
Abstract
Diabetic neuropathy is a troublesome complication of diabetes mellitus. It affects about 50% of patients with diabetes and may mask symptoms of ischemic conditions. Sudden blockade in blood flow to the limb known as acute limb ischemia (ALI) is a life-threatening disease associated with peripheral artery disease (PAD). Diabetes mellitus predisposes both to ALI and PAD, while also delaying recognition due to diabetic peripheral neuropathy.
We report a case of a patient with poorly controlled type 2 diabetes and atrial fibrillation who presented a rare occurrence of painless acute upper limb ischemia. Despite two embolectomies with positive revascularization, ischemia progressed, leading to amputation.
In the article we discuss management of the patient and the case’s similarity to diabetic foot disease. Our case report highlights the importance of vigilance against diabetes-related complications, which may manifest unusual symptoms and thus mask other dangerous ailments.
Introduction
Diabetic neuropathy (DN) affects 30%–50% of people living with diabetes and results from metabolic and microvascular nerve damage. 1 The most common form, distal symmetric polyneuropathy (DSP), presents with numbness, tingling, pain, and weakness in a “stocking and glove” pattern, and is strongly associated with foot ulcers and amputation. 2 Acute limb ischemia (ALI) is a vascular emergency defined by sudden arterial occlusion within 14 days, often due to embolism or thrombosis.3,4
We report a rare case of painless upper-limb ALI in a 70-year-old woman with poorly controlled type 2 diabetes, that led to amputation. In this study, we discuss clinical revelations of acute upper limb ischemia, and compare it with lower limb ischemia. Authors theorize about plausible cause of painless ischemia. Furthermore, the report explores limb-related complications of diabetes, emphasizing the resemblance between the discussed case and diabetic foot disease.
Case description
A 70-year-old female patient presented to the hospital with complaints of decreased hand motor function and paraesthesia related to the left limb. On examination the radial artery pulse was not palpable and the hand had pallor with slight mottling. The diagnosis of acute upper limb ischemia of Rutherford IIb severity was made. Notably, the patient denied having ever felt any pain in the affected limb. A decision to perform embolectomy was made. However, after 3 days obstruction in the axillary, ulnar and radial left artery emerged. A second embolectomy was undertaken, which successfully re-established vascular perfusion. The patient was discharged from the hospital.
On day 12 after the first embolectomy, the patient presented to the Emergency Department with complaints of fatigue, peripheral edema and loss of exercise tolerance. On examination the patient presented painless and dry ischemic changes on the distal part of left limb’s fingers from one to five (Figure 1 and 2). The left palm was covered with multiple bullous lesions. The cubital fossa was protected with a dressing after the previous angio-surgical intervention. The left arm was edematous. Abduction of the left arm was limited, and physiological pronation of the left forearm was moderate compared to the right forearm. Dorsal side of the affected limb, during hospitalization. Palmar side of the affected limb, during hospitalization.

The patient suffered from various comorbid conditions, including dysregulated and neglected type 2 DM, hyperlipidemia, hypertension, atrial fibrillation (AF), asthma and obesity. She had a history of an embolic ischemic stroke of the left cerebral hemisphere a few years before. Moreover, the patient had missed taking their morning anticoagulant medication on the day of presentation to the hospital.
Doppler ultrasonography revealed obstruction in left upper limb arteries. Blood flow in the left subclavian artery was detectable with high-resistance, and the left axillary artery had reduced flow velocities (Peak Systolic Velocity 30-35 cm/s). There was no detectable flow in the brachial artery in the cubital fossa or more distally. The patient was noted to be in AF.
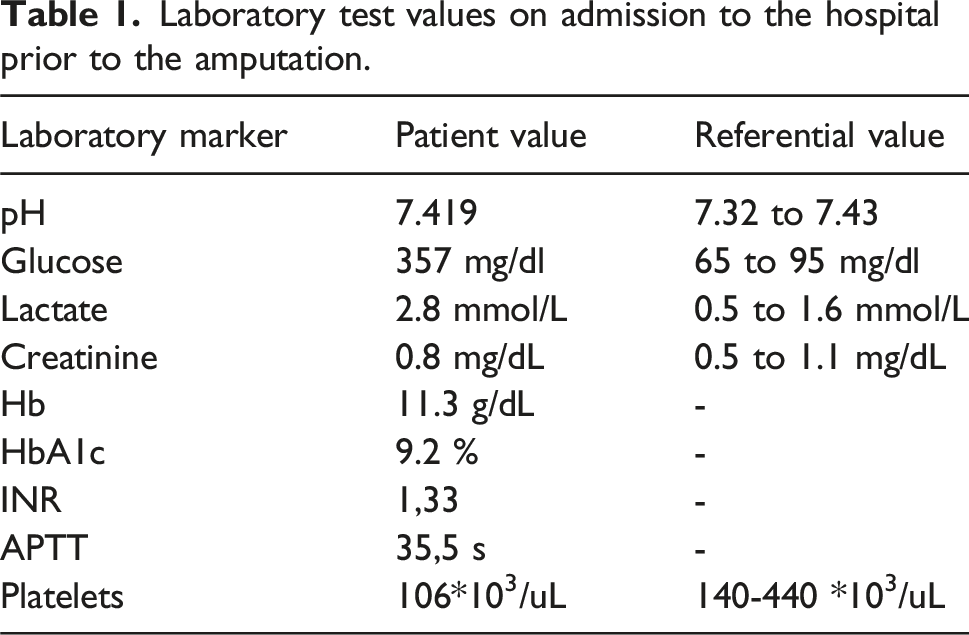
During hospitalization edema of the affected extremity increased and new bullous lesions appeared. Laboratory tests showed a decrease in hemoglobin (Hb) and increase of creatine (Table 1). A decision was made to perform amputation on the level of the left forearm. The surgical procedure went without complication.
After the amputation the patient underwent dietetic consultation where she was advised about lifestyle changes. Ophthalmological examination showed no significant abnormalities. She was referred to the orthopedic ambulatory service for future prosthesis preparation. Echocardiographic examination revealed thickened aortic valve leaflets with moderate regurgitation, concomitant moderate mitral regurgitation, evidence of pulmonary hypertension, and right ventricular dysfunction, with a reduced ejection fraction of 25%–32%.
From then on her diabetes was well controlled on empagliflozin, semaglutide, metformin and gliclazide.
Discussion
Acute limb ischemia
Acute limb ischemia most commonly affects the lower extremities. The characteristic symptoms of acute limb ischemia include pain, absence of a pulse, pallor and cooling of the skin, paresthesia, and loss of motor function in the limb.
Laboratory test values on admission to the hospital prior to the amputation.
ALI should be treated within 6–8 h depending on the severity of ischemia. 7 Decision about therapeutic management is made on the basis of Rutherford classification and determining the etiology of arterial blockage (thrombotic or embolic). Salvage of the limb can be performed by surgery or endovascular thrombolysis depending on the risk factors and contraindications.8,9 Amputation is reserved for cases of life-threatening conditions or irreversible ischemia (class III). 5

Differences between acute upper- and lower-limb ischemia
While acute limb ischemia (ALI) predominantly affects the lower extremities, upper-limb ALI is not uncommon and should not be considered atypical.10,12 One of the key differences lies in the pattern of collateral circulation. The upper limb has a well-developed collateral network around the shoulder and elbow, which can lead to a more gradual and less overt symptom onset. This often results in delayed diagnosis and intervention. In contrast, lower-limb ALI typically presents abruptly with pain, pallor, coldness, and paresthesia due to poorer collateralization and a greater susceptibility to muscle necrosis. 13
Therapeutic strategies also differ. Upper-limb ALI is most often managed surgically with procedures such as Fogarty balloon embolectomy. In contrast, lower-limb ALI-especially in cases of thrombotic occlusion, may benefit more from endovascular approaches such as catheter-directed thrombolysis or mechanical thrombectomy. 14
Painless presentation of ALI
This case highlights an uncommon form of acute upper limb ischemia, with ischemic changes occurring entirely without pain from onset. Prolonged ischemia damages the nerves causing paresthesia, although the first and most significant symptom is an unbearable pain of the affected limb. 15 Uncontrolled diabetes of the patient suggests that lack of protective pain sensation may be the effect of DPN. 2 In the presented case, the clinical manifestation was unusual due to the absence of pain at any stage of ischemia. Typically, ALI presents with a sudden onset of severe pain, which is often disproportionate to clinical findings and is considered one of the earliest and most sensitive indicators of ischemia. 15
In a 2012 study of 822 patients with ALI in all of the cases sudden onset of pain was present, including 111 patients with DM. 11 Although, literature describes cases of acute painless lower limb ischemia, due to aortic dissection or bilateral femoral thromboembolism, we have found no other cases of upper-limb acute ischemia with a painless course, which assures us that the presented case is unique.16,17
The painless progression observed in our patient may be attributed to diabetic peripheral neuropathy (DPN), which can blunt protective nociception. Ischemia-induced nerve damage may eventually lead to paraesthesia or motor loss.
Diabetic neuropathy
Diabetic neuropathy is a type of nerve damage that occurs as a complication of uncontrolled diabetes. It results from prolonged high blood sugar levels, which can impair nerve function throughout the body. This leads to segmental demyelination, axonal atrophy and degeneration, and neuron loss in the anterior horns and intervertebral ganglia. 2
Distal symmetric polyneuropathy (DSP) is one of the most common types of peripheral neuropathy. This condition primarily affects the peripheral nerves, beginning in the longest nerves of the body, which supply sensation and motor control to the feet and hands. The most common symptoms are numbness, tingling, or a “pins and needles” sensation, burning pain, especially at night, reduced ability to sense vibration, temperature and pain. 1
Damage to the peripheral nerves in distal symmetric polyneuropathy not only leads to sensory deficits but also predisposes patients to complications in the lower extremities, setting the stage for diabetic-related foot disease (DFD). Neuropathy along with ischemia is the main pathology related with DFD. 18
The literature describes widely painless lesions in the course of DFD.19,20 Depending on the predominant process, DFD may be neuropathic or ischemic. In the combined neuro-ischemic type, despite advanced ischemia, symptoms may be absent due to neuropathy. Clinically ischemic and neuro-ischemic ulcers develop on the distal part of extremity and the digits. 20 We suspect an analogous complication in our patient, due to poorly controlled diabetes, with a similar ischemic pattern and painless course.
However, no proper neurological examination has been made to prove diabetic neuropathy. Therefore, the discussed process is only hypothetical but still plausible due to the patient’s comorbidities.
Peripheral artery disease (PAD)
PAD, primarily caused by atherosclerosis, is associated with a high risk of amputation during acute limb ischemia (ALI). 21 The condition tends to be more severe in patients with diabetes, who face a significantly higher risk of complications. 19 Moreover, diabetic peripheral neuropathy may mask PAD symptoms, delaying diagnosis and treatment. 19
Multidisciplinary approach
Given the patient’s complex clinical profile, a multidisciplinary strategy was essential. She was referred to cardiology for further evaluation, including coronary angiography, due to exertional dyspnea, exercise intolerance, and edema—symptoms suggestive of coronary artery disease (CAD), especially in the context of atherosclerosis. The absence of chest pain may be attributed to diabetic neuropathy, which can mask typical anginal symptoms.
Pharmacological treatment included acetylsalicylic acid, bisoprolol, metildigoxin, eplerenone, torsemide, sacubitril/valsartan, and atorvastatin. Additionally, she received dietary counseling and was advised to follow a low-sodium, low-glycemic index diet, while monitoring blood glucose and blood pressure.
Diabetes care was optimized with empagliflozin, semaglutide, metformin, and gliclazide to slow neuropathy progression and reduce the risk of future ischemic events. Limb prosthesis planning requires a coordinated team approach, including stump care and rehabilitation. Psychological support was emphasized to promote adherence and reduce the risk of further complications. 22
In such cases, only integrated, interdisciplinary care can adequately address the full spectrum of a patient’s medical needs.
Conclusions
Distal polyneuropathy is a common complication of uncontrolled diabetes. Sensory dysfunction may mask minor and non-perceived injuries that contribute to the development of diabetic foot disease. A routine part of the consultation of patients with diabetes is to ensure that they are aware of the need to conduct regular visual self-inspection. The literature widely describes asymptomatic heart and lower limb ischemia. This case highlights that upper extremities might be threatened by painless limb-threatening ischemia as well. The atypical painless course of acute upper limb ischemia delayed limb salvaging procedures. Despite embolectomy leading to revascularization, the tissue ischemia was irreversible, leading to progressive necrosis and amputation of the affected limb.
Diabetic neuropathy is a serious complication that may mask symptoms of ischemia, and significantly delay patient’s treatment. Medical providers should remember about the possibility of neuropathy when examining patients with diabetes.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.