
Abstract
What we already know
• Physical activity is proposed to be a protective factor of type 2 diabetes mellitus (T2DM) by reversing overweight, which is a major risk factor for T2DM. • Data on the association between physical activity and T2DM risk in lean individuals are conflicting and explanations underlying this association are lacking.
What this study adds
• This study provides novel findings regarding the interactive effects of physical activity and psychological factors on lean T2DM risk.
Introduction
The global number of adults with diabetes mellitus (DM) was estimated to be 463 million in 2019 and has been projected to reach approximately 700 million by 2045. 1 The DM prevalence is relatively high in South-east Asia, which is ranked third among seven global regions. 1 However, obesity, which is the most important risk factor for type 2 DM (T2DM) and accounts for over 90% of all DM cases, is less prevalent in this region than in others. 2
Lean T2DM is defined as T2DM that develops in lean individuals with a body mass index (BMI) less than 25 kg/m2. 3 A higher prevalence of lean T2DM has been reported in Asian adults than in those of other ethnicities. 4 In an epidemiological study analyzing the German diabetes registry data, patients with lean DM exhibited a 2.5-fold higher odds ratio of mortality than those with obesity. 5 Nonetheless, only few studies have investigated the risk factors for lean T2DM.5–7
Physical activity is a well-known protective factor of T2DM, and it is important for managing blood glucose in DM patients. 8 However, previous data regarding the combined effects of BMI and physical activity on T2DM risk are inconsistent. Weinstein et al. 9 reported that physical activity was not significantly associated with T2DM risk among United States women with low BMI (<25 kg/m2) and that the protective effects of physical activity on T2DM risk were trivial, even within the overweight and obesity strata, because of the greater effects of BMI. In contrast, the EPIC-InterAct Study, which included European men and women, demonstrated that physical activity was significantly associated with T2DM risk in the <25 kg/m2 and 25–30 kg/m2 BMI strata. 10 In particular, the effects of physical activity on T2DM risk were higher in men with low BMI (<25 kg/m2) than in those in higher BMI strata. Similar findings have been observed between women with a waist circumference <80 cm and those with larger waists. The conflicting data in populations with obesity are suggested to have potentially emanated from the misclassification of physical activity levels, with such populations tending to over-report. 10 However, the reason for the inconsistency in study results regarding the association in lean individuals remains unclear.
To address the preexisting disputes regarding lean populations, psychological factors also need to be analyzed because they may play a role, in place of body weight, in the association between physical activity and T2DM risk. Previous studies have observed that psychological factors, including depression, are positively associated with T2DM risk11,12 and inversely associated with physical activity.13,14 Nevertheless, data on the association of the interactions between physical activity and psychological factors with T2DM risk are limited.
Thus, the current study aimed to investigate the associations of physical activity and psychological factors with a 10-years risk of T2DM among lean individuals. Specifically, this study calculated the participants’ daily total physical activity (TPA), which is considered to be comprehensive information on daily activities, 15 and sought to evaluate whether psychological factors modify the association between TPA and lean T2DM risk.
Methods
Study population
This study’s participants were Korean men and women aged 40–69 years who were enrolled in the population-based Ansan and Ansung cohorts of the Korean Genome Epidemiology Study. Detailed information regarding the sampling method employed and study procedures followed is available in previous reports.16,17 Approximately 1,000 male and female Korean residents of Ansan and Ansung were enrolled as cohort members. During the baseline period between June 2001 and January 2003, 9,996 members completed the on-site health examination, which included blood pressure measurement, anthropometric assessment, blood collection for biochemical and genetic assays, and a questionnaire-based interview. The questionnaire inquired about the participants’ socio-demographics, medical history and health conditions, and lifestyle factors, including physical activity. Similar examinations were conducted biennially during the follow-up period. All the procedures and protocols of this cohort study were approved by the Human Subjects Review Committee of either Korea University Ansan Hospital or Ajou University Medical Center, and written informed consent was obtained from all participants. The study datasets, which were anonymized and publicly availed for research purposes, were obtained from the Korea Disease Control and Prevention Agency. The Human Subjects Review Committee of Kookmin University (IRB approval No. KMU-201512-HR-094) approved the use of the datasets for this study.
The current study analyzed data from 1,945 cohort members who were free of DM and maintained a BMI <23 kg/m2, the cutoff point of normal BMI for Asians, 18 at baseline and through the 10-years follow-up period.
Type 2 diabetes mellitus as an outcome variable
T2DM was defined as the use of insulin or oral hypoglycemic medication or having fasting blood glucose levels ≥126 mg/dL or a 2-h post-load glucose level ≥200 mg/dL in a 75-g oral glucose tolerance test. Fasting and postprandial plasma specimens were collected in every follow-up examination for assays.
Total physical activity and psychological factors as exposure variables
Data on TPA and psychological factors obtained from the baseline questionnaire were used because questions regarding these exposures were partly changed in the follow-up questionnaires.
Participants completed a table that inquired about the time (hours) spent in a typical day on given activity categories (sleep, sedentary, very light, light, moderate, and vigorous activities), including details on specific activities corresponding to each category. Based on this information, a total metabolic equivalent (MET/h) score was calculated by multiplying hours spent by MET values (1.0, 1.5, 2.4, 5.0, and 7.5 for sleep or sedentary, very light, light, moderate, and vigorous activities, respectively), which were determined based on the activities indicated under each category. 17
The questionnaire also included questions regarding depressed mood and distress (symptoms of stress). 19 Participants were asked to answer one question on perceived depressed mood and a structured questionnaire comprising 10 items on distress. 19 The questionnaire included items regarding anxiety, response to anxiety producing situations, physical signs of stress, effects of stress on daily life, anxiety management, and the use of medications to manage stress symptoms, with the following frequency categories: none, occasional, and frequent. Using a three-point rating scale ranging from 1 (none) to 3 (frequent) for each item, distress scores were calculated.
Confounding variables
Information on other potential risk factors, such as age, sex, household income status, occupation type, educational level, marital status, family history of DM, waist circumference, smoking status, alcohol consumption, and calorie intake, was collected from the baseline data. Detailed methodological information on anthropometric measurements and dietary intake assessment is described elsewhere.17,20
Statistical analysis
The baseline characteristics of the 1,945 participants were compared across TPA quartiles (MET/h) using the Chi-square test and analysis of variance, and their descriptive statistics were calculated. The association between each activity category and TPA was analyzed using linear regression models. To analyze the associations among TPA, psychological factors, and T2DM risk, Cox proportional hazards regression analysis was used, and a hazard ratio (HR) and its 95% confidence interval (CI) were obtained. To calculate person-years, the end of the follow-up period was determined as the date of initial T2DM diagnosis, date of death, or December 31, 2012, whichever preceded. Individuals who died, withdrew from further participation, or could no longer be contacted were considered dropouts. In the multivariate models, TPA (MET-h/d quartiles), depressed mood (binary), distress score (three categories: 0–5, 6–9, and ≥10), age (continuous), sex (binary), household income status (binary: wages of <106 or ≥106 won/month), occupation type (binary: office or non-office work), educational level (binary: <9 or ≥9 years), marital status (binary: married or other status), parental history of diabetes (binary), smoking status (five categories: never smoked; former smoker; or currently smoking ≤10, 11–20, or >20 cigarettes/day), alcohol consumption status (five categories: abstained; former drinker; or alcohol consumption of <15, 15–30, or >30 g/day), waist circumference (continuous), and dietary calorie intake (quintiles) were fitted. The association between TPA and T2DM risk was evaluated, and further analyses stratified by psychological factors were conducted. Furthermore, the stratified data were analyzed in women and men separately. In the analyses, p-values for trends across the TPA quartiles were obtained. All statistical analyses were performed using The SAS program (SAS 9.4., SAS Institute, Cary, NC, USA) and evaluated at a 0.05 significance level for a two-tailed test.
Results
Characteristics of the study participants
Baseline characteristics of 1,945 study participants across quartiles of total physical activity.
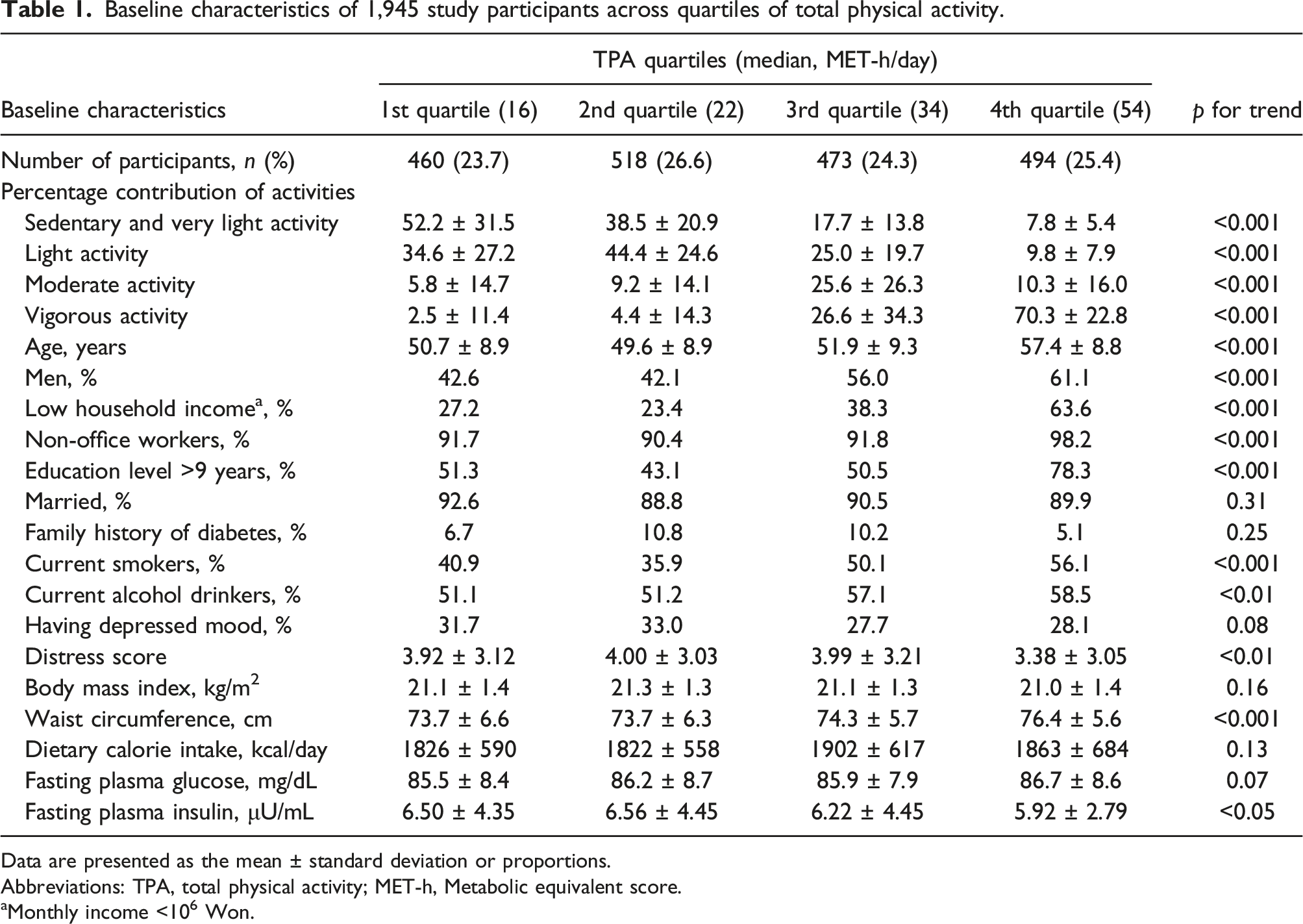
Data are presented as the mean ± standard deviation or proportions.
Abbreviations: TPA, total physical activity; MET-h, Metabolic equivalent score.
aMonthly income <106 Won.
Associations between TPA, psychological factors, and T2DM risk
Associations of total physical activity and psychological factors with 10-year incidence of lean type 2 diabetes mellitus.

Abbreviations: HR, hazard ratio; CI, confidence interval.
aAdjusted for age (continuous), sex, household income (wages of <106 or ≥106 Won/month), occupation type (office or non-office worker), educational level (<9 or ≥9 years), marital status (married or other status), smoking status (never smoked; former smoker; currently smoking; <10, 11–20, or ≥21 cigarettes/day), alcohol consumption status (lifetime abstainer; former drinker; or currently drinking; <16, 16–30, ≥31 g/day), waist circumference (continuous), MET-h/d quartiles, quartiles of dietary calorie intake, parental history of diabetes (yes or no), having depressed mood (yes or no), and distress score (0–5, 6–9, or ≥10).
Multivariate association between total physical activity and 10-year incidence of lean diabetes stratified by psychological factors.

Abbreviations: HR, hazard ratio; CI, confidence interval; TPA, total physical activity.
aAdjusted for age (continuous), sex, household income (wages of <106 or ≥106 Won/month), occupation type (office or non-office worker), educational level (<9 or ≥9 years), marital status (married or other status), smoking status (never smoked; former smoker; currently smoking; <10, 11-20, or ≥21 cigarettes/day), alcohol consumption status (lifetime abstainer; former drinker; or currently drinking; <16, 16–30, ≥31 g/day), waist circumference (continuous), MET-h/d quartiles, quartiles of dietary calorie intake, parental history of diabetes (yes or no), having depressed mood (yes or no), and distress score (0-5, 6-9, or ≥10).
The results of sex-specific analyses are shown in supplementary material (supplemental table 2). The inverse association observed between TPA and T2DM risk among participants with depressed mood was apparently influenced by the women’s data; the multivariate HR (95% CI) of T2DM risk was 0.14 (0.04, 0.56) for the 4th TPA quartile compared with the reference group (p-value for trend <0.01). In contrast, the inverse association observed between TPA and T2DM risk among participants with higher distress scores appeared to emanate from a stronger association in men; compared with the reference group, the multivariate HR (95% CI) of T2DM risk was 0.14 (0.03, 0.72) for the 4th TPA quartile (p-value for trend <0.05). Among the women, a significantly inverse association was observed between TPA and T2DM risk in the lower distress score group. The multivariate HR (95% CI) of T2DM risk was 0.23 (0.08, 0.68) for the 4th TPA quartile compared with the reference group (p-value for trend <0.05).
Discussion
The present study investigated the associations among TPA, psychological factors, and lean T2DM risk. In all the lean participants, T2DM risk was significantly associated with TPA but not with psychological factors. In particular, higher TPA significantly decreased T2DM risk in lean individuals who had depressed mood or greater distress levels rather than in those with lower distress levels. Sex-specific analyses revealed that the inverse association between TPA and T2DM was stronger in women with depressed mood and men with higher distress levels.
Based on accumulating evidence, higher physical activity decreases T2DM risk in a dose-response manner. 21 Daily movement and regular exercise have been suggested to prevent T2DM because of their beneficial effects on postprandial glycemic control. 8 In addition, higher physical activity has been reported to reduce the incidence of major complications, such as cardiovascular disease and retinopathy, among patients with diabetes 22 probably because of the associated management of body weight, blood pressure, and lipid profiles. 8 Nonetheless, data on the protective effects of physical activity on T2DM risk in lean individuals with BMI <25 kg/m2 have been inconsistent. Compared with active group, T2DM risk of the inactive group was found to be insignificant among lean women. 9 However, among lean men, the inactive group was observed to exhibit a significant 1.4-fold higher T2DM risk than the active group. 23 Even in men with BMI <23 kg/m2 who were thinner than the participants of other studies, a significantly inverse association between physical activity and T2DM risk was found. 24 Such conflicting data may result from sex differences in the prevalence of risk factors associated with T2DM risk.
Patients with diabetes reportedly tend to have psychological problems. Higher prevalence of depression has been observed in patients with diabetes versus non-diabetic adults. 25 Similarly, psychological distress is prevalent among patients with diabetes and frequently accompanied by depressive symptoms. 26 In contrast, high levels of depressive symptoms have been reported to significantly increase DM incidence risk in women but not in men. 27 Moreover, a significant association has been observed between psychological distress and T2DM risk in men but not in women. 28 Thus, psychological factors have been suggested as potential risk factors for T2DM, 29 although previous studies have yielded conflicting sex-specific results.
The biological mechanisms underlying the effects of psychological distress and depression on T2DM include dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis and the HPA-stimulated release of cortisol, which affects glucose homeostasis and potentially leads to insulin resistance. 29 Conflicting data on the association of psychological factors with T2DM between women and men may partially emanate from sex differences in HPA-axis regulation as well as the prevalence of psychological distress and depression.
Physical activity has been suggested to modify psychological factors, 14 and especially it could reduce depression symptoms in patients with diabetes. 30 However, data on the interactive effects of physical activity and psychological factors on T2DM risk, especially sex-specific data, remain limited. The current study, which focused on lean adults, found that the beneficial effects of physical activity on T2DM were greater in women with depressed mood and men with psychological distress. These findings suggest that psychological factors may act as effect modifiers in the association between physical activity and lean T2DM, and their influence may differ by sex.
This study has certain potential limitations. First, data on TPA and psychological factors were collected via simple questionnaires that potentially yielded less comprehensive information. In addition, those on the baseline exposures were used, but not updated. Thus, possible random misclassification of TPA categories and psychological factors cannot be ruled out. Second, residual confounding might have occurred in the associations, although a broad range of potential confounding factors were considered in the analysis. Notwithstanding, the current study has several strengths, including its population-based prospective design and the use of assayed blood glucose levels to ascertain T2DM cases. The study’s findings may thus be generalized to Asian populations with low or normal BMIs and similar age ranges.
In summary, this prospective study demonstrates that physical activity potentially reduces T2DM risk among lean individuals and that the beneficial effects of physical activity are more pronounced in individuals who are depressed or highly distressed. Based on this study’s findings, increasing physical activity mainly by performing exercise on a regular basis is recommended for both lean and overweight individuals to prevent T2DM.
Supplemental Material
Supplemental Material - Interactions between physical activity and psychological factors in the association with the risk of lean type 2 diabetes mellitus
Supplemental Material for Interactions between physical activity and psychological factors in the association with the risk of lean type 2 diabetes mellitus by Inkyung Baik in Diabetes & Vascular Disease Research.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation of Korea Grant funded by the Korean Government (NRF-2019R1A2C2084000).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.