
Abstract
Objective
To evaluate the association between GGT/HDL-C ratio and resolution of MetS in adults after sleeve gastrectomy (SG).
Methods
We conducted a retrospective cohort study using secondary data from a Peruvian bariatric center. The study population consisted of adults aged 18 and above who underwent laparoscopic SG and were diagnosed with MetS prior to the surgery. The main outcome measured was MetS resolution 6 months post-surgery and the exposure variable was the GGT/HDL-C ratio.
Results
We analyzed 137 patients with a mean age of 38.9 ± 10.9 years; 64.2% were females. The median GGT/HDL-C ratio was 1.1 [0.7 – 1.5], and 83.9% of patients experienced resolution of MetS. Furthermore, both the middle tertile of GGT/HDL-C (aRR: 1.28; 95% CI: 1.04 - 1.58; p = .019) and the lowest tertile (aRR: 1.27; 95% CI: 1.01 - 1.60; p = .038) showed a significant association with the resolution of MetS.
Conclusion
Eight out of 10 patients undergoing SG experience resolution of MetS within 6 months after surgery. Patients in the middle and lower tertiles of the GGT/HDL-C were more likely to achieve this outcome. Therefore, the GGT/HDL-C ratio should be considered a valuable and efficient biomarker for preoperative assessment of bariatric surgery candidates.
Keywords
Highlights
• This study is the first to investigate the GGT/HDL-C ratio as a predictive marker for the resolution of MetS in adults undergoing sleeve gastrectomy. • A lower GGT/HDL-C ratio pre-surgery was linked with a higher probability of resolving MetS 6 months after sleeve gastrectomy. • By examining MetS in Peruvian patients, the research fills a critical data void and extends understanding of MetS in Latin populations. • The GGT/HDL-C ratio seems to be a useful preoperative indicator to help tailor surgery and postoperative plans for patients with MetS.
Introduction
Metabolic syndrome (MetS) is a cluster of biological factors including insulin resistance, dyslipidemia, and central obesity. 1 Bariatric surgery is notably effective in resolving metabolic comorbidities linked to obesity such as type 2 diabetes mellitus (T2DM), non-alcoholic fatty liver disease (NAFLD), and MetS in adult patients. 2
Several studies have explored various laboratory parameters for predicting MetS. These include levels of high-density lipoprotein cholesterol (HDL-C), 3 gamma-glutamyl transferase (GGT), 4 fasting glucose, 5 insulin, 6 and glycated hemoglobin. 7 However, the effectiveness of using some of these parameters individually in predicting specific metabolic diseases has been questioned. 8 In a Chinese study, the GGT/HDL-C ratio was used in adults with a normal BMI or overweight to explore the relationship between the ratio and NAFLD. They found that the top quartile was significantly associated with the prevalence of NAFLD and MetS. 8 However, in assessing its performance using the area under the curve (AUC), the study only analyzed the GGT/HDL-C ratio for NAFLD prevalence, excluding MetS. 8 This limitation, along with the specific population studied, restricts the extrapolation of these findings to other ethnic groups, such as the Latin population. Additionally, there has been no study examining the relationship between the GGT/HDL-C ratio and the resolution of MetS in patients undergoing sleeve gastrectomy. This gap highlights the need for further research in this area.
In Latin America, the prevalence of MetS is 24.9%, 9 whereas in Peru, a prevalence of 16.8% has been reported. 10 Specifically, the prevalence in Metropolitan Lima is 20.7%, compared to 21.5% in the rest of the coast, and one in every four women faces this condition.10,11 Likewise, due to the rise in obesity and other comorbidities, the Roux-en-Y gastric bypass (RYGB) has been the most commonly used method globally for many years, but in Peru, sleeve gastrectomy is more commonly preferred. 12 Therefore, this study aimed to assess the association between GGT/HDL-C ratio and MetS resolution in patients undergoing sleeve gastrectomy.
Methods
Study design and population
This was a retrospective cohort study based on an analysis of secondary data. The target population comprised patients aged 18 years and older who underwent bariatric surgery at a Peruvian clinic between 2017 and 2022. Eligibility criteria included a BMI ≥30 kg/m2 and a pre-surgery diagnosis of MetS (Supplementary Figure 1). The diagnosis of MetS was based on the International Diabetes Federation (IDF) criteria. 13 Patients with self-perceived harmful consumption of alcohol, tobacco, and/or drugs in the last month prior to bariatric surgery, as documented in the medical history, were excluded. Additionally, patients with a history of viral hepatitis (Hepatitis B and C), autoimmune liver diseases, cholelithiasis, liver storage diseases such as hemochromatosis and hemosiderosis, a history of previous bariatric surgery, and patients who were taking medications such as amiodarone, tamoxifen, methotrexate, corticosteroids, valproate, and nitrofurantoin were also excluded.
Outcome
We defined the resolution of MetS as the absence of compliance with the diagnostic criteria established by the IDF-2009 6 months after surgical intervention. For the sensitivity analysis, the criteria of the Latin American Diabetes Association (ALAD) were used, which varies in the central obesity values, which are: 94 cm in men and 88 cm in women. 13
Exposure
We used the GGT/HDL-C ratio to classify the study population into tertiles. With this, we aimed to evaluate the association between this ratio and the MetS resolution in adults who underwent sleeve gastrectomy.
Other variables are described in the Supplementary Material (Supplementary Table 1).
Statistical Analysis
The database was encoded and imported into the statistical software Stata v17.0 (StataCorp, TX, USA) for analysis.
Our study employed descriptive and two bivariate analyses to characterize the population. In the first bivariate analysis, we compared independent variables with MetS resolution. For numerical independent variables with a normal distribution, the Student’s T-test was utilized. In cases where the distribution was not normal, the Mann-Whitney U test was applied. The second bivariate analysis involved categorizing the GGT/HDL-C ratio into tertiles for comparison. Here, the ANOVA test was used for numerical variables with a normal distribution, while the Kruskal-Wallis test was employed otherwise. For categorical covariates in both analyses, either Fisher’s exact test or the Chi-squared test was applied, depending on the expected values.
To address the main objective of the study, both crude (cRR) and adjusted relative risks (aRR) were calculated. This was done using generalized linear models with a Poisson family, a logarithmic link function, and robust variances. An epidemiological approach was adopted, adjusting for confounding variables like age, sex, alcohol consumption, smoking, and NAFLD (fatty liver inhibition of progression (FLIP) algorithm). Multicollinearity was assessed using the variance inflation factor, which consistently showed values below 10. Additionally, the linearity of the ‘age’ variable was examined using residual component plots (Anscombe residuals), and the potential role of ‘sex’ as an effect modifier was explored. An interaction variable was introduced into the multivariable model, but it did not show significance in the Wald test. This finding was confirmed by comparing two models, one with and one without the interaction variable, using the log-likelihood ratio test, which also indicated no significance.
A sensitivity analysis was also conducted, considering MetS resolution as the outcome but using the ALAD criteria. The regression models for this analysis followed the same guidelines as mentioned earlier. Importantly, for all scenarios, the measures of association were presented with their respective 95% confidence intervals (95% CI), and p-values <0.05 were considered statistically significant.
Results
A total of 137 patients were included in the analysis. The mean age was 38.9 ± 10.9 years, with 64.2% being female. The baseline prevalences of NAFLD, hypertension, diabetes and hypothyroidism were 86.1%, 19.7%, 11.0% and 7.3%, respectively. MetS resolution was achieved by 83.9% of the patients (Supplementary Table 2).
General characteristics of adults undergoing sleeve gastrectomy according to the tertile of the gamma glutamyl transpeptidase cholesterol/HDL-C ratio (GGT/HDL-C ratio) (n = 137).
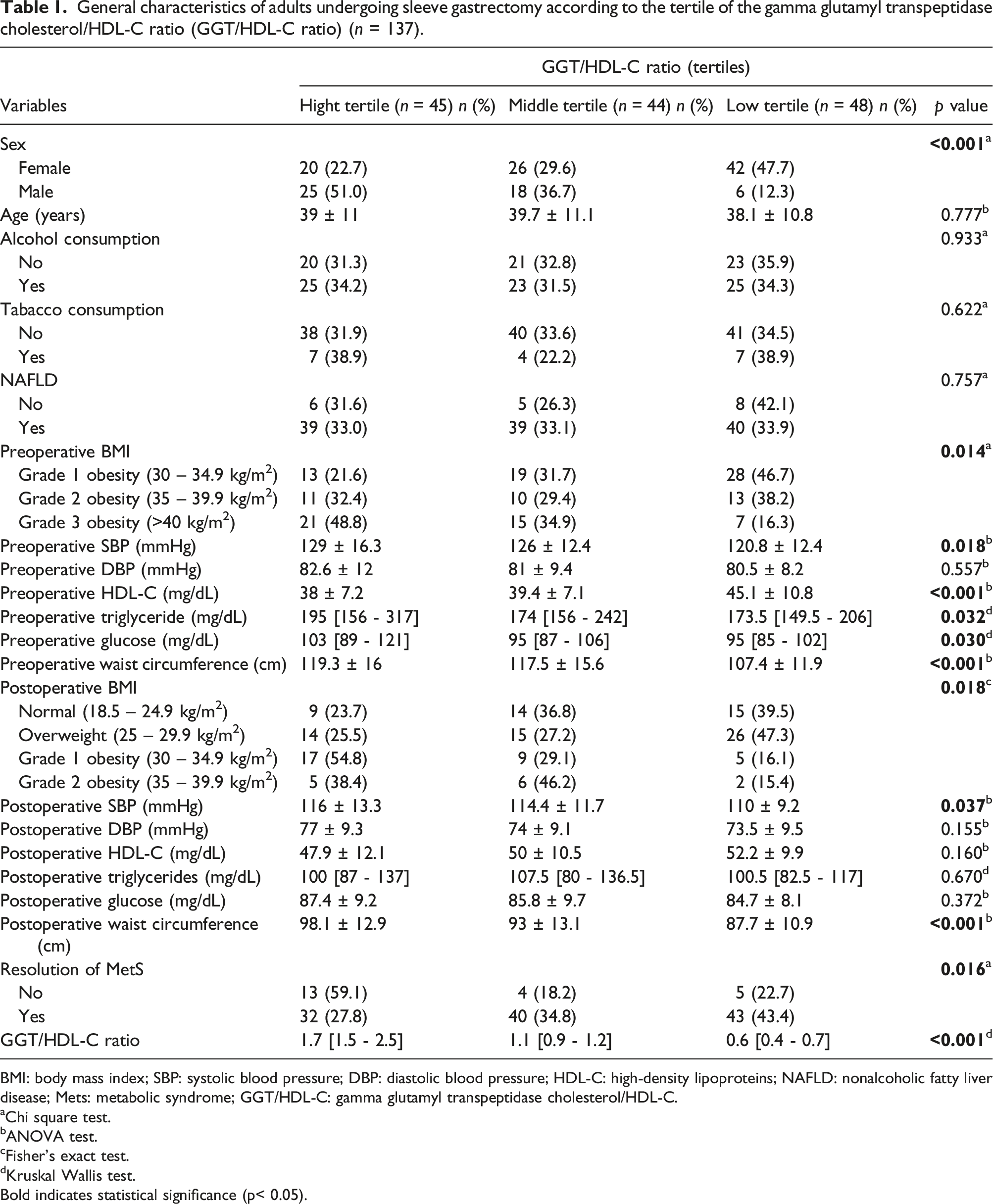
BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; HDL-C: high-density lipoproteins; NAFLD: nonalcoholic fatty liver disease; Mets: metabolic syndrome; GGT/HDL-C: gamma glutamyl transpeptidase cholesterol/HDL-C.
aChi square test.
bANOVA test.
cFisher’s exact test.
dKruskal Wallis test.
Bold indicates statistical significance (p< 0.05).
In the crude model, both the middle (cRR: 1.28; 95%CI: 1.04 - 1.58; p = .021) and the lower tertile of the GGT/HDL-C ratio (cRR: 1.26; 95%CI: 1.02 - 1.56; p = .032) were associated with MetS resolution at 6 months. After adjusting for age, sex, NAFLD, history of smoking, and alcohol consumption, the association remained significant for both the middle (aRR: 1.28; 95% CI: 1.04 - 1.58; p = .019) and lower tertiles (aRR: 1.27; 95%CI: 1.01 - 1.60; p = .038) (Table 2). There was no statistical evidence of interaction between GGT/HDL-C tertiles and sex.
Association between the GGT/HDL-C ratio and the resolution of MetS 6 months after sleeve gastrectomy.

aAdjusted for sex, age, non-alcoholic fatty liver disease (NAFLD), tobacco consumption, alcohol consumption.
bAssociation between the GGT/HDL-C ratio and the resolution of metabolic syndrome 6 months after sleeve gastrectomy, according to the criteria of the Latin American Diabetes Association (ALAD).
cRR: crude relative risk; *aRR: adjusted relative risk; CI: confidence interval.
Discussion
To our knowledge, this is the first cohort study to explore the association between the GGT/HDL-C ratio and MetS resolution within a 6-month follow-up in patients who underwent sleeve gastrectomy and were diagnosed with MetS. A key finding is that approximately 80% of patients experienced MetS resolution within 6 months post-surgery. This is consistent with existing literature, which reports significant metabolic benefits following bariatric surgery. For instance, Asian studies observed a 78% to 82% MetS resolution rate, though over a one to 4-year follow-up period post-sleeve gastrectomy and gastric bypass surgery.14,15 Similarly, a Latin American study in Mexico reported high MetS resolution rates (93%) 1-year post-surgery, maintained over 2 years. 16 These findings, coupled with ours, suggest a potential influence of genetic factors in the Latin population on MetS resolution. Notably, 43.8% of our patients had grade I obesity, potentially indicating less severe initial metabolic alterations compared to those with higher-grade obesity, thus leading to more effective post-surgical weight loss.
While the role of GGT/HDL-C ratio in MetS resolution is novel, existing studies support its utility as a predictor of cardiometabolic diseases. 17 Chinese studies have linked elevated GGT/HDL-C ratios with an increased risk of T2DM and found its predictive performance for T2DM superior to that of GGT and HDL-C individually.17,18 Furthermore, a one-unit increase in the GGT/HDL-C ratio corresponded to a 0.4% and 0.5% increase in the prevalence of NAFLD and MetS, respectively. 8
In patients with obesity, elevated GGT levels are commonly observed, 19 often due to the high prevalence of liver steatosis. 20 In the Framingham cohort study, GGT has been identified as an independent risk factor for the development of cardiovascular diseases and mortality, separate from other inflammatory markers. 21 Conversely, high levels of HDL-C are recognized as protective against cardiometabolic diseases, 22 while low levels are associated with an increased risk of MetS. 23 Both GGT and HDL-C have been identified as risk markers for MetS in previous literature.21,23 Studies report that in patients with obesity undergoing bariatric surgery, GGT levels typically decrease, 23 whereas HDL-C levels increase. 24 Moreover, metabolic complications generally show improvement over time following surgery, attributed to sustained weight loss in the medium and long term. 15
According to our hypothesis, we found that preoperative GGT/HDL-C ratio was associated with MetS resolution after 6 months of bariatric surgery. This finding supports the evidence of the usefulness of GGT/HDL-C ratio in MetS resolution, suggesting its potential utility, as it can help stratify patients and design additional interventions for those with a lower likelihood of improvement. To date, several preoperative factors have been identified as predictors of metabolic outcomes after bariatric surgery, 25 yet many of these markers face challenges in cost-effectiveness, either due to high costs or limited availability in certain regions. In contrast, the GGT/HDL-C ratio stands out as a promising, more accessible marker for monitoring MetS in bariatric surgery patients.
Our study acknowledges several limitations. Firstly, the data originated from a single center, which may limit the generalizability of our findings to other settings. Secondly, the retrospective nature of our study could introduce measurement or information bias. However, this risk is likely minimal, as the clinic where the study was conducted adheres to standardized protocols and regularly calibrates its equipment. Thirdly, the relationship between the GGT/HDL-C ratio and MetS resolution may not be uniform across all obesity categories. Therefore, future research with larger and more diverse sample sizes is necessary to validate our findings across different obesity subgroups. Fourthly, there are potential unmeasured confounding factors, such as dietary habits and physical activity levels post-surgery, which could influence the outcomes. Additionally, the absence of data on percentage weight loss and diabetes resolution limits our ability to fully evaluate the impact of bariatric surgery on these outcomes. Lastly, our study’s follow-up period was limited to 6 months, leaving the long-term stability of MetS resolution uncertain. Extended follow-up periods in future studies would be beneficial to assess the persistence of these outcomes.
In conclusion, those bariatric patients with lower GGT/HDL-C ratio values (middle and low tertiles) had a higher likelihood of achieving MetS resolution. Hence, we recommend optimizing the assessment of candidates for bariatric surgery, offering additional strategies to improve MetS components and cardiovascular risk in those with elevated GGT/HDL-C ratio values. However, it is essential to recognize the broader context of bariatric surgery’s impact beyond the resolution of metabolic syndrome. Bariatric surgery significantly contributes to health improvements across various parameters, including weight loss, reduction in HbA1c levels, decreased medication burden, and enhancement of cardiometabolic factors. These improvements collectively contribute to, for example, a lower risk of cancer and myocardial infarction, alongside an increased quality of life. Therefore, while the GGT/HDL-C ratio may provide valuable insights into potential MetS resolution, the overall evaluation of bariatric surgery candidates should encompass a holistic view of the anticipated health benefits, suggesting a more nuanced approach in the preoperative assessment to optimize patient outcomes.
Supplemental Material
Supplemental Material - Association between gamma glutamyl transpeptidase to HDL-Cholesterol (GGT/HDL-C) ratio and metabolic syndrome resolution after sleeve gastrectomy
Supplemental Material for Association between gamma glutamyl transpeptidase to HDL-Cholesterol (GGT/HDL-C) ratio and metabolic syndrome resolution after sleeve gastrectomy by Melanni L. Lizarbe-Lezama1, Jhoel E. Rodriguez-Macedo, Daniel Fernandez-Guzman, Ana L. Alcantara-Diaz, Gustavo Salinas-Sedo, and Carlos J. Toro-Huamanchumo in Diabetes & Vascular Disease Research.
Footnotes
Author contributions
Melanni L. Lizarbe-Lezama conceived and designed the experiments, analyzed the data, prepared figures and/or tables, authored or reviewed drafts of the paper, and approved the final draft. Jhoel E. Rodriguez-Macedo conceived and designed the experiments, analyzed the data, prepared figures and/or tables, authored or reviewed drafts of the paper, and approved the final draft. Daniel Fernandez-Guzman analyzed the data, prepared figures and/or tables, authored or reviewed drafts of the paper, and approved the final draft. Ana L. Alcantara-Diaz analyzed the data, prepared figures and/or tables, authored or reviewed drafts of the paper, and approved the final draft. Gustavo Salinas-Sedo conceived and designed the experiments, authored or reviewed drafts of the paper and approved the final draft. Carlos J. Toro-Huamanchumo conceived and designed the experiments, analyzed the data, prepared figures and/or tables, authored or reviewed drafts of the paper, and approved the final draft.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by CJTH is supported by the Forrest Research Foundation Scholarship and the Edith Cowan University Higher Degree by Research Scholarship.
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.