
Abstract
Purpose
To investigate the impact of statin use on primary prevention of cardiovascular disease (CVD) in patients with type 2 diabetes mellitus (T2DM) in a dose-, class-, and use intensity-dependent manner.
Methods
We used an inverse probability treatment-weighted Cox hazards model, with statin use status as a time-dependent variable.
Results
Our results showed that statin use was associated with a significant reduction in CVD risk with an adjusted hazard ratio of 0.39. Pitavastatin was found to have the lowest CVD risk among the different classes of statins, followed by rosuvastatin, pravastatin, atorvastatin, simvastatin, fluvastatin, and lovastatin. Our analysis also revealed that a higher cumulative defined daily dose per year of statin was associated with a lower CVD risk. Additionally, a higher intensity of daily statin dose was associated with a lower CVD risk in patients with T2DM.
Conclusion
This study highlights the importance of statin use in reducing the risk of CVD in patients with T2DM, and the significance of dose, class, and intensity of statin use, in particular, pitavastatin class of statins was found to be the most effective in primary prevention of CVD in T2DM.
Keywords
Key points:
Introduction
In 2021, the International Diabetes Federation Atlas reported that approximately 537 million adults worldwide had diabetes. 1 In 2022, the Centers for Disease Control and Prevention’s Diabetes Surveillance System estimated that about 11.3% of adults, equivalent to 37.3 million people, had diabetes, with 8.5 million remaining undiagnosed. Of this population, 95% had type 2 diabetes (T2DM).2,3 Patients with overt diabetes face an increased risk of cardiovascular disease (CVD), which is linked to the severity of hyperglycemia. 4 Numerous studies, including a meta-analysis of 13 cohort studies, demonstrate this link. 4 Even after accounting for factors like age, hypertension, smoking, hypercholesterolemia, and left ventricular hypertrophy, diabetes remains an independent CVD risk factor. 5
In the context of primary prevention of CVD in T2DM patients, the rationale for reducing low-density lipoprotein cholesterol (LDL-C) is well-established. Observational and clinical trial evidence supports the idea that lower LDL-C levels reduce CVD risk. While clinical trials do not specify precise LDL-C targets, they do show that statin therapy can reduce relative CVD risk by approximately 30%. 6 As the global T2DM population continues to grow, so does the associated CVD risk.1–5 Yet, no randomized controlled trial has explored the use of statins for primary CVD prevention in T2DM patients without prior CVD. Existing studies on primary CVD prevention with statins have yielded mixed results, with little focus on T2DM patients. 7 Thus, additional epidemiological evidence is essential to assess the impact of statin dose, class, and use intensity in primary CVD prevention for T2DM patients.
Our study aims to address this gap by utilizing real-world data to estimate the effects of statin dose, class, and use intensity on the primary prevention of CVD in T2DM patients without prior CVD.
Methods
Study population
We conducted a population-based cohort study using data from Taiwan's National Health Insurance Research Database (NHIRD), which includes comprehensive medical claims, demographics, and vital status information. 8 The study focused on patients with type 2 diabetes (T2DM) aged ≥40 from 2008 to 2020, excluding those with missing age data and those who switched statin classes during the follow-up period (1). Statin users were defined as those prescribed statins for >1 month annually, with a mean dose of ≥28 cumulative defined daily doses (cDDDs). 8 The observation period extended until CVD occurrence, death, or December 31, 2021. 8
Study covariates
To adjust for potential confounders, patients were categorized into age groups, and analyses adjusted for age, sex, income, urbanization, types of antidiabetic drugs, diabetic severity, comorbidities, smoking, alcoholic liver diseases, and Charlson comorbidity index scores using inverse probability treatment-weighted (IPTW) Cox regression models (Supplemental Table 1). 9 Comorbidity data were extracted from medical records within 1 year before the index date. 9
Exposure to statins
Statin exposure was coded using the Anatomical Therapeutic Chemical (ATC) classification system. 10 Lipophilic and hydrophilic statins were analyzed as major exposures, and the intensity of statin use was based on average daily doses. 10
Statistical analysis
Time-dependent Cox hazard models were used to compare CVD risk between statin users and nonusers, and the study considered statin prescriptions every 3 months to define user status as a time-dependent variable. The study examined the effect of various statins on CVD risk and performed subgroup analyses with similar results. Statistical analyses were conducted using SAS version 9.4 (SAS Institute, Cary, NC, USA).
Results
Among patients diagnosed with T2DM between 2008 and 2020, our analysis encompassed 187,702 individuals, with an equal split between statin users and nonusers (93,851 each). The average age at T2DM diagnosis was 52.00 years for both groups. Notably, atorvastatin was the most commonly prescribed statin (33.29%), followed by simvastatin (21.59%) and rosuvastatin (17.13%) (Supplemental Table 1). Post-matching, absolute standardized mean differences (ASMD) for all baseline covariates were below 0.1 after using IPTW, indicating balanced covariates between statin users and nonusers.
In terms of the association with CVD, 38,757 statin nonusers (41.30%) and 27,867 statin users (29.69%) developed CVD, with an adjusted hazard ratio (aHR) for statin users of 0.39 (95% CI = 0.38–0.39). Notably, various statins displayed significantly reduced risks of CVD among statin users, with aHRs ranging from 0.06 to 0.71 (Supplemental Table 2). The log-rank test showed significant differences in CVD risk between users of different statin classes (Figure 1). Kaplan–Meier of cumulative curves of primary cardiovascular disease for different classes of statins in patients with T2DM.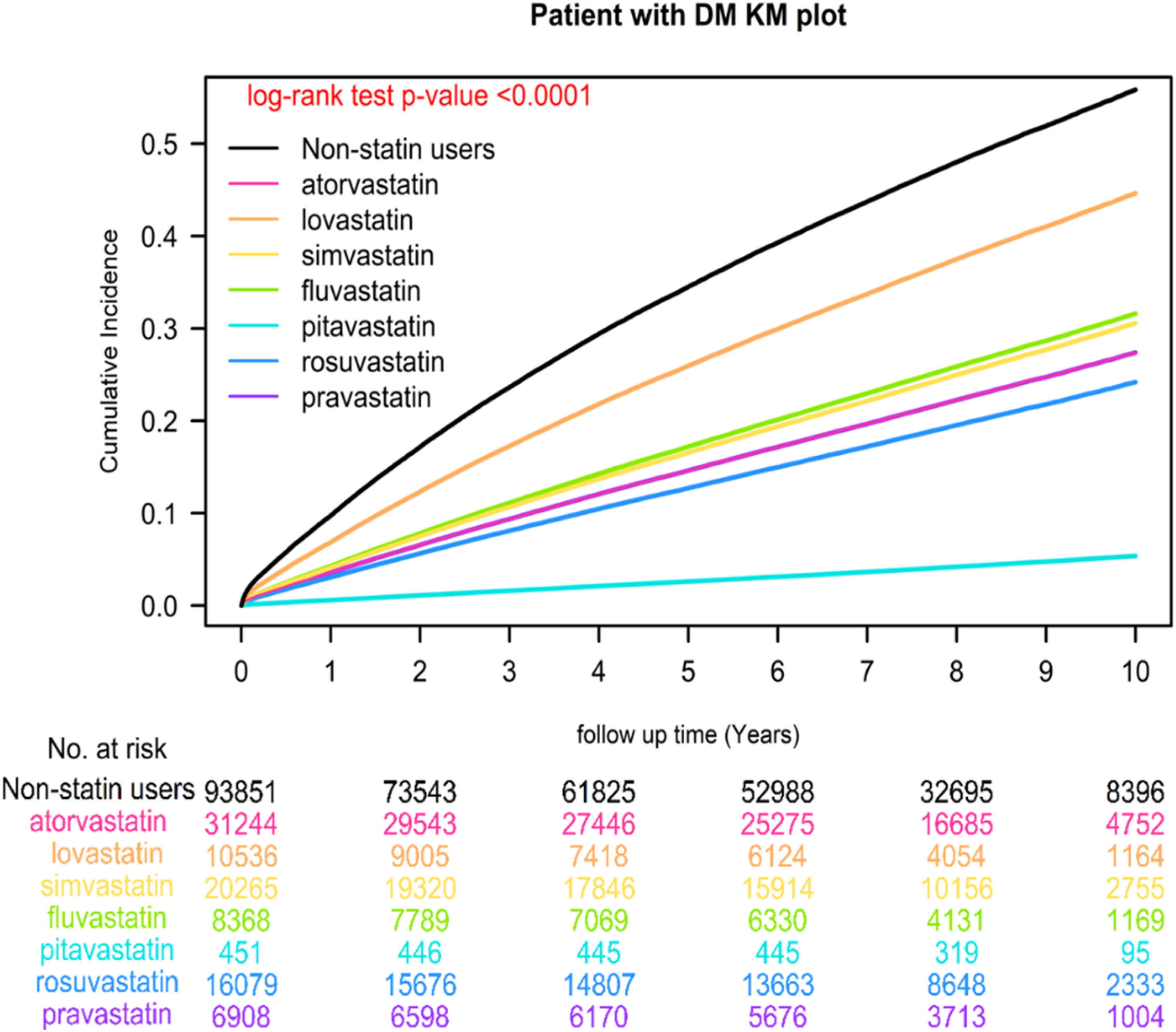
IR and IRRs for primary cardiovascular disease.
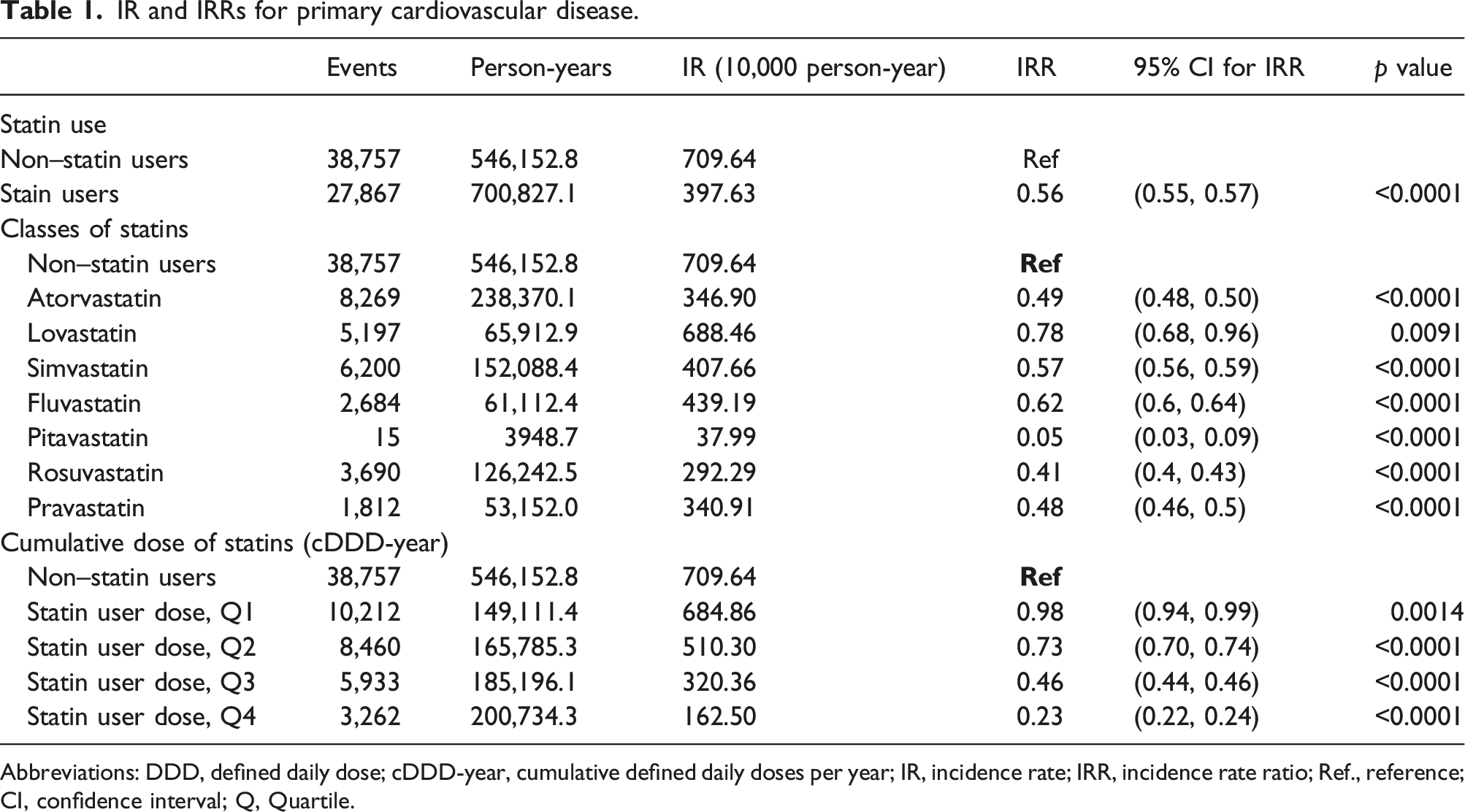
Abbreviations: DDD, defined daily dose; cDDD-year, cumulative defined daily doses per year; IR, incidence rate; IRR, incidence rate ratio; Ref., reference; CI, confidence interval; Q, Quartile.
Discussion
In this comprehensive study, we undertook the most extensive and long-term analysis of its kind, covering a mean follow-up duration of 9 years. Our findings unequivocally support the protective effects of statin use against the primary prevention of CVD in individuals with T2DM. Importantly, this study stands out as the first to explore the impact of different classes of statins on CVD prevention, offering a hierarchy of their effects in this patient population: pitavastatin > rosuvastatin > pravastatin > atorvastatin > simvastatin > fluvastatin > lovastatin. This hierarchy aligns closely with the known potency of these statins in terms of lipid profile improvements, including their effects on LDL-C, HDL-C, and triglyceride levels.
Prudent management of T2DM often necessitates multiple medications, making the potential for drug interactions a matter of concern. Statins that exhibit fewer drug interactions, such as pitavastatin and pravastatin, or those with potent lipid profile-improving effects, notably rosuvastatin, may be particularly well-suited for individuals with T2DM seeking to prevent CVD. 11 Surprisingly, evidence regarding the effects of statin intensity has been relatively scarce. While one trial from 2018 found no significant difference between more- and less-intensive statin therapy based on LDL-C targets, 12 our study indicates a correlation between higher statin intensity (defined by DDDs) and a greater reduction in CVD risk among T2DM patients. Nonetheless, due to limited data on patients prescribed higher doses, our analysis couldn't definitively evaluate the protective effects of extremely high doses compared to other DDDs.
Another uncharted territory was the impact of cumulative doses of statins on primary CVD prevention in patients with T2DM. Our results pointed to a direct relationship, where higher cumulative doses (cDDD-year) of statin therapy were associated with a lower risk of CVD. While the magnitude of our study's strengths lies in its sizable sample size, offering reliable real-world evidence with long-term follow-up, several limitations should be acknowledged. Notably, our use of claims data prevented the analysis of individual blood and lipid profiles, limiting our ability to establish associations between lipid profile changes after statin initiation and CVD risk. Furthermore, potential unmeasured confounders could have influenced our findings, despite our efforts to mitigate bias through various analyses. Additionally, the lack of data on body mass index and other lifestyle factors at the index date hindered the assessment of their contributions to CVD incidence. Lastly, the majority of our study population comprised individuals of Han Chinese ethnicity, primarily Taiwanese residents, limiting the generalizability of our results to other ethnic groups and countries.
Conclusion
In patients with T2DM, our real-world evidence demonstrates that statin use yields a dose-, class-, and use intensity-dependent reduction in CVD risk, with pitavastatin exhibiting the most robust preventive effect, followed by rosuvastatin, pravastatin, atorvastatin, simvastatin, fluvastatin, and lovastatin. These findings underscore the utility of statins in primary CVD prevention for T2DM patients and provide novel insights derived from a large-scale national database analysis, paving the way for informed clinical decision-making and improved strategies in this context.
Supplemental Material
Supplemental Material - Optimizing statin therapy for primary prevention of cardiovascular disease in type 2 diabetes mellitus patients: Exploring dose, class, and intensity
Supplemental Material for Optimizing statin therapy for primary prevention of cardiovascular disease in type 2 diabetes mellitus patients: Exploring dose, class, and intensity by Jung-Min Yu, Wan-Ming Chen, Ben-Chang Shia and Szu-Yuan Wu in Diabetes & Vascular Disease Research.
Footnotes
Acknowledgments
Lo-Hsu Medical Foundation, LotungPoh-Ai Hospital, supports Szu-Yuan Wu’s work (Funding Number: 110908, 10909, 11001, 11002, 11003, 11006.
Author contributions
Conception and Design: Jung-Min Yu; Wan-Ming Chen; Ben-Chang Shia; Szu-Yuan Wu, Collection and Assembly of Data: Szu-Yuan Wu. Data Analysis and Interpretation: Wang-Ming Chen; Jung-Min Yu; Ben-Chang Shia; Szu-Yuan Wu. Administrative Support: Szu-Yuan Wu. Manuscript Writing: Szu-Yuan Wu; Jung-Min Yu. Final Approval of Manuscript: All authors. Administrative Support: Szu-Yuan Wu ![]()
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Lo-Hsu Medical Foundation, LotungPoh-Ai Hospital, supports Szu-Yuan Wu’s work (Funding Number: 10,908, 10,909, 11,001, 11,002, 11,003, 11,006, and 11,013).
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.