
Abstract
Objective
To determine the prevalence of metabolic syndrome and its risk factors in various ethnic groups in Istanbul, Turkey.
Methods
Study participants were aged ≥20 years. Risk factor components for metabolic syndrome were measured and its presence was determined in study participants.
Results
The study included 254 Greeks, 273 West Thracians, 275 East Turkistanis and 304 Armenians. The prevalence of metabolic syndrome was significantly different between groups (Greeks, 19.3%; West Thracians, 24.9%; East Turkistanis, 15.3%; Armenians, 20.4%), and increased with age in all groups. Low levels of high-density lipoprotein cholesterol (HDL-C) were found mainly in Greeks (females, 64.5%; males, 61.6%) and West Thracians (females, 75.8%; males, 73.1%). Among East Turkistanis, HDL-C and triglyceride levels were significantly higher compared with the other ethnic groups. Hypertension was the most frequently encountered component of metabolic syndrome in East Turkistanis.
Conclusions
The prevalence of metabolic syndrome varied between ethnic groups living in the same geographical location. In Turkey, metabolic syndrome is common. It is important to determine differences between ethnic groups, as this will assist in identifying those at higher risk of developing coronary heart disease.
Keywords
Introduction
Metabolic syndrome is characterized by the following risk factors: hypertension; hyperglycaemia; hypertriglyceridaemia; reduced high-density lipoprotein cholesterol (HDL-C) levels; abdominal obesity. 1 Abundant data suggest that, compared with other people, patients meeting these diagnostic criteria have a greater risk of having substantial clinical consequences, the two most prominent of which are the development of diabetes mellitus and coronary heart disease.1–6
The National Cholesterol Education Program (NCEP) Adult Treatment Panel III (ATP III) criteria are practical for physicians to use, since the variables defining metabolic syndrome are commonly measured in clinical practice. 6 The Third National Health and Nutrition Examination Survey (1988–1994) reported that the age-adjusted prevalence of metabolic syndrome in the USA was 23.7%, with the highest age-adjusted prevalence found among Mexican Americans (31.9%). 7 Other studies in the USA have also shown ethnic variations in the prevalence of metabolic syndrome. 8,9
The importance and prevalence of metabolic syndrome in Turkey were evaluated in the Turkish Adult Risk Factor (TEKHARF) study.10,11 Another population-based study in Turkey, which evaluated diabetes and its risk factors, was the Turkish Diabetes Epidemiology Study (TURDEP). 12
The present study determined the prevalence of metabolic syndrome and the differences in its components among people of different ethnic groups, living in the same geographical area of Turkey; these people were therefore exposed to similar environmental conditions.
Participants and methods
Study Population
All participants included in the study were male or female Turkish citizens living in specific districts in Istanbul (Zeytinburnu, Samatya and Bayrampasa), and were ≥20 years of age. Participants were recruited sequentially between January 2001 and December 2002. The study was conducted at the Department of Internal Medicine, Haseki Training and Research Hospital, Haseki, Istanbul, Turkey. Admission to the study was based solely on voluntary participation. Four fellows training in internal medicine delivered handouts explaining the study conditions via local fraternity society groups for each ethnic group. Females were excluded from the study if they were pregnant or lactating.
All participants in the study provided verbal informed consent. The study was approved by the Education Planning Commission of Haseki Training and Research Hospital (No. 2012-35).
Study Assessments
For each participant, the following parameters were measured: (i) waist circumference (cm); (ii) weight (kg); (iii) height (m). Each participant's body mass index (BMI) was calculated as weight/height 2 (kg/m2). A participant was considered to be obese if the BMI was >29 kg/m2.
After a rest period of 10 min, blood pressure (BP) was measured twice in the right arm using a sphygmomanometer with a 3-min interval between measurements, and the mean value was calculated. Blood samples were taken after a fast of >8 h. Blood was collected from the antecubital vein, stored at room temperature and analysed within 1 h after being drawn. Blood analysis was carried out at the Biochemistry Laboratories of the Haseki Teaching Hospital, using an Abbott Aeroset® analyser (Abbott Laboratories, Abbott Park, IL, USA).
Metabolic syndrome was diagnosed when a patient had at least three of the following conditions: (i) fasting plasma glucose (FPG) ≥110 mg/dl (or was receiving drug therapy for hyperglycaemia); (ii) systolic/diastolic BP (SBP/DBP) ≥130/85 mm Hg (or was receiving drug therapy for hypertension); (iii) triglycerides ≥150 mg/dl (or was receiving drug therapy for hypertriglyceridaemia); (iv) HDL-C level <40 mg/dl in males or <50 mg/dl in females (or was receiving drug therapy for reduced HDL-C); (v) waist circumference ≥102 cm in males or ≥88 cm in females (i.e. abdominal obesity).
Statistical Analyses
Data were analysed using the SPSS® software package, version 16.0 (SPSS Inc., Chicago, IL, USA) for Windows®. Data were expressed as mean ± SD and calculated prevalence. Quantitative and qualitative variables were tested using Student’s t-test and the χ2-test, respectively. A P-value <0.05 was considered to be statistically significant.
Results
Demographic and clinical characteristics according to ethnicity in males and females living in Istanbul, Turkey, recruited into a study taking place between January 2001 and December 2002.

Data are n patients or mean ± SD.
HDL, high-density lipoprotein; FPG, fasting plasma glucose; BP, blood pressure.
Quantitative and qualitative variables were tested using Student’s t-test and the χ2-test, respectively; NS, not significant (P ≥ 0.05).
P < 0.001 males versus females within same ethnic group.
P < 0.001 East Turkistanis versus West Thracians within the same sex.
P < 0.001 Greek versus West Thracians within the same sex.
P < 0.001 Armenian versus West Thracians within the same sex.
P < 0.001 East Turkistanis versus Greeks within the same sex.
P < 0.001 Armenians versus Greeks within the same sex.
P < 0.001 East Turkistanis versus Armenians within the same sex.
P < 0.05 East Turkistanis versus Greeks within the same sex.
P < 0.05 Armenians versus Greeks within the same sex.

Prevalence of the metabolic syndrome by sex in Turkish citizens of different ethnic origin (as listed on the x-axis), living in Istanbul; participants were recruited into a study between January 2001 and December 2002.

Prevalence of the metabolic syndrome in (A) males and (B) females living in Istanbul, Turkey, according to age (x-axes) and ethnicity; participants were recruited into the study between January 2001 and December 2002. There were no significant differences between the age groups in terms of the prevalence of metabolic syndrome among men or women; χ2-test.
The overall prevalence of obesity was 12.6% (32/254) in Greeks, 29.3% (80/273) in West Thracians, 17.8% (49/275) in East Turkistanis and 26.3% (80/304) in Armenians. Significant differences between the ethnic groups for obesity were as follows: Armenians versus Greeks (P = 0.011); Armenians versus West Thracians (P = 0.031); Armenians versus East Turkistanis (P = 0.004); Greeks versus West Thracians (P < 0.001); West Thracians versus East Turkistanis (P < 0.001).
Mean ± SD values for the components of metabolic syndrome according to sex for each ethnic group are given in Table 1. The following statistically significant differences were found between the sexes within the same ethnic group. Greek males had a lower mean HDL-C level and a higher mean waist circumference compared with Greek females (both P < 0.001). Armenian males had lower mean SBP and HDL-C levels, and a higher mean waist circumference, compared with Armenian females (all P < 0.001). West Thracian males had lower mean DBP and HDL-C levels, and a higher mean waist circumference, compared with West Thracian females (all P < 0.001). East Turkistani males had lower mean SBP and HDL-C levels, and a higher mean waist circumference, compared with East Turkistani females (all P < 0.001). There were no other significant differences in metabolic syndrome components between sexes within each ethnic group.
The following statistically significant differences were found in males between the ethnic groups (Table 1). In comparison with East Turkistani males, West Thracian males were older, had a higher mean triglyceride level and waist circumference, and a lower mean HDL-C level (all P < 0.001). In comparison with Greek males, West Thracian males had a greater mean waist circumference, and lower mean HDL-C and FPG levels (all P < 0.001). In comparison with Armenian males, West Thracian males were older, had a greater mean waist circumference and a lower mean HDL-C level (all P < 0.001). In comparison with East Turkistani males, Greek males had higher mean FPG and triglyceride levels, and a lower mean HDL-C level (all P < 0.001). Greek males were older, and had a higher mean FPG level and a lower HDL-C level, compared with Armenian males (all P < 0.001). Compared with East Turkistani males, Armenian males had a higher mean triglyceride level and a lower mean HDL-C level (both P < 0.001).
The following statistically significant differences were found in females between the ethnic groups (Table 1). West Thracian females had a higher mean triglyceride level, a greater mean waist circumference, a lower mean HDL-C level and a lower mean SBP compared with East Turkistani females (all P < 0.001). In comparison with Greek females, West Thracian females had a greater mean waist circumference, a higher mean DBP and a lower mean HDL-C level (all P < 0.001). In comparison with Armenian females, West Thracian females had a higher mean DBP and a lower mean HDL-C level (both P < 0.001). In comparison with East Turkistani females, Greek females had a higher mean triglyceride level, a lower mean HDL-C level and a lower mean SBP (all P < 0.05). Greek females had a lower mean HDL-C level, a smaller mean waist circumference and a lower mean SBP compared with Armenian females (all P < 0.05). Armenian females had a greater mean waist circumference, a higher mean triglyceride level, a lower mean HDL-C level and a lower mean SBP compared with East Turkistani females (all P < 0.001).
Prevalence of conditions associated with metabolic syndrome according to ethnicity, in males and females living in Istanbul, Turkey, recruited into a study taking place between January 2001 and December 2002.
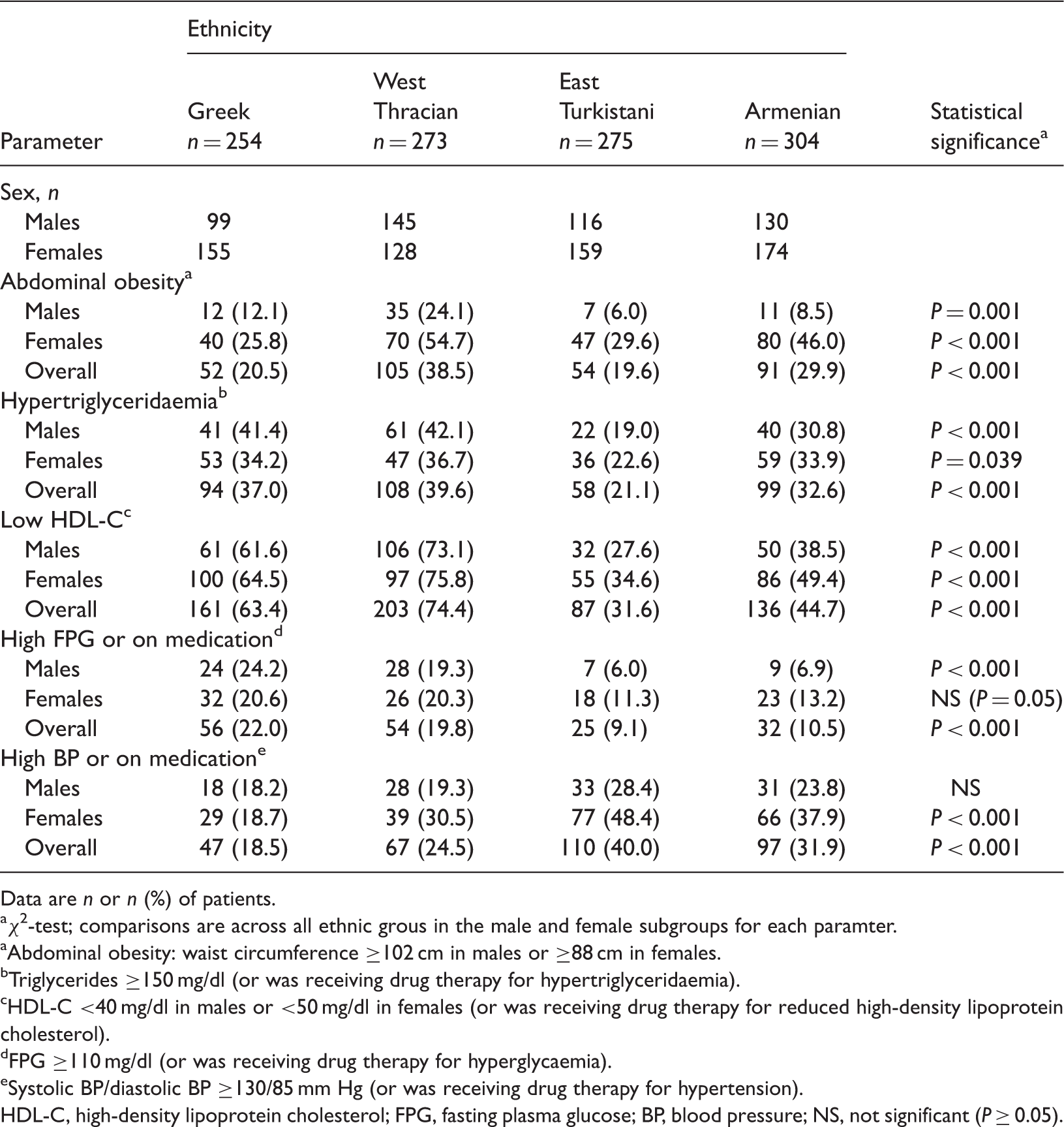
Data are n or n (%) of patients.
χ2-test; comparisons are across all ethnic grous in the male and female subgroups for each paramter.
Abdominal obesity: waist circumference ≥102 cm in males or ≥88 cm in females.
Triglycerides ≥150 mg/dl (or was receiving drug therapy for hypertriglyceridaemia).
HDL-C <40 mg/dl in males or <50 mg/dl in females (or was receiving drug therapy for reduced high-density lipoprotein cholesterol).
FPG ≥110 mg/dl (or was receiving drug therapy for hyperglycaemia).
Systolic BP/diastolic BP ≥130/85 mm Hg (or was receiving drug therapy for hypertension).
HDL-C, high-density lipoprotein cholesterol; FPG, fasting plasma glucose; BP, blood pressure; NS, not significant (P ≥ 0.05).
Discussion
Metabolic syndrome is widely recognized as an important risk factor for coronary artery disease. According to the NCEP criteria, 6 the age-adjusted prevalence of metabolic syndrome in adults (≥20 years) in the United States between 1988 and 1994 was found to be 23.7%. 7 Prevalence was found to increase with age: 6.7% in those aged 20–29 years; 43.5% in those aged 60–69 years; 42.0% in those aged ≥70 years. 7 In the TEKHARF study,10,11 using the NCEP criteria, the prevalence of metabolic syndrome was estimated to be 37% in Turkish people aged ≥30 years (9.1 million adults, of whom 5.7 million were female). These data indicate that in Turkey, metabolic syndrome affects a large number of people. The TEKHARF study also demonstrated that metabolic syndrome was prevalent in 27% of males and 43% of females. Other studies have also shown a high prevalence of metabolic syndrome in individuals living in Turkey.12–14
The present study aimed to determine the prevalence of metabolic syndrome and differences in its components among the ethnic groups living in Istanbul, Turkey. Study participants were all ≥20 years old and the prevalence of metabolic syndrome was 19.3% in Greeks, 24.9% in West Thracians, 15.3% in East Turkistanis and 20.4% in Armenians. In the ATTICA study performed in Greece,15,16 the prevalence of metabolic syndrome in Greeks was 19.8%. 16
For many centuries, Greeks and Armenians have lived in Turkey and their eating habits are similar to the indigenous population. In TURDEP, 12 which was a nationwide, cross-sectional, population-based survey in Turkey, the prevalence of obesity was 22%. The prevalence of obesity was 12.6% in Greeks and 26.3% in Armenians. Similar to the findings of TURDEP 12 and TEKHARF10,11 studies, the prevalence of obesity was higher among females compared with males in the present study. In TURDEP 12 the prevalence of abdominal obesity was 19% and in the present study it was 20.5% in Greeks and 29.9% in Armenians, with a higher prevalence in females compared with males. The present study may have identified a higher prevalence of abdominal obesity in females partly because of the different reference values that were set for the sexes (i.e. waist circumferences of ≥102 cm [males] and ≥88 cm [females]).
In the ATTICA study,15,16 the prevalence of obesity in Greeks was 20% in males and 15% in females. In the present study, the prevalence of abdominal obesity in Greeks was 12.1% in males and 25.8% in females. The difference between the present study and the ATTICA study may be explained by the different definitions of obesity used by the researchers. In the ATTICA study, obesity was defined as having a BMI >29.9 kg/m2, whereas in the present study, obesity for the purpose of defining a metabolic syndrome component was defined as having a waist circumference ≥102 cm in males and ≥88 cm in females. Thus, in the ATTICA study, the prevalence of obesity was highest in males, while in the present study it was highest in females. Abdominal obesity in the East Turkistani population in the present study was 19.6 %, with a higher prevalence in females versus males. The East Turkistani population had led a nomadic life and settled in cities after emigrating to Turkey. In the West Thracian population, which emigrated from Macedonia, abdominal obesity was 38.5% and prevalence was higher in females compared with males. The difference in abdominal obesity in West Thracians was statistically significant compared with other ethnic groups.
Social diversity may affect diet and exercise habits in all the ethnic groups. In the TURDEP study, the prevalence of hypertension was 29% and was higher in females than in males. 12 In the TEKHARF study, the prevalence of hypertension was 43.0% and was higher in females than in males (49.1% versus 36.3%).10,11 In the present study, the incidence of hypertension was 18.5% in Greeks (and was similar in both genders), but was 31.9% in Armenians and higher among females. The prevalence of hypertension was 40.0% in East Turkistanis (increasing with age) and was nonsignificantly higher in females. The prevalence of hypertension in West Thracians was 24.5% and again was higher in females. In East Turkistanis, especially in females, hypertension appeared to be the most important parameter of metabolic syndrome. Compared with data from TURDEP and the TEKHARF study, the overall prevalence of hypertension was higher in East Turkistanis and Armenians in the present study, and this was especially the case for females. In our study, 18.2% of males and 18.7% of females were defined as hypertensive, whereas in ATTICA, 37% of males and 25% of females were hypertensive. 15
It is well known that the total cholesterol levels in the Turkish population show differences compared with Western populations. 10 Even in the age group of 40–55 years, where total cholesterol was highest, total cholesterol levels in the TEKHARF study were 188 mg/dl in males and 196 mg/dl in females, which are lower rates compared with data from studies performed in Western populations.17,18 According to the TEKHARF study, one of the most important reasons for such an outcome was that HDL-C levels were <40 mg/dl in 64% of males and 36% of females.11,13 Overall, an even greater percentage of females in the present study had low HDL-C levels. The cut-off point for low HDL-C was <50 mg/dl in females, which would be expected to have resulted in a higher number of cases than those found in other studies. In the Greek and West Thracian populations, the prevalence of low HDL-C was similar to that of the general population. 10 The Greek population in the present study showed a prevalence of low HDL-C of 61.6% in males and 64.5% in females, whereas the prevalence in the East Turkistani population was lower, at 27.6% in males and 34.6% in females. In Armenians, the prevalence of low HDL-C was 38.5% in males and 49.4% in females. The East Turkistani population had the lowest prevalence of abdominal obesity, low HDL-C levels and low rates of hypertriglyceridaemia compared with the other ethnic groups. The TEKHARF study established that three out of every eight Turkish adults had metabolic syndrome, and that the presence of low HDL-C levels and hypertension in males (and obesity in females) were major contributory factors. 13 Each ethnic group in the present study had its own characteristics of metabolic syndrome.
The prevalence of metabolic syndrome in non-European groups such as South Asians, black Afro-Caribbeans, Hispanics and indigenous populations of North America and the Western Pacific Region, has been found to be relatively high. 19 Several studies have shown ethnic variations in risk factors for (and prevalence of) metabolic syndrome in groups living within the same geographical region. Study of the prevalence of metabolic syndrome among Han and Mongolian ethnic groups living in the same rural region of China revealed a high prevalence of metabolic syndrome in both groups (33.9% and 37.6% in the Han and Mongolian groups, respectively). 20 In females, the prevalence was significantly higher in Mongolians compared with Hans, however in males there was no significant between-group difference. The presence of hypertension (SBP ≥140 mmHg or DBP ≥90 mmHg) and metabolic syndrome are high in southern China; 21 with a significant inverse relationship between life stress/anxiety and diabetes, metabolic syndrome, abdominal obesity, low HDL-C levels, elevated blood glucose and elevated blood pressure (systolic BP ≥130 mmHg or diastolic BP ≥85 mmHg). The prevalence of metabolic syndrome in north-eastern China was found to be higher than in the general Chinese population, was higher in females compared with males, and gradually increased with age. 22
Ethnic differences in cardiovascular risk factors in Caucasians and South Asians with metabolic syndrome were studied and, using a logistic regression model, plasma levels of C-reactive protein and plasminogen activator inhibitor-1 were shown to be independent predictors of metabolic syndrome in Caucasians, whereas plasma levels of complement C3, tissue plasminogen activator and homeostasis model assessment of insulin resistance (HOMA–IR) were independent predictors in South Asians. 23 The prevalence of metabolic syndrome in patients with ischaemic stroke was reported to be significantly higher in ethnic South Asian patients (61%) compared with ethnic Chinese patients (47%). 24 Mean HDL was significantly lower in South Asian patients compared with Chinese patients in this study. 24
In another study, African Americans were reported to have a lower prevalence of elevated triglycerides compared with non-Hispanic whites. 25 In the latter group, there was a significant association between triglycerides and waist circumference, which was not apparent in African American females. In those with triglyceride levels <150 mg/dl, compared with white females, African American females tended to have a higher prevalence of abdominal obesity, elevated blood pressure, low HDL-C levels, and elevated FPG levels and HOMA–IR. The prevalence of high blood pressure, elevated FPG levels and HOMA–IR were all significantly higher in African American males compared with white males. The authors of this study concluded that in African Americans, the cut-off points for elevated triglycerides (and its clustering effect with other cardiometabolic risk factors on predicting risk for diabetes and cardiovascular disease) require further investigation.
In a Norwegian study in overweight and obese patients aged 6–17 years, the prevalence rates for metabolic syndrome in participants of Middle Eastern or South Asian origin were higher than in those of Norwegian origin. 26 The authors concluded that, compared with Norwegians, the ethnic minorities studied may have had an increased sensitivity to adiposity and, therefore, may have required more aggressive prevention and treatment strategies for metabolic syndrome.
When the prevalence of metabolic syndrome was assessed in children and adolescents from Brazil, Iran and Germany, 27 it was shown that there was a significantly higher prevalence of low HDL-C levels and elevated triglycerides in Iranians and Brazilians compared with Germans, and that the prevalence of metabolic syndrome was significantly higher in Iranians compared with Germans. While the prevalence of abdominal adiposity was almost similar, Iranians and Brazilians each had a noticeably higher prevalence of dyslipidaemia compared with Germans.
Whereas around 25% of the entire US population is estimated to have metabolic syndrome, a much higher prevalence is observed in Hispanic Americans (31.9%), with rates being 23.8% for Native Americans and 21.6% for African Americans. Susceptibility to central obesity and insulin resistance are thought to be major contributing factors. 28
Despite the participants in the present study being exposed to the same environmental influences by living in the same geographical area, there were significant differences in prevalence of metabolic syndrome and its various risk-factor components between the different ethnic groups. Apart from the five criteria specified by NCEP, 6 additional personal habits (such as diet and exercise) would have played a role in these differences. Since genetic make-up (which is inherited) cannot be changed, obesity as a risk factor for metabolic syndrome can be tackled, most importantly by adopting lifestyle changes such as healthy dietary intake and increased levels of physical activity. Since Turkish society has a great number of individuals with metabolic syndrome, it is important to determine the differences between ethnic groups. The common factor for metabolic syndrome between the ethnic groups was a reduced HDL-C level. In order to prevent coronary disease development and identify groups at heightened risk of disease, differences between the ethnic groups should be identified.
In conclusion, the present study, as in other studies performed in various regions, showed a high prevalence of metabolic syndrome and its related morbidities such as cardiovascular disease, obesity and dyslipidaemia. Dietary and exercise habits can demonstrate differences between the ethnic groups. When lifestyle modifications are being planned, taking into account the social and cultural diversities of ethnic groups may increase the likelihood of success in reducing metabolic syndrome.
Footnotes
Declaration of Conflicting Interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.