
Abstract
The aim of this study was to assess the blood vessel density and maturity in the skin of adults with type 1 diabetes in relation to the presence of late neurovascular complications. We included 148 patients (87 men) with a median (interquartile range) age of 41 (31–49) and median diabetes duration of 21 (17–30) years. Microvessel (CD133, CD34, CD31 and von Willebrand factor) markers were evaluated by indirect immunohistochemistry assay in material from a skin biopsy. Diabetic retinopathy was diagnosed using direct ophthalmoscopy, and diabetic kidney disease was estimated in people with increased albuminuria and a 10-year duration of diabetes or evidence of diabetic retinopathy . Diabetic peripheral neuropathy diagnosis was based on Toronto definition, cardiac autonomic neuropathy on validated ProSciCard III program. Microvessel density, assessed by CD34 and CD133, was significantly higher in patients with cardiac autonomic neuropathy [160 (125–175) vs 121 (100–154)/1 mm2, p = 0.001 and 92 (83–104) vs 79 (63–92)/1 mm2, p = 0.007, respectively] and CD34 in patients with diabetic peripheral neuropathy [135 (106–168) vs 121 (95–145)/1 mm2, p = 0.018], as compared with subjects without complications. In multivariate logistic regression, density of CD34 and CD133 positive vessels was associated with presence of cardiac autonomic neuropathy [odds ratio 1.016 (95% confidence interval: 1.002–1.029), p = 0.019 and odds ratio 1.037 (95% confidence interval: 1.008–1.067), p = 0.011, respectively]. It was independent from age, sex, diabetes duration, smoking status, body mass index and HbA1c value. Density of CD34 positive vessels was also associated with diabetic peripheral neuropathy, independently from sex and diabetes duration [odds ratio 1.009 (95% confidence interval: 1.001–1.020), p = 0.037]. Skin microvessel density is increased in adults with clinical evidence of neurovascular complications of type 1 diabetes. This is associated with predominance of the vessels of low maturity.
Keywords
Introduction
Despite advances in the treatment of diabetes, the prevention of its chronic complications remains a significant clinical challenge. Therefore, new prognostic markers for both micro- and macroangiopathy in diabetes are needed. 1 The neurovascular pathogenesis of late diabetic complications has been postulated recently. 2 Not only hyperglycaemia but also fluctuations of glycaemia lead to cellular hypoxia and mitochondrial reactive oxygen species generation that may promote endothelial dysfunction and parallel impaired activity of neurons. Eventually, prolonged tissue hypoxia leads to the development of late diabetic complications. 3
In the pathogenesis of diabetic complications, both microvascular deficiencies and proliferation coexist, sometimes simultaneously. The expression of growth factors, in particular, vascular endothelial growth factor (VEGF) is extensively increased as a response to hypoxia in patients with diabetic proliferative retinopathy. 4 On the contrary, long-lasting diabetes mellitus is characterized by impaired collateral growth and arteriogenesis, which is regarded as the ‘diabetic angiogenic paradox’. 5 A possible mechanism to explain the angiogenic paradox is VEGF resistance. 5 VEGF through binding to its cognate receptor promotes a multistep process which ends with endothelial cell (EC) differentiation into mature blood vessels. 6 Increased expression of VEGF and its receptors has been observed in highly vascularized tissues, particularly the retina. However, decreased concentrations of constitutive VEGF mRNA in medium to large arteries have been observed in vivo in humans, and this expression was found restricted to vascular smooth muscle cells. 7 The knowledge about factors which promote proper angiogenesis and inhibit impaired proliferation of dysfunctional vessels provides an opportunity for new treatments of diabetic complications. 8 Interestingly, skin, as one of the most accessible tissues, is an excellent material for the examination of microcirculation as well as ongoing processes in nerve tissue.
During new vessel formation, characteristic markers are expressed on the surface of the endothelium, while some other markers disappear. These could serve as determinants or risk factors for late diabetic complications. In our study, we used immunohistochemical methods to determine the morphological changes observed in diabetic microangiopathy. The aim of this study was to assess the blood vessel density and maturity in the skin of adults with type 1 diabetes (T1D) in relation to the presence of late diabetic neurovascular complications.
Materials and methods
Patients
The study included people with T1D who underwent routine follow-up in the Department of Internal Medicine and Diabetology, Poznan University of Medical Sciences in the years 2015–2017. Eligibility criteria were as follows: age >18 years, duration of T1D >10 years and patient consent to participate in the study. Exclusion criteria were as follows: coagulation disorders (activated partial thromboplastin time (APTT) > 37 s, international normalized ratio (INR) > 1.1, platelet count < 100 G/mm3), anticoagulant or antiplatelet treatment, skin disorders in the biopsy area and lack of patient consent. Informed consent was obtained from all individual participants included in the study. The research protocol was approved by the Ethical Committee of the Poznan University of Medical Sciences (No. 1064/15). Medical research was conducted according to the World Medical Association Declaration of Helsinki. Finally, we included 148 patients with T1D (87 male, 61 female) with median age of 41 (31–49) years and median diabetes duration of 21 (17–30) years.
Clinical characteristics of the study group is presented in Table 1.
Characteristics of the study group.
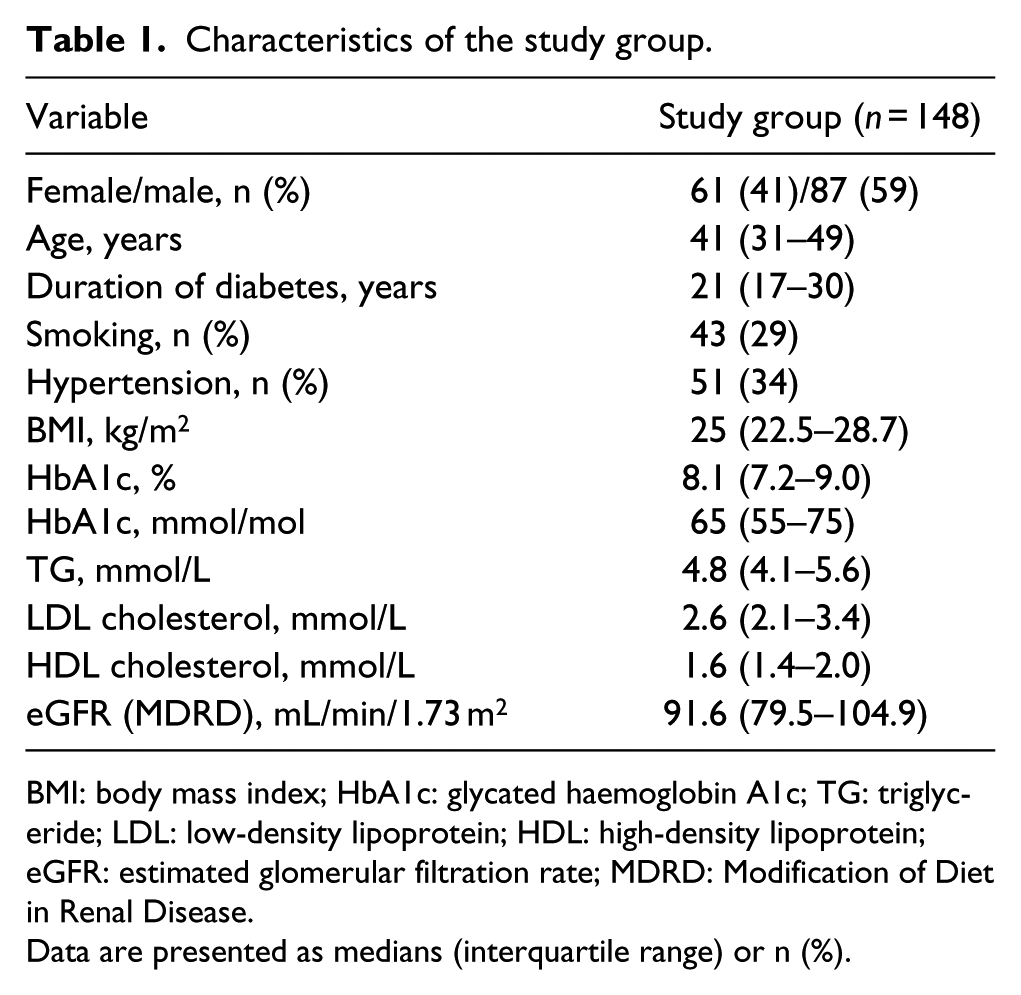
BMI: body mass index; HbA1c: glycated haemoglobin A1c; TG: triglyceride; LDL: low-density lipoprotein; HDL: high-density lipoprotein; eGFR: estimated glomerular filtration rate; MDRD: Modification of Diet in Renal Disease.
Data are presented as medians (interquartile range) or n (%).
Data collection procedures
Patients completed a questionnaire on the history of diabetes, co-morbidities, medication use and smoking history. All patients underwent a complete physical examination with anthropometric measurements (body mass, height). Body mass index (BMI) was calculated from the following equation: BMI = weight (kg)/squared height (m2).
Laboratory tests
Blood samples (10 mL) were taken after 10 h of fasting with minimum occlusion of the vein using an S-Monovette blood collection system. The serum concentrations of creatinine, total cholesterol, high-density lipoproteins (HDLs) cholesterol, low-density lipoproteins (LDLs) cholesterol and triglycerides (TGs) were measured using standard methods. Estimated glomerular filtration rate (eGFR) was calculated using the Modification of Diet in Renal Disease (MDRD) study equation. HbA1c was measured in venous blood with competitive turbidimetric inhibition immunoassay method on Cobas analyzer (Roche Diagnostics, Basel, Switzerland) and expressed in % and in IFCC units (mmol/mol) according to DCCT/NGSP (IFCC: The International Federation of Clinical Chemistry and Laboratory Medicine; DCCT: Diabetes Control and Complication Trial; NGSP: National Glycohemoglobin Standardization Program).
Assessment of diabetic complications
Diabetic retinopathy
Diabetic retinopathy (DR) was diagnosed using direct ophthalmoscopy through dilated pupils. Fundus examinations was performed using an indirect Volk lens. Evaluation of ophthalmoscopy was performed for the entire group by the same ophthalmologist experienced in DR assessment. DR was graded according to the classification of the American Academy of Ophthalmology as: no retinopathy, mild nonproliferative, moderate nonproliferative, severe nonproliferative and proliferative retinopathy. 9
Diabetic kidney disease
The urinary albumin excretion was assessed on the basis of a 12 h urine collection, with the simultaneous determination of the albumin/creatinine index in the morning urine. Urinary albumin excretion from 30 to 300 mg per day in two of the three urine collections and albumin/creatinine ratio >30 mg/g in the morning urine sample was considered to be increased albuminuria. Diabetic kidney disease (DKD) was diagnosed in people with increased albuminuria and a 10-year duration of diabetes or shorter duration with coexistence of retinopathy. 10 DKD was divided into stages based on the result of the eGFR: stage 1 (eGFR ⩾ 90 mL/min/1.73 m2), stage 2 (eGFR 60–89 mL/min/1.73 m2), stage 3 (eGFR 30–59 mL/min/1.73 m2), stage 4 (eGFR 15–29 mL/min/1.73 m2) and stage 5 (eGFR < 15 mL/min/1.73 m² or treatment with dialyses).
Diabetic peripheral neuropathy
The study was based on Toronto definition of probable DPN. Symptoms of peripheral neuropathy were evaluated on the basis of the medical history. During the standard examination, touch sensation was evaluated with the use of 10 g monofilament; feeling of vibration, with the 128 Hz tuning fork; temperature sensation, with Tip Therm; and pain sensation, with neurotips. Achilles tendon reflexes were also evaluated. DPN was diagnosed in patients with two or more of the following five elements: the occurrence of symptoms, abnormal sensation of touch, vibration, temperature and absence of ankle reflexes. 11
Cardiac autonomic neuropathy
Cardiac autonomic neuropathy (CAN) was assessed with the use of validated ProSciCard III program. 12 Heart rate variability at rest in a supine position and under standardized stimuli (deep breathing test, Valsalva manoeuvre, orthostatic test) was studied. During the examination, the electrocardiogram of the patient was monitored on the computer screen. On the basis of the calculated inter-beat (R-R) interval, the parameters of autonomic neuropathy were calculated and subsequently compared with age- and sex-specific standard values. The test at rest lasted 5 min, in a continuous electrocardiogram (ECG) record, each QRS complex is detected, and the so-called normal-to-normal (NN) intervals are calculated; the results were expressed as heart rate variability (HRV) index [the integral of the density distribution (that is, the number of all NN intervals) divided by the maximum of the density distribution], TINN (triangular interpolation of NN interval histogram), standard deviation of the NN intervals (SDNN) and the square root of the mean squared differences of successive NN intervals (RMSSD). The provocative tests were performer according to standards of Task Force of the European Society of Cardiology, North American Society of Pacing and Electrophysiology. The result of the deep-breathing test (six cycles per minute) was expressed as the mean value for the ratio of maximal RR interval during breathing-out and minimal RR during breathing-in. The result of the lying-to-standing test was expressed as the ratio of the longest RR interval (about the 30th beat) over the shortest RR interval (about the 15th beat). The Valsalva test was performed three times consecutively and the mean value for the Valsalva ratio (VR) was calculated. CAN was diagnosed if the results of two of four tests were abnormal. 13
Biopsy procedure
The skin biopsy was performed on the distal part of the lower limb (10 cm above the lateral malleolus) using a sterile, disposable 3 mm biopsy punch with plunger (Disposable Biopsy Punches, Integra™ Miltex®). 14 Before the biopsy, the site was anesthetized with 2% lidocaine injections in sterile conditions. The test lasted 10 min and was minimally invasive. The wound after the biopsy did not require suturing. The excised tissues were fixed in Bouin solution for 24 h at room temperature, and then embedded in paraffin blocks.
Immunohistochemistry
We used CD133, CD34, CD31 and von Willebrand factor (vWF) as markers of maturity, as well as morphological and functional endothelial integrity. 15 Paraffin-embedded tissue blocks were cut into 3- to 4-µm-thick sections on a semi-automatic rotary microtome (Leica RM 2145, Leica Microsystems, Nussloch, Germany). All of the immunohistochemistry (IHC) analyses employed the StreptABComplex/HRP method modified by the use of biotinylated tyramine (Dako Catalyzed Signal Amplification System, Peroxidase, K1500, DakoCytomation A/S, Glostrup, Denmark). The endogenous peroxidase activity was blocked with 10% hydrogen peroxide. The staining IHC protocol included following steps: (1) preincubation with the appropriate normal goat serum in phosphate buffered saline for 30 min at room temperature, (2) incubation with the specific primary antibody overnight at 4°C in a hybridization chamber, (3) incubation with the secondary antibody for 60 min at room temperature, and finally and (4) antigen-antibody complexes staining using 0.5% 3,3′-diaminobenzidine (DAB) (Sigma Chemical Co., St. Louis, MO, USA).
The specific primary antibodies used in the study protocol were the following: anti-CD133 (Novus Biologicals, Littleton, CO, USA; code NB300–266, diluted 1:3000), anti-CD34 (Dako, Glostrup, Denmark; code M7165, diluted 1:30), anti-CD31 (Dako, Copenhagen, Denmark; code M0823, diluted 1:20) and anti-vWF (Dako; code M0616, diluted 1:30). All tissue sections were analysed under an AxioImager Z.1 light microscope and selected pictures were taken with an attached AxioCam MRc5 digital camera (Carl Zeiss). The negative controls consisted of specimens incubated with non-immune IgG1 (X-0931, Dako, Gdynia, Poland) and sections for which the primary or secondary antibody was omitted. All of the sections from blood vessels samples from an individual patient were processed in the same IHC experiment.
Morphometric analyses
Microvessel density (MVD), defined as the mean number of blood vessels presented in 1 mm2 of analysed tissue, was calculated using the ‘hot spots technique’. The histological preparation was viewed under a small magnification (20×) by selecting three areas with the highest number of blood vessels. Then the vessel sections were counted under a magnification of 40× in a selected area. The arithmetic mean of the three ‘hot spots’ was calculated for microvessel number and subsequently calculated to 1 mm2. This procedure was applied separately for CD133, CD34, CD31 and vWF. Slides were scanned using the Mirax Midi scanner (Carl Zeiss) and were viewed using CaseViewer (3DHISTECH Ltd. Budapest, Hungary). All of the analyses were evaluated independently by two scientists on coded samples that included positive and negative controls.
Statistical analysis
The Mann–Whitney U test was used for comparing quantitative variables and Fisher exact test for categories. To compare vascular markers in three groups with different retinopathy status (no – nonproliferative – proliferative retinopathy), Kruskal–Wallis test and post-hoc Dunn’s tests were used. Multivariate logistic regression was used to control for possible confounders when analysing association between vascular markers and late diabetic complications. Multivariate regression models included the following variables: age, sex, diabetes duration, smoking status, BMI, and HbA1c (CAN) or sex and diabetes duration (DPN). Receiver operating characteristics (ROC) curve analysis was used to determine the cut-off values of vascular marker density to distinguish subjects with DPN or CAN from those without evidence of these complications. The results of comparative analyses were presented as medians and interquartile ranges (IQRs) or as numbers and percentages (%). A p value less than 0.05 was considered statistically significant. Data were analysed using Statistica v. 13 (StatSoft Inc., Tulsa, OK, USA), MedCalc v. 18.5 (MedCalc Software bvba, Ostend, Belgium) (Kruskal–Wallis and Conover-Iman tests) and GraphPad Prism v. 7.00 (GraphPad Software, La Jolla, CA, USA) (figures).
Results
In the study group, 51 (34%) of patients had arterial hypertension, 43 (29%) were current active smokers, 36% used medications containing angiotensin-converting enzyme inhibitors (ACE-I) or angiotensin receptor blockers (ARB) and 27% statins. The HbA1c value was 8.1% (7.2–9.0); 65 (55–75) mmol/mol.
Seventy-three patients (50%) had DR, 21 (14%) had DKD, 57 individuals (39%) met the criteria for the diagnosis of DPN and CAN was diagnosed in 19 subjects (14%). The study group included 55 (37.2%) individuals without chronic neurovascular complications and 93 (62.8%) with at least one complication.
Immunopositive blood vessels were found in both layers of dermis (papillary and reticular dermis) in all samples. CD34 and CD133 were expressed in ECs as well as individual smooth muscle cells present in arterioles and meta-arterioles. CD31 and vWF (if present) were expressed exclusively in ECs.
The median MVD determined by CD34 blood vessels per 1 mm2 dermal biopsies was 121 (100–155) and by CD133 79/mm2 (63–92), by vWF 50/1 mm2 (40–69) and by CD31 38/1 mm2 (19–56). The values given above were calculated for both layers of the dermis (papillary and reticular dermis). In addition, there were no significant differences for MVD assessed in the particular skin layers independently.
Individuals without chronic neurovascular complications were younger than those with at least one complication 36 (23–42) versus 44 (34–53) years, had shorter diabetes duration [18 (14–23) vs 25 (20–30) years] and were rarely diagnosed with hypertension 7 (13%) versus 44 (47%) (p < 0.001). In the next step, we divided patients into groups depending on what complications were found. Comparison of groups of patients with T1D without and with any and specific complications is shown in Tables 2 and 3.
Comparison of groups of patients with type 1 diabetes without chronic neurovascular complications and those with at least one complication.
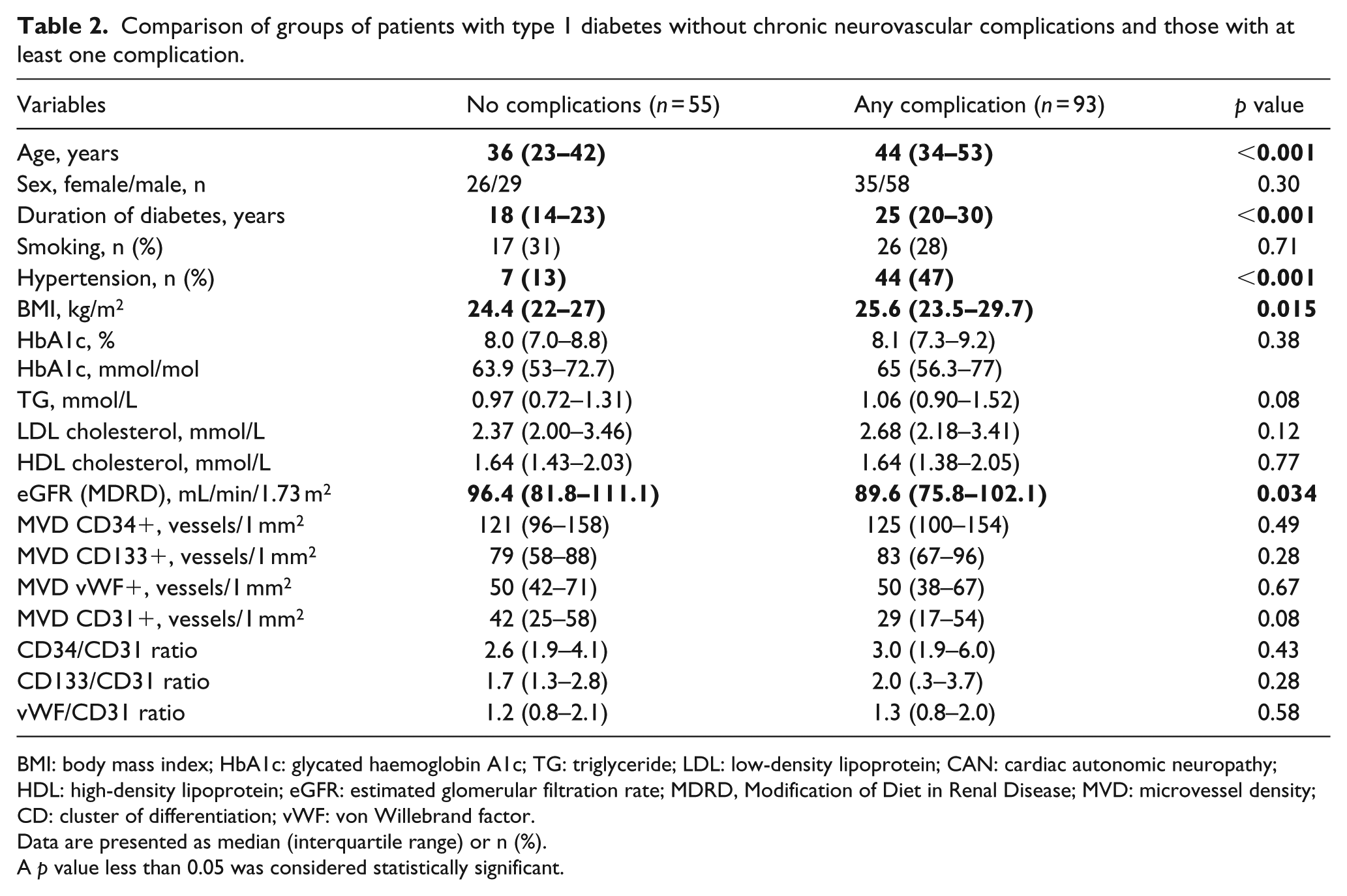
BMI: body mass index; HbA1c: glycated haemoglobin A1c; TG: triglyceride; LDL: low-density lipoprotein; CAN: cardiac autonomic neuropathy; HDL: high-density lipoprotein; eGFR: estimated glomerular filtration rate; MDRD, Modification of Diet in Renal Disease; MVD: microvessel density; CD: cluster of differentiation; vWF: von Willebrand factor.
Data are presented as median (interquartile range) or n (%).
A p value less than 0.05 was considered statistically significant.
Comparison of groups of patients with type 1 diabetes in relation to late diabetic complications.
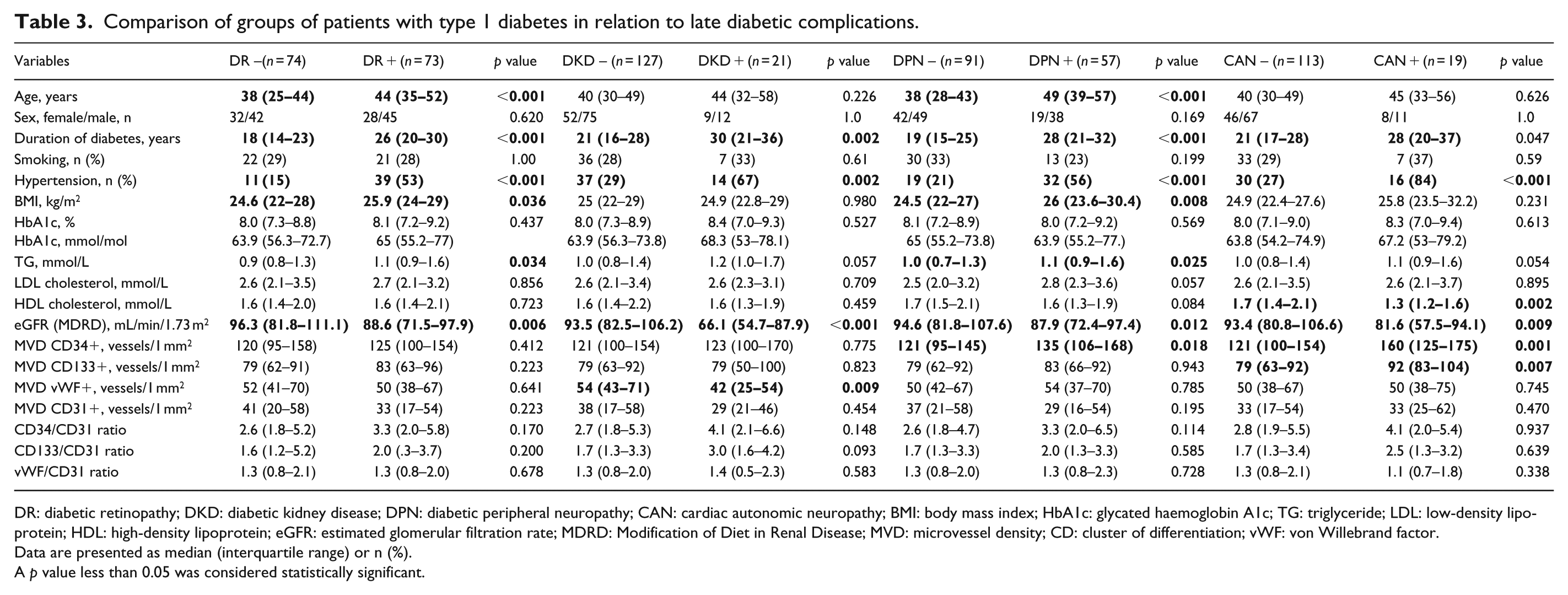
DR: diabetic retinopathy; DKD: diabetic kidney disease; DPN: diabetic peripheral neuropathy; CAN: cardiac autonomic neuropathy; BMI: body mass index; HbA1c: glycated haemoglobin A1c; TG: triglyceride; LDL: low-density lipoprotein; HDL: high-density lipoprotein; eGFR: estimated glomerular filtration rate; MDRD: Modification of Diet in Renal Disease; MVD: microvessel density; CD: cluster of differentiation; vWF: von Willebrand factor.
Data are presented as median (interquartile range) or n (%).
A p value less than 0.05 was considered statistically significant.
MVD was similar in group with and without retinopathy. However, patients with proliferative retinopathy had significantly higher values of CD34/CD31 and CD133/CD31 indices than patients without retinopathy [5.0 (3.1–6.4) vs 2.4 (1.7–4.1), p = 0.016 and 3.3 (1.7–4.8) vs 1.6 (1.2–2.8), p = 0.032, respectively] (Table 4).
Comparison of groups of patients with type 1 diabetes without and with retinopathy.
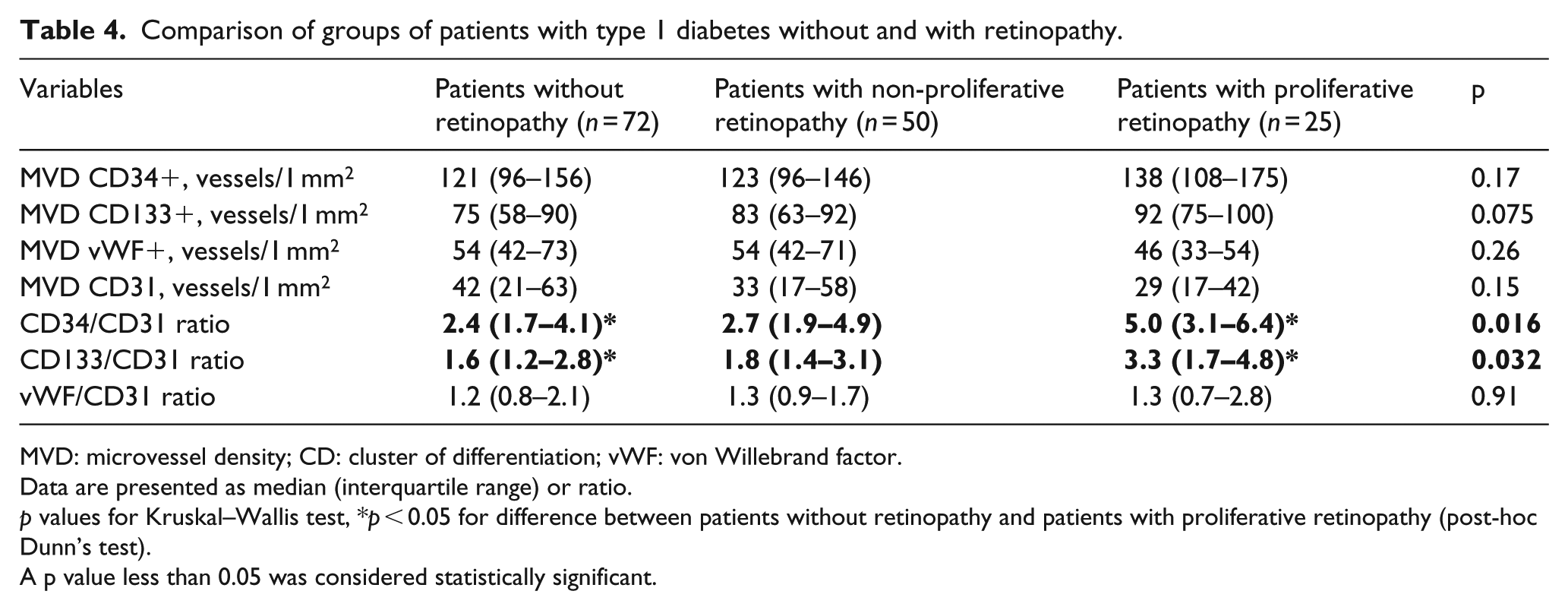
MVD: microvessel density; CD: cluster of differentiation; vWF: von Willebrand factor.
Data are presented as median (interquartile range) or ratio.
p values for Kruskal–Wallis test, *p < 0.05 for difference between patients without retinopathy and patients with proliferative retinopathy (post-hoc Dunn’s test).
A p value less than 0.05 was considered statistically significant.
Patients with DKD had lower expression of vWF than subjects without DKD [42 (25–54) vs 54 (43–71)/1 mm2, p = 0.009].
MVD determined by CD34 was higher in patients with DPN [135 (106–168) vs 121 (95–145)/1 mm2, p = 0.018] (Figure 1). Moreover, MVD assessed by CD34 and also CD133 was significantly higher in patients with CAN [160 (125–175) vs 121 (100–154)/1 mm2, p = 0.001 and 92 (83–104) vs 79 (63–92)/1 mm2, p = 0.007, respectively] (Figures 2 and 3).
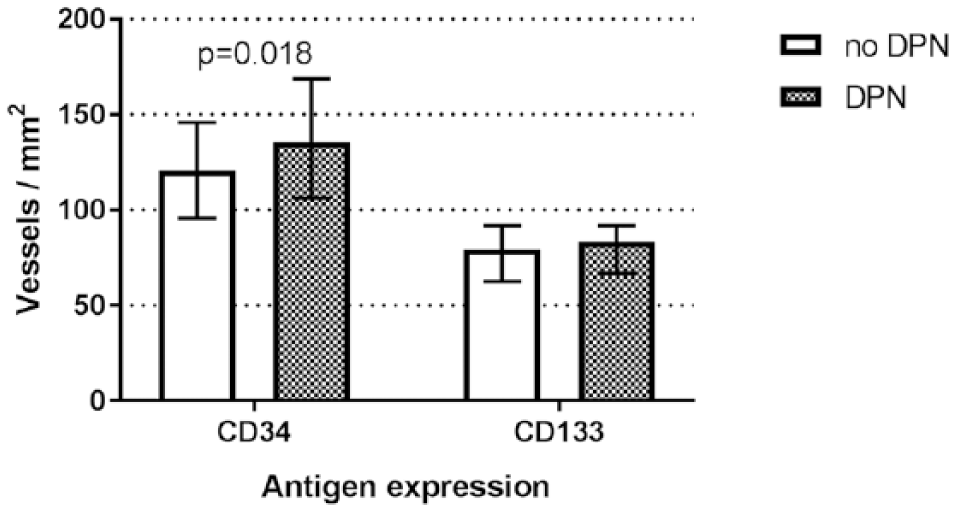
Comparison of microvessels density defined by CD34 and CD133 in skin biopsies of adults with type 1 diabetes without and with diabetic peripheral neuropathy (DPN).
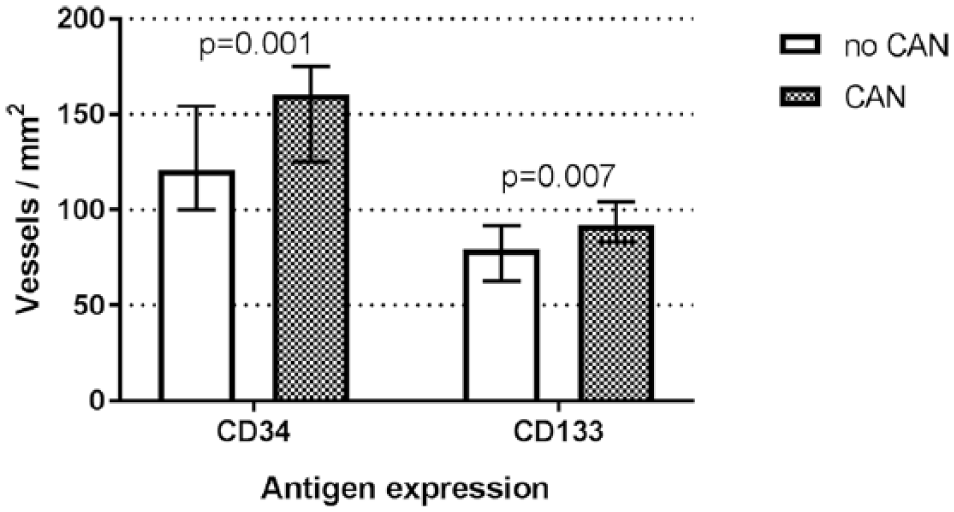
Comparison of microvessels density defined by CD34 and CD133 in skin biopsies of adults with type 1 diabetes without and with cardiac autonomic neuropathy (CAN).
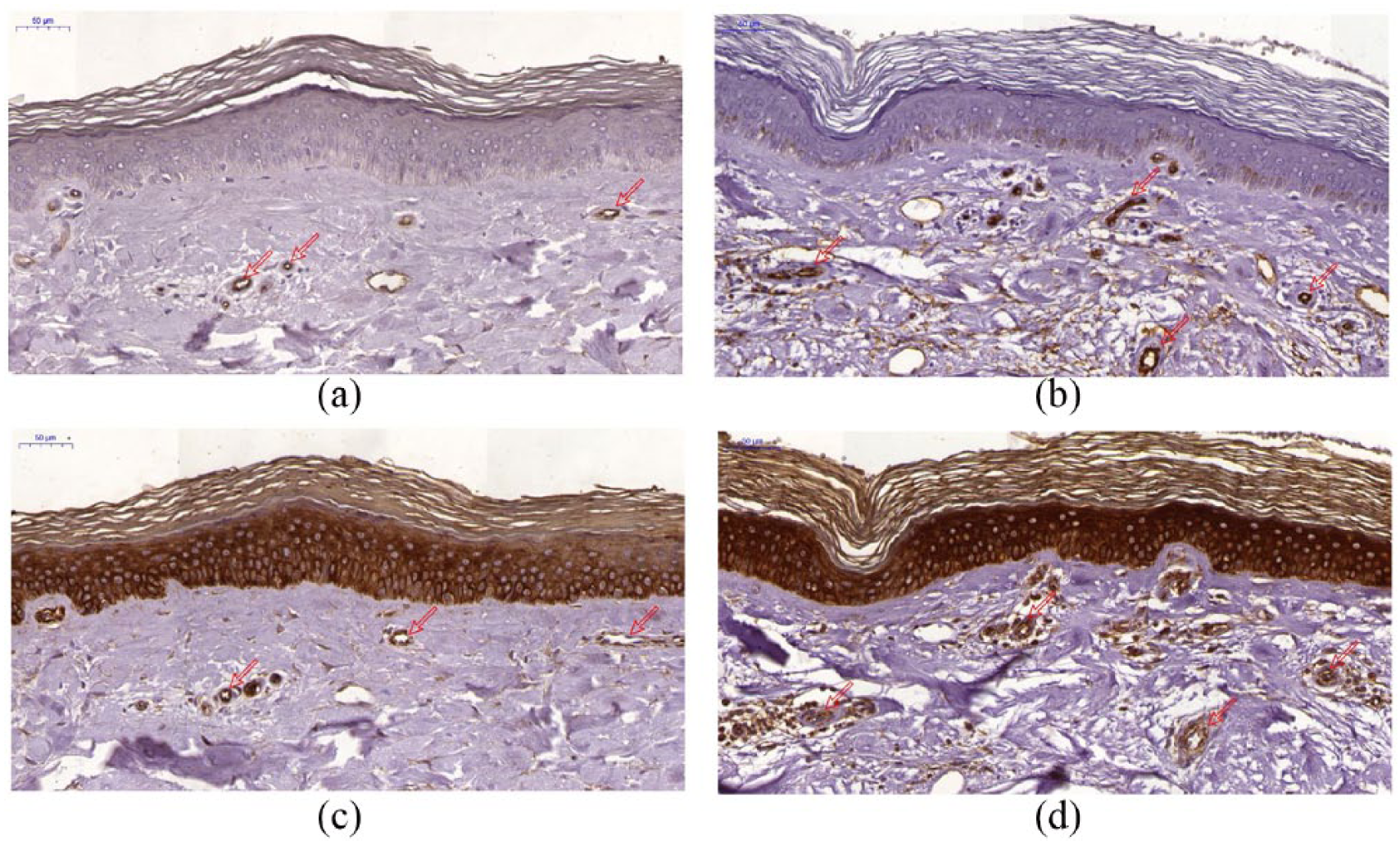
Demonstration of microvessels density in skin biopsies of adults with type 1 diabetes. Subsequent sections were stained by immunohistochemistry to show MVD defined by (a, b) CD34 and (c, d) CD133 expressions. (a) and (c) were obtained from representative patient without diabetic complications. (b) and (d) were obtained from patient with complication. Notice significantly higher microvessel density defined by CD34 and CD133 in patient with complications. On micrographs, the CD34 reaction is also visible in the reproductive layer of epidermal cells, and CD133 in the entire epidermis (in the case of CD133, the reaction seems to be unspecific) Scale bar = 50 µm.
In multivariate logistic regression density of CD34 positive vessels was associated with DPN, independently from sex and diabetes duration [odds ratio (OR) 1.009 (95% confidence interval (CI): 1.001–1.020), p = 0.037]. Density of CD34 and CD133 positive vessels was also associated with the presence of CAN [OR 1.016 (95% CI: 1.002–1.029), p = 0.019 and OR 1.037 (95% CI: 1.008–1.067), p = 0.011, respectively], independently from age, sex, diabetes duration, smoking status, BMI and HbA1c value.
In ROC curve analysis, for DPN, when choosing a CD34 cut-off point of 121/mm2 (optimal Youden index), sensitivity was 61% and specificity was 58%. The area under the ROC curve was 0.62.
For CAN, when choosing a CD34 cut-off point of 117/mm2, sensitivity was 94% and specificity was 45%. The area under the ROC curve was 0.74. When choosing a CD133 cut-off point of 83/mm2, sensitivity was 74% and specificity was 64%. The area under the ROC curve was 0.70.
Discussion
Traditionally, late diabetic complications were classified as micro-, macroangiopathy and neuropathy. Recently, increasing awareness of parallel pathology of microcirculation and nerve fibres resulted in the concept of neurovascular complications of diabetes. Our results confirm association between increased formation of new vessels and late complications of diabetes. This is indicated by high prevalence of CD34, a marker of microvascular ECs. Of notice, the angiogenesis is most intensive in patients with advanced complications, namely, cardiac autonomic neuropathy (CAN) and proliferative retinopathy. Moreover, the results might suggest impaired arteriogenesis in people with DKD as these patients had lower expression of vWF, a protein expressed by mature endothelium.
One of our research objectives was to select vascular marker that could serve as an attribute for development of neurovascular complications. We evaluated the immunohistochemical expression of CD133, a marker of endothelial progenitor cells (EPCs); CD34, a marker of late EPCs; and CD31 and vWF as markers of mature ECs in the skin of people with diabetes. 15 In 1997, Asahara discovered angiogenic cells that participate in endothelial repair and angiogenesis, including neovascularization. 16 These are derived from the bone marrow and have properties of embryonal angioblast. Thus, they have been termed EPCs and are characterized by the expression of CD133 (early EPCs) and CD34 (late EPCs, do not express CD133). The process of maturation, in which cells gradually lose their progenitor properties (CD133) and start the expression of mature endothelial markers (CD31, vWF), is controlled by serum VEGF.17–19 In our study, the median MVD defined by CD133 and CD34 antigen expression was increased as compared with the number of CD31 positive cells and expression of vWF in relation to all assessed late complications (Figure 4). In addition, higher CD133/CD31 and CD34/CD31 ratios in individuals with complications, even if not statistically significant, suggest activation of reparative mechanisms in this population. Previously, we have shown that generally in the whole population of individuals with diabetes, the expression of selected markers was not increased compared with healthy controls. 20 It seems that the increased expression of vascular markers occurs at the moment or parallel to the appearance of complications. The results do not allow to specify that one of them precedes the development of neurovascular complications. The obtained results for the expression of CD34 seem to be the most promising. In multiple regression analysis, CD34 was independently related to the presence of both DPN and CAN. However, the ROC curve analysis does not allow the designation of CD34 as sufficiently sensitive marker to recognize neuropathy. The ROC curve results appear to be more promising for CAN. This result may partly be associated with a more reliable method of diagnosing autonomic neuropathy with the use of ProSciCard than peripheral based on Toronto definition of probable peripheral neuropathy. Second, the results suggest that angiogenesis has greater impact and is markedly increased particularly in patients with CAN, in whom both CD34 and CD133 were significantly higher.
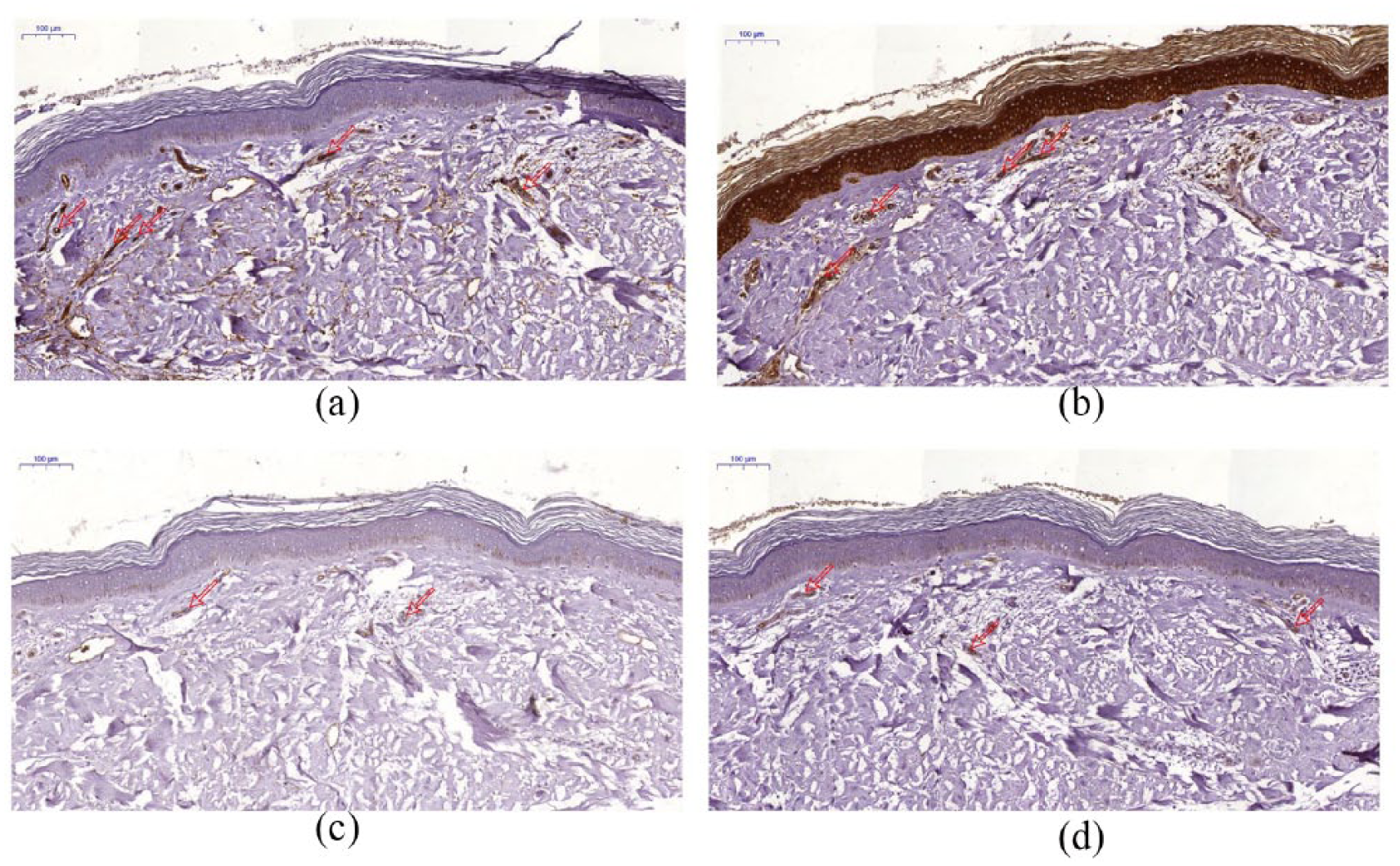
Demonstration of microvessels density in skin biopsies of adults with type 1 diabetes. Subsequent sections were stained by immunohistochemistry to show the MVD defined by (a) CD34, (b) CD133, (c) CD31 and (d) vWF expression. (a) and (b) antigens’ expression were increased as compared with the (c) and (d), and were obtained from representative patient with diabetic complications. Notice significantly higher microvessel density defined by CD34 and CD133 in patient with complications. Scale bar = 100 µm.
Despite advances in the treatment of diabetes, we observed that peripheral neuropathy symptoms occur in 39% and autonomic neuropathy in 14% of patients with approximately 20 years of disease duration. In diabetes, the function of microcirculation is closely linked to neuronal activity. Hyperglycaemia impairs the function of ECs and neurons. Abnormal glucose concentrations are responsible for intracellular metabolism defects and lead to metabolic stress. Imbalance between vasoconstricting and vasorelaxating factors produced by endothelium decreases blood flow in microcirculation leading to hypoxia that stimulates formation of new blood vessels. 21 The majority of the energy consumption in the nervous system is associated with neuronal activity and cycling of neurotransmitters. In addition, vasculature supports neuronal activity and its metabolic demands. In diabetes, when microcirculation is disturbed, impaired blood flow in nerve nutrient vessels leads to further degeneration of nerves.22,23 However, there are no data concerning angiogenetic markers and neuropathy development as well as its advancement in diabetes type 1.
We did not find statistically significant association between expression of biomarkers and the presence or degree of retinopathy. It cannot be excluded that with direct ophthalmoscopy, early stages of retinopathy were underdiagnosed. Use of more sensitive methods, for example, angiography with optical coherence tomography (angio-OCT) would allow verifying this finding. However, we observed the tendency to higher expression of biomarkers of lower maturity and significantly higher values of CD34/CD31 and CD133/CD31 ratios in subjects with proliferative retinopathy as compared with patients with nonproliferative as well as without retinopathy. Higher CD133/CD31 ratio that is recognized as renewal index confirms activation of reparative mechanisms in this population. Our results support the concept that skin may be treated as a model of processes that take place in the entire microcirculation.
Interestingly, we observed decreased number of mature blood vessels (defined by vWF) and no increase in MVD assessed by CD34 and CD133 in individuals with DKD. Diagnosis of DKD is one of the strongest risk factors for coronary heart disease in patients with T1D. 24 The lower expression of mature vessel markers in these subjects, which reflects decreased arteriogenesis, may indirectly explain the abnormal angiogenetic processes in diabetes. These processes lead to impaired coronary collateral vessel development that contributes to the excessive cardiovascular risk. In kidneys, the increase in glomerular filtration rate seen in early diabetes is regarded as a response to excessive angiogenesis. 25 Acevedo et al. have evaluated expression of the adhesion molecule CD34 in renal glomerular cells. Diabetes triggers an increased labelling for CD34 in renal tissues, mostly in plasma membranes of glomerular endothelium and mesangial processes, as compared with young normoglycemic animals. However, the level of labelling in old rats with diabetes and old healthy control rats was similar. 26 DKD in our study was diagnosed in people with increased albuminuria and either a 10-year duration of diabetes or evidence of retinopathy. 10 With this diagnosis, we have recognized much less DKD than other complications. Treatment with ACE-I or ARB could also influence the diagnosis and staging of DKD. In our patients with DKD and a median of 30 years of diabetes duration, we have not found the association between DKD and CD34+. The results suggest that in long-lasting diabetes complicated by kidney disease, angiogenesis is impaired and insufficient in view of the increased degeneration of vessels.
Conclusion
The density of skin microcirculation in patients with T1D and neuropathy as well as proliferative retinopathy is higher as compared with those without complications. This is associated with predominance of the vessels of low maturity. The results confirm the angiogenic processes involved in the pathogenesis of neuropathy and the neurovascular nature of late complications.
Footnotes
Acknowledgements
We would like to thank Dr Hanna Faza for ophthalmologist experience in diabetic retinopathy assessment.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The study was funded by the Poznan University of Medical Sciences (No. 502-14-02234382-41190) and scientific grant of Diabetes Poland.