variables as n (%). The statistical evaluation is based on the non-parametric two-sample t-test, followed by the Mann–Whitney post-test (p < 0.05 *, p < 0.01 **, p < 0.001 ***).
T2DM - CHD, patients with type 2 diabetes mellitus and without coronary heart disease; T2DM + CHD, patients with type 2 diabetes mellitus and with coronary heart disease; SBP, systolic blood pressure; DBP, diastolic blood pressure; DM-duration, Diabetes mellitus duration; BMI, body mass index; OAD, oral antidiabetic:
Additional exploratory parameters collected for the patient population according to the coronary heart disease-status.
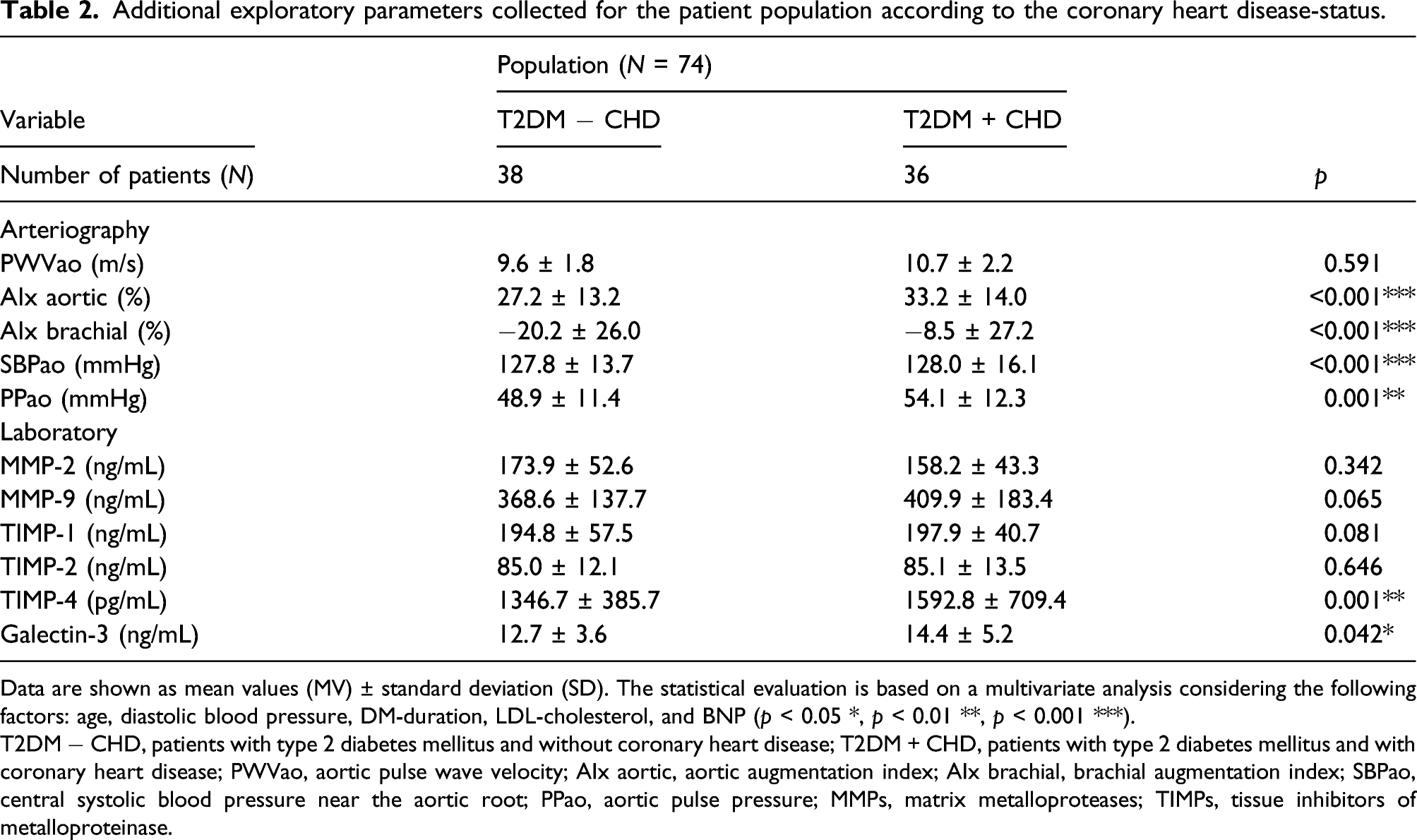
Data are shown as mean values (MV) ± standard deviation (SD). The statistical evaluation is based on a multivariate analysis considering the following factors: age, diastolic blood pressure, DM-duration, LDL-cholesterol, and BNP (p < 0.05 *, p < 0.01 **, p < 0.001 ***).
T2DM − CHD, patients with type 2 diabetes mellitus and without coronary heart disease; T2DM + CHD, patients with type 2 diabetes mellitus and with coronary heart disease; PWVao, aortic pulse wave velocity; AIx aortic, aortic augmentation index; AIx brachial, brachial augmentation index; SBPao, central systolic blood pressure near the aortic root; PPao, aortic pulse pressure; MMPs, matrix metalloproteases; TIMPs, tissue inhibitors of metalloproteinase.
No statistically significant difference was shown for PWVao between both groups although patients with T2DM presented with slightly elevated but still normal PWVao of 9.6 ± 1.8 m/s in contrast to the patients with additional CHD, who had an elevated PWVao of 10.7 ± 2.2 m/s (p = ns) (Table 2).
Severity of CHD and the parameters of arteriography.
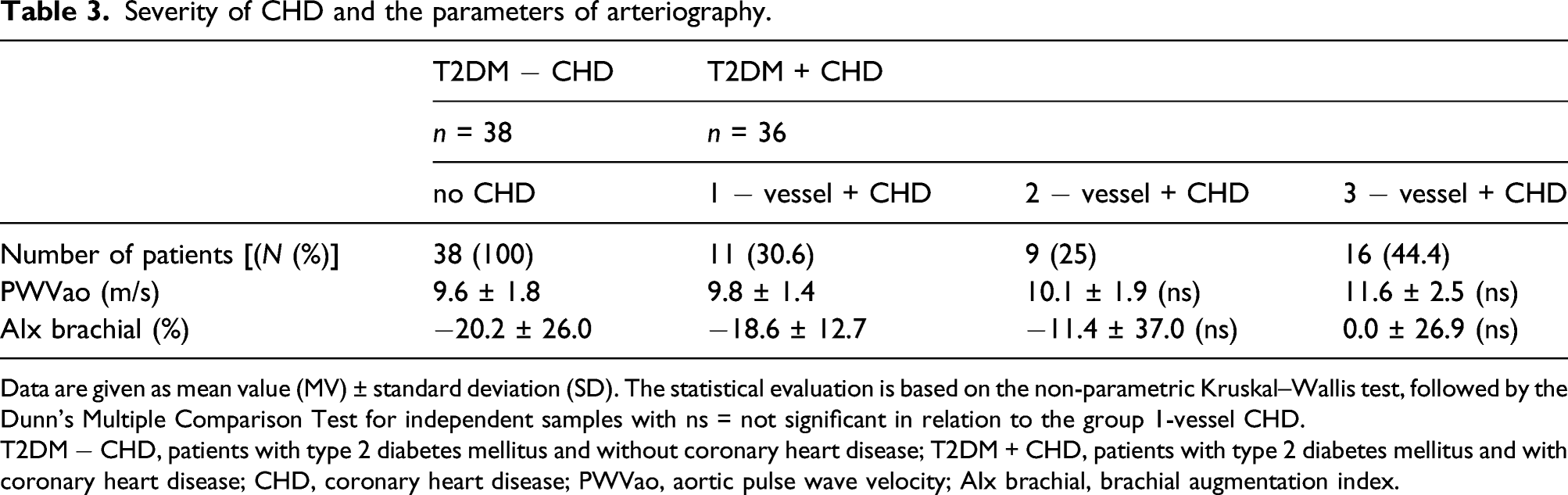
Data are given as mean value (MV) ± standard deviation (SD). The statistical evaluation is based on the non-parametric Kruskal–Wallis test, followed by the Dunn’s Multiple Comparison Test for independent samples with ns = not significant in relation to the group 1-vessel CHD.
T2DM − CHD, patients with type 2 diabetes mellitus and without coronary heart disease; T2DM + CHD, patients with type 2 diabetes mellitus and with coronary heart disease; CHD, coronary heart disease; PWVao, aortic pulse wave velocity; AIx brachial, brachial augmentation index.
Evaluation according to aortic pulse wave velocity-status
Demographic and clinical characteristics of the patient population according to the aortic pulse wave velocity-status.
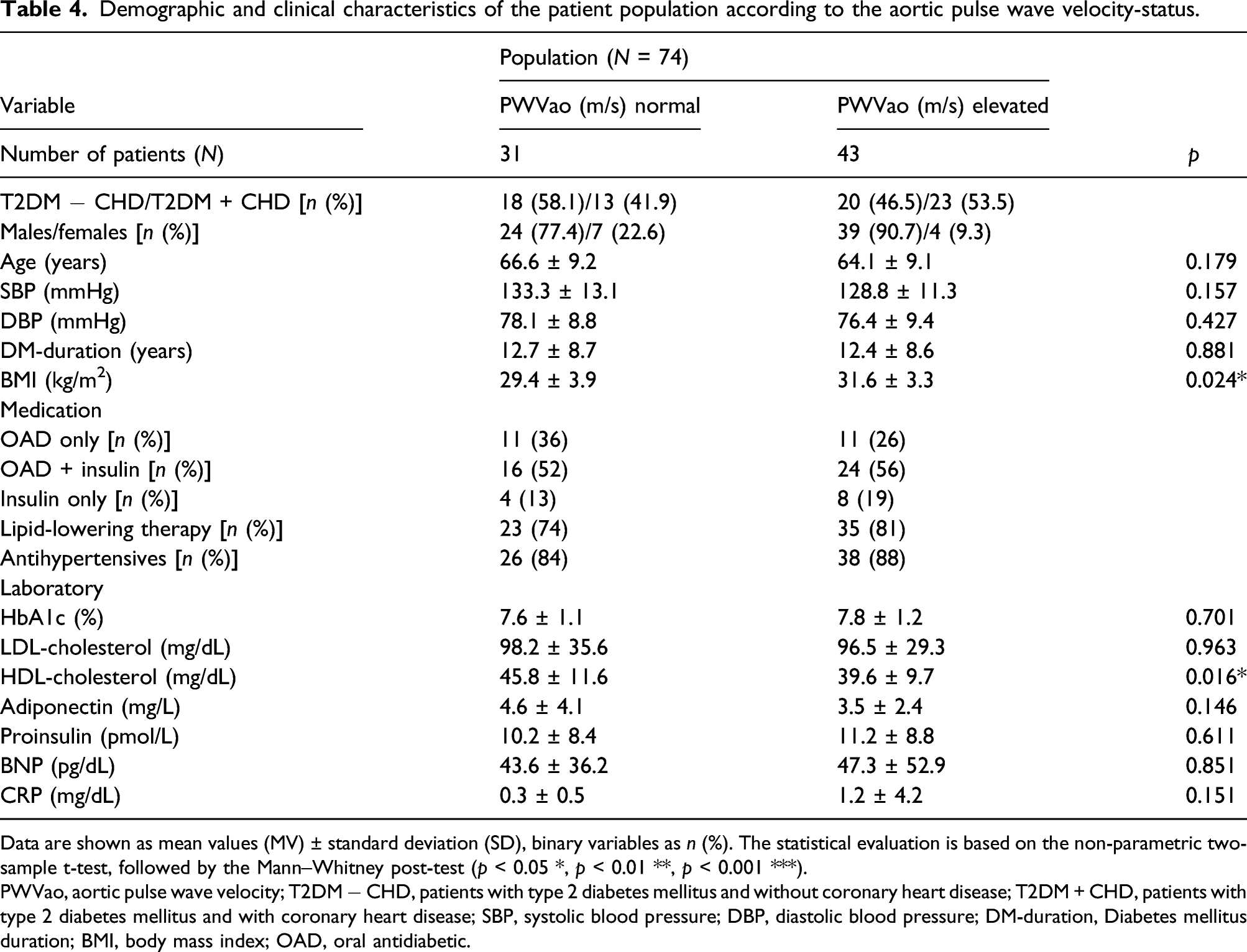
Data are shown as mean values (MV) ± standard deviation (SD), binary variables as n (%). The statistical evaluation is based on the non-parametric two-sample t-test, followed by the Mann–Whitney post-test (p < 0.05 *, p < 0.01 **, p < 0.001 ***).
PWVao, aortic pulse wave velocity; T2DM − CHD, patients with type 2 diabetes mellitus and without coronary heart disease; T2DM + CHD, patients with type 2 diabetes mellitus and with coronary heart disease; SBP, systolic blood pressure; DBP, diastolic blood pressure; DM-duration, Diabetes mellitus duration; BMI, body mass index; OAD, oral antidiabetic.
Additional exploratory parameters collected for the patient population according to the aortic pulse wave velocity-status.
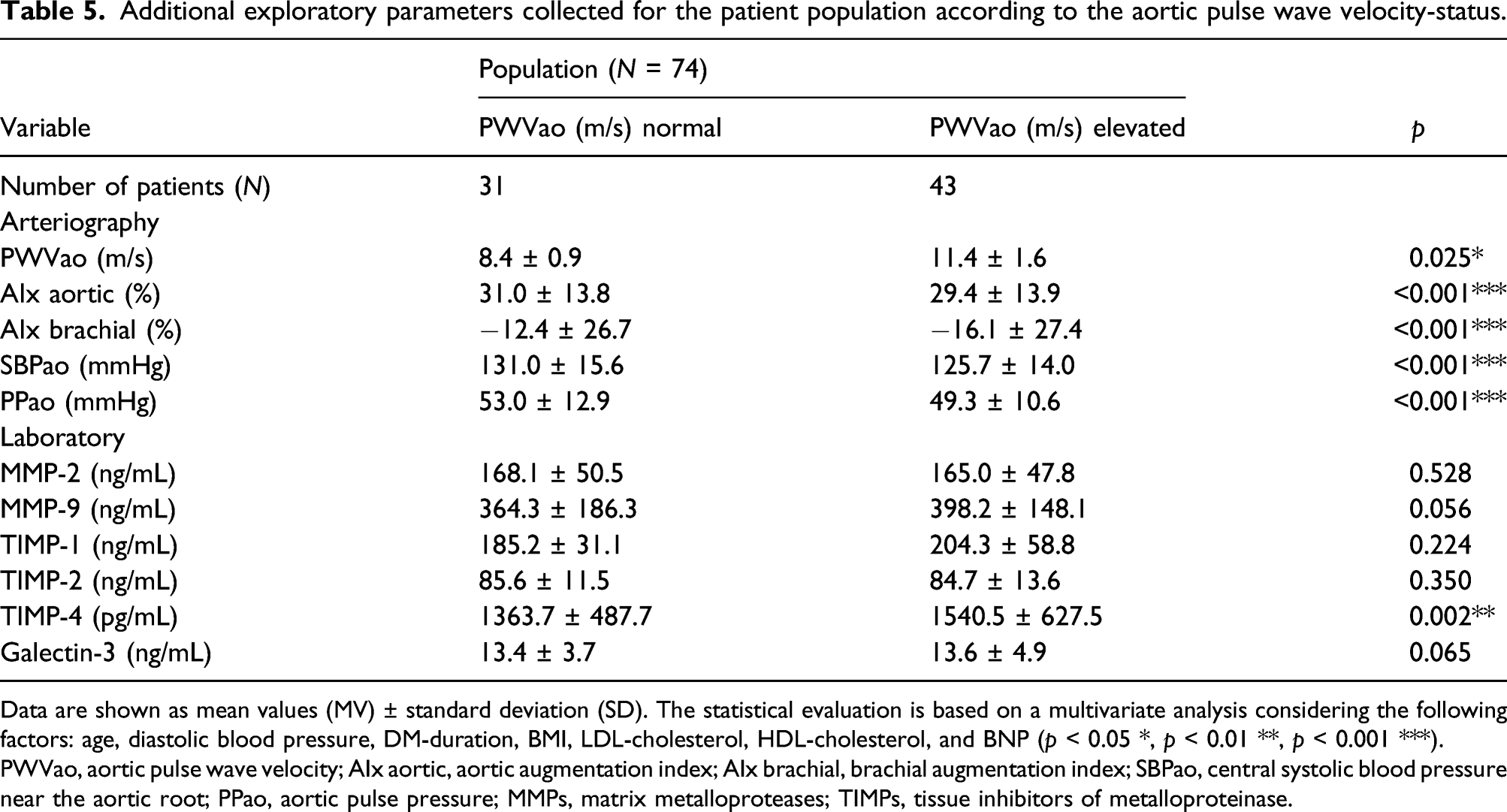
Data are shown as mean values (MV) ± standard deviation (SD). The statistical evaluation is based on a multivariate analysis considering the following factors: age, diastolic blood pressure, DM-duration, BMI, LDL-cholesterol, HDL-cholesterol, and BNP (p < 0.05 *, p < 0.01 **, p < 0.001 ***).
PWVao, aortic pulse wave velocity; AIx aortic, aortic augmentation index; AIx brachial, brachial augmentation index; SBPao, central systolic blood pressure near the aortic root; PPao, aortic pulse pressure; MMPs, matrix metalloproteases; TIMPs, tissue inhibitors of metalloproteinase.
Multivariate analysis considering age, DBP, diabetes duration, BMI, LDL-cholesterol, HDL-cholesterol and BNP revealed that the laboratory marker TIMP-4 (1363.7 ± 487.7 pg/mL vs. 1540.5 ± 627.5 pg/mL; p < 0.01) was increased in patients with elevated PWVao, and for galectin-3 (13.4 ± 3.7 ng/mL vs. 13.6 ± 4.9 ng/mL; p = 0.065) and MMP-9 (364.3 ± 186.3 ng/mL vs. 398.2 ± 148.1 ng/mL; p = 0.056), a trend to increased values was detectable. MMP-2 and TIMP-1 and -2 were comparable in patients with normal and elevated PWVao (Table 5). Depending on a normal PWVao, correlations with all indirect parameters of arteriography were shown for TIMP-4: TIMP-4 correlated with AIx aortic (r = 0.47; p < 0.01), AIx brachial (r = 0.44; p < 0.05), SBPao (r = 0.48; p < 0.01) and PPao (r = 0.59; p < 0.001). In the population with elevated PWVao, a positive association of PWVao with both TIMP-4 (r = 0.32; p < 0.05) and galectin-3 (r = 0.33; p < 0.05) was shown.
Discussion
Patients with T2DM per se are at increased risk for CVDs. Presence of CHD multiplies the risk for future vascular events. 3 Assuming that the peripheral vascular situation reflects the coronary situation, as previously shown in the Clopidogrel for High Atherothrombotic Risk and Ischemic Stabilization, Management, and Avoidance (CHARISMA) trial, the aim of the study was to investigate arteriosclerotic status of patients with T2DM with and without CHD by arteriography and biochemical risk markers. 22 In any case, following the CHARISMA result, we would have expected that the presence of CHD would lead to higher arterial stiffness and increased marker concentrations of MMPs, TIMPs and galectin-3 in terms of generalised atherosclerosis. Therefore, the correlation between the arteriography parameters and the coronary status in patients with T2DM was primarily analysed. Secondly and exploratively, the correlation between the arteriography parameters and MMPs, TIMPs and galectin-3 was examined independently from CHD status.
However, this study showed that patients with additional CHD had a pathologically increased arterial stiffness in terms of AIx but not PWVao as measured by arteriography supporting the primary assumption, but it also became clear that only selective laboratory markers (TIMP-4 and galectin-3) were associated with the coronary status in patients with T2DM. Secondly, this study revealed that patients with T2DM independently from CHD already present with atherosclerosis, underlying the fact that diabetes mellitus per se independent from metabolic control is a driver of the disease. In this study, patients with vascular disease – either on the peripheral or the coronary level – are present in every group following our analysis scheme. Thus, peripheral does not depict coronary status and vice versa in T2DM as it was shown previously for the patient population of the CHARISMA-trial leading to the assumption that atherothrombosis should be regarded as a systemic disorder with various local manifestations. 22 Nevertheless, with the grade of severity of CHD, PWVao increased in our study.
It has already been shown in several studies that arterial stiffness measured on the basis of elevated PWVao is associated with the risk of CVDs, particularly in patients with T2DM.5,23 In this study, additional parameters of arterial stiffness were investigated, and elevated values for AIx aortic and AIx brachial as well as elevated values for SBPao and PPao could be detected in our cohort substantiating the presence of arterial stiffness.
The demographic and clinical characteristics of the patients with T2DM and those with additional CHD showed some statistically significant but expected differences which were considered in the statistical analysis. Data from the cross-sectional analysis of the Innovative Medicine Initiative SUrrogate markers for Micro‐ and Macro‐vascular hard endpoints for Innovative diabetes Tools (SUMMIT) project revealed patient-dependent differences in PWV. Compared to patients without CHD, patients with T2DM and additional CHD had a higher age, a longer duration of diabetes and a lower diastolic blood pressure, 23 comparable to our cohort. Effects become less pronounced with increased age – from around 60 years of age. The systolic blood pressure in the subgroups of patients was in the normal or high-normal range not at least because of the higher age and the strict antihypertensive treatment. 6 In our study, all patients with T2DM + CHD were on antihypertensive medication compared to 74% of patients with T2DM − CHD. Regarding quality of metabolic control and obesity grade, no differences between the two groups were detected. The significantly increased BNP in patients with T2DM + CHD could be due to the underlying cardiac disease despite the BNP values being far below the upper limit of normal in both groups. The more aggressive metabolic treatment of CHD-patients and the higher proportion of prescribed lipid-lowering therapy in T2DM + CHD (92%) compared to in T2DM − CHD (66%) might account for the statistically significantly lower LDL-cholesterol in patients with T2DM + CHD. The influence of statin therapy on the concentration of MMPs and TIMPs is controversial. In a meta-analysis of clinical data from 2017, however, it was shown that statin therapy reduces TIMP-1 levels, but it does not influence MMP-9 and MMP-3 concentrations. 24
MMP and TIMP concentrations were increased in patients with T2DM compared to healthy adults. 25 Increased concentrations of the markers analysed in this study have also been described in acute coronary events (MMPs and TIMPs) or chronic heart failure (galectin-3). Loftus et al. 26 described increased concentrations of these markers in the context of atherosclerosis, in particular in acute atherosclerotic plaque rupture sustaining the assumption markers are elevated in acute events and are reduced to near normal values after convalescence. This might explain comparably low values of markers in our T2DM + CHD cohort.
For the first time, the correlation between the markers MMPs, TIMPs as well as galectin-3 and arterial stiffness in patients with T2DM with CHD was investigated. In other studies, in different populations such as healthy adults, patients with T2DM and patients with high blood pressure, it could be proven that MMPs and TIMPs are involved in arteriosclerotic processes and arterial stiffness.27-29 The participation of galectin-3 in the fibrotic process in the vessel wall and thus the contribution to arterial stiffness has been investigated in the general population. 30 Lorenzo-Almorós et al. 31 showed that galectin-3 is suitable as a marker for predicting cardiovascular events, especially in patients with CHD and additional T2DM.
Assuming that the markers of the ECM and galectin-3 depict different pathophysiological processes on the peripheral vessels, further analyses were carried out depending on the PWVao. Strong correlations between TIMP-4 and all indirect parameters of arterial stiffness were detectable in case of normal PWVao. In case of elevated PWVao, TIMP-4 and galectin-3 were correlated to PWVao although galectin-3 is only trendwise different between the PWVao groups (p for difference = 0.065). A previous study also showed an independent association between elevated PWVao and galectin-3 in a large cohort and thus confirms the findings obtained here. 30 In summary, TIMP-4 rather than galectin-3 and even the established atherosclerosis marker MMP-9 may represent the stiffening process in the peripheral vessels and may therefore be suitable for predicting increased vascular stiffness.
Limitations
This cross-sectional study recruited not optimally treated patients in a real-life clinical setting, and the patients were in inpatient treatment in order to optimise metabolic treatment. Thus, no rigorous inclusion and exclusion criteria were applied.
The arterial stiffness was measured using arteriography, a newer oscillometric method. Other non-invasive procedures are based on a tonometric or piezo-electric method and determine the arterial stiffness using the carotid-femoral PWVao as an indicator. 10 The comparability of the measurement methods is controversial, so the data should be compared depending on the method. 9
The number of cases should be mentioned as a limiting factor. In particular, the analysis between the severity of CHD and the parameters of the arteriography has only limited informative value.
Conclusion
Determination of arterial stiffness seems to be an effective and, compared to laboratory markers, more reliable measurement method for determining the peripheral vascular situation in patients with T2DM, but it does not clearly depict the coronary situation. Diabetes per se contributes to arterial stiffening, pronouncing its role as a CVRF. TIMP-4 should be further investigated as potential marker for predicting increased vascular stiffness as there is a significant correlation to PWVao independent from CHD status in T2DM.
Supplemental Material
sj-pdf-1-dvr-10.1177_14791641211046522 – Supplemental Material for Peripheral oscillometric arterial performance does not depict coronary status in patients with type 2 diabetes mellitus
Supplemental Material, sj-pdf-1-dvr-10.1177_14791641211046522 for Peripheral oscillometric arterial performance does not depict coronary status in patients with type 2 diabetes mellitus by Magdalene Jaeger, Bernd Stratmann and Diethelm Tschoepe in Diabetes & Vascular Disease Research
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.