
Abstract
Type 2 diabetes individuals are at high risk for macrovascular complications: myocardial infarction, stroke and cardiovascular mortality. Recent cardiovascular outcome trials have demonstrated that agents in two antidiabetic classes (SGLT2 inhibitors and GLP-1 receptor agonists) reduce major adverse cardiovascular events. However, there is strong evidence that an older and now generically available medication, the thiazolidinedione, pioglitazone, can retard the atherosclerotic process (PERISCOPE and Chicago) and reduce cardiovascular events in large randomized prospective cardiovascular outcome trials (IRIS and PROactive). Pioglitazone is a potent insulin sensitizer, preserves beta-cell function, causes durable reduction in HbA1c, corrects multiple components of metabolic syndrome and improves nonalcoholic fatty liver disease/nonalcoholic steatohepatitis. Adverse effects (weight gain, fluid retention, fractures) must be considered, but are diminished with lower doses and are arguably outweighed by these multiple benefits. With healthcare expenses attributable to diabetes increasing rapidly, this cost-effective drug requires reconsideration in the therapeutic armamentarium for the disease.
Background
Type 2 diabetes mellitus (T2DM) is a cardiometabolic disease1,2 that affects both the microvasculature (retinopathy, nephropathy, neuropathy) and macrovasculature [myocardial infarction (MI), stroke]. The microvascular complications primarily are related to the level of glycaemic control,3,4 whereas hyperglycaemia is a relatively weak risk factor for the macrovascular complications3,5 which represent the major cause of mortality in T2DM patients.6,7 Long-term cardiovascular (CV) outcome trials have generally demonstrated no or only slight reduction in CV events with intensive glycaemic control.3,8–10 In contrast, treatment of more traditional CV risk factors (blood pressure, dyslipidaemia) consistently has been associated with major CV benefits in T2DM patients. 1
The results of recent CV outcome trials have documented that glucose-lowering agents in two different classes significantly reduce the MACE (major adverse cardiovascular events) endpoint (composite of CV mortality, non-fatal MI, non-fatal stroke). In both the EMPA REG OUTCOME trial 11 and in the CANVAS program, 12 the sodium glucose transporter-2 (SGLT2) inhibitors, empagliflozin and canagliflozin, reduced MACE by 14% and 13%, respectively, although the relative contributions of the three individual components of the composite outcome differed. In LEADER 13 and SUSTAIN-6, 14 therapy with the glucagon-like-peptide receptor agonists (GLP-1 RAs), liraglutide and semaglutide, resulted in reductions in MACE of 13% and 26%, respectively, and also with differential contributions from the composite elements. Importantly, empagliflozin and liraglutide were each associated with significant reductions in CV mortality as well. With the robust results of these large, long-term, CV outcome trials, we are entering a new era of T2DM treatment where glucose-lowering drugs that address both glycaemia, as well as CV risk, are now preferred in patients with cardiovascular disease (CVD) over those therapies that simply lower HbA1c. 15
In the midst of the newfound interest in the SGLT2 inhibitors and GLP-1 RAs, the established anti-atherogenic benefits of the thiazolidinedione (TZD), pioglitazone, have been overlooked. 16 The recent results of the IRIS (Insulin Resistance Intervention after Stroke) trial 17 should rekindle interest in pioglitazone as a cardioprotective drug, an effect which actually was established more than a decade ago. Because pioglitazone is now generically available, it represents a more affordable option than either an SGLT2 inhibitor or a GLP-1 RA. 18 Furthermore, it can be combined with these and other glucose-lowering agents, including the SGLT2 inhibitors or GLP-1 RAs, to minimize side effects.15,18–20 Pioglitazone also has a number of other demonstrated benefits, including amelioration of insulin resistance, preservation of beta-cell function, durable glycaemic control, improvement of multiple factors of the metabolic syndrome and reversal of hepatic steatosis [nonalcoholic fatty liver disease (NAFLD)]/nonalcoholic steatohepatitis (NASH) making it an attractive option for the treatment of many patients with T2DM, particularly those at risk for CV events. In this review, we examine the CV, glycaemic and other metabolic benefits of pioglitazone and provide strategies to maximize the drug’s benefit: risk ratio.
CV benefit
A substantial body of evidence, including large randomized prospective CV outcome trials,16,17,21–23 real-world observational studies24–26 and smaller studies of regression of coronary atherosclerosis 27 and carotid intima thickness, 28 has demonstrated that pioglitazone reduces both atheroma progression and related CV events. These investigations were initiated because of a substantial literature dating back many decades that has linked insulin resistance to premature coronary heart disease (CHD). 29 These data begged the question as to whether reducing insulin resistance with an insulin-sensitizing drug would provide a CV benefit. The question is also of historical importance, since the notion that a diabetes drug could reduce CV events had eluded investigators for years. In PROactive, 5238 T2DM patients with a prior CV event were randomized to pioglitazone or placebo and followed for a mean of 2.9 years. 16 Although the primary endpoint, a broad composite that included leg revascularization procedures, fell short of statistical significance [hazard ratio (HR) = 0.90, p = 0.09], the ‘main secondary endpoint’, MACE, was significantly reduced (HR = 0.84, p = 0.027) (Figure 1), on par with the effect size in the aforementioned recent positive trials of newer glucose-lowering agents.11–15 In PROactive participants with a prior MI (n = 2445) or prior stroke (n = 948) pioglitazone therapy were associated with robust 28% and 47% reductions in recurrent MI 30 and recurrent stroke, 31 respectively. The primary endpoint in PROactive 16 should be interpreted in the context that leg revascularization historically has not been included as an endpoint in CV outcome trials since it is refractory to antihypertensive, lipid-lowering and glucose-lowering therapy.32,33 Consistent with PROactive, a meta-analysis of published pioglitazone studies and reported to the Food and Drug Administration (FDA) demonstrated a 25% reduction in CV events.21,22
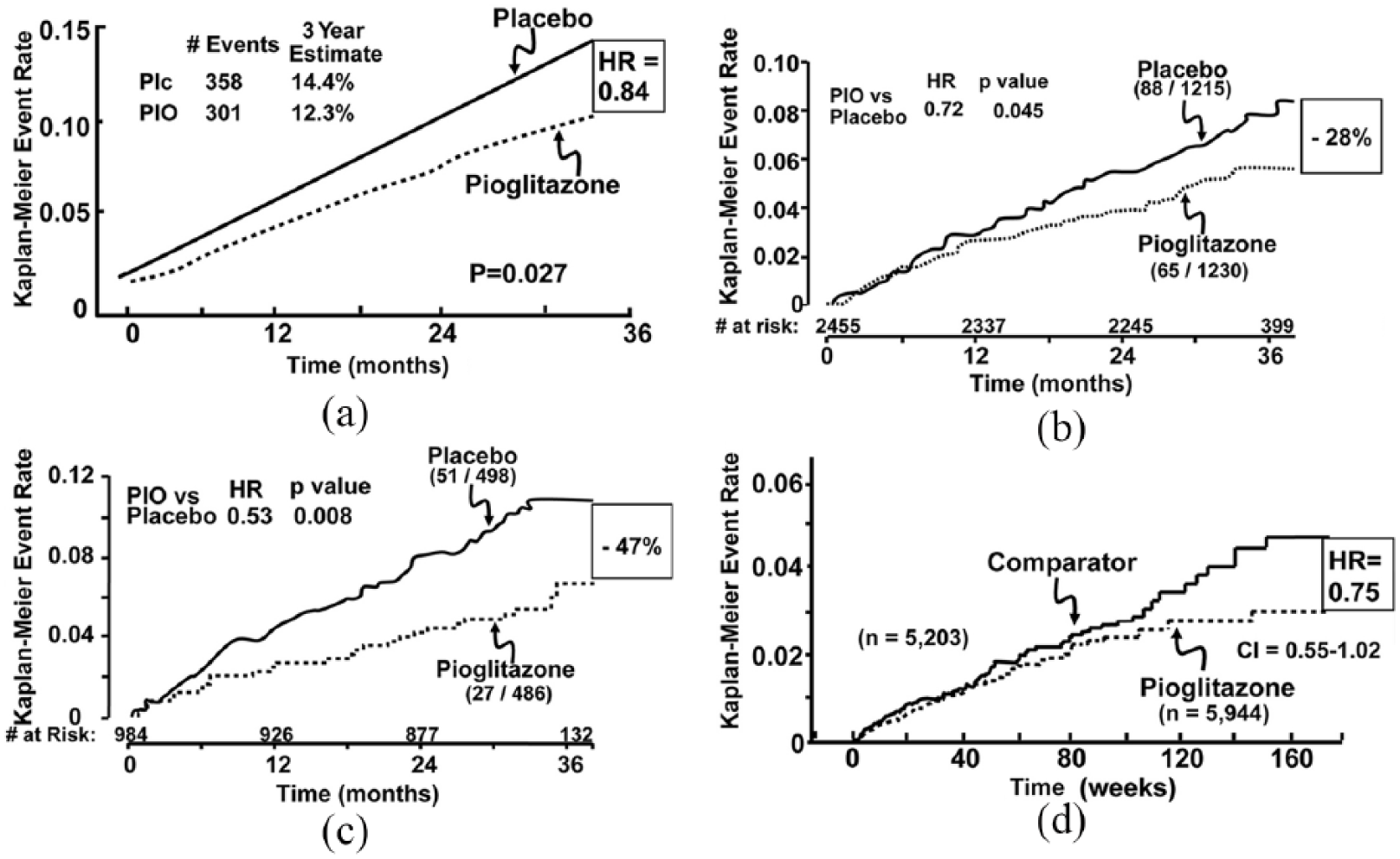
(a) Kaplan–Meier plot of time to MACE endpoint (cardiovascular mortality, non-fatal MI, non-fatal stroke) in T2DM patients treated with pioglitazone (PIO) or placebo (Plc) in PROactive. Redrawn with permission from Dormandy et al. 16 (b) Pioglitazone reduces recurrent MI in diabetic patients with a previous MI in PROactive. Redrawn with permission from Erdmann et al. 30 (c) Pioglitazone reduces recurrent stroke in diabetic patients with a previous stroke in PROactive. Redrawn with permission from Wilcox et al. 31 (d) Meta-analysis of all published studies (excluding PROactive) in which the effect of pioglitazone versus placebo or active comparator on cardiovascular events is examined. Redrawn with permission from Lincoff et al. 21
Based upon (1) evidence that insulin resistance was a strong risk factor for stroke as well CHD, 2 (2) the consistently positive results observed in these CV outcome trials,16,17,21,22,24–28 and (3) the reduction in recurrent stroke (by 47%) and MI (by 28%) in T2DM individuals in PROactive, 16 the National Institutes of Health initiated the IRIS study. 17 In 3876 non-diabetic, insulin-resistant individuals with a recent transient ischaemic attack (TIA) or stroke, pioglitazone reduced fatal/non-fatal stroke or MI by 24% (p = 0.007) over a mean of 4.8 years (Figure 2). 17 In a follow-up report from this study, 34 pioglitazone reduced the risk of any stroke by 25% (p = 0.01) and decreased the risk of acute coronary syndrome by 29% (p = 0.02), with most of the drug’s effects on type 1 MIs (HR = 0.62, p = 0.03), particularly large infarcts (HR = 0.44, p = 0.02). 35 These results compare favourably with results obtained with aspirin and anti-platelet drugs,36–38 as well as with statins, 39 which are now widely used for stroke prevention.36–38 Notably, the positive beneficial CV effects of pioglitazone in all of these studies occurred on the background of widespread use of evidence-based CV therapies including anti-platelet agents suggesting that pioglitazone can effectively address ‘residual CV risk’.
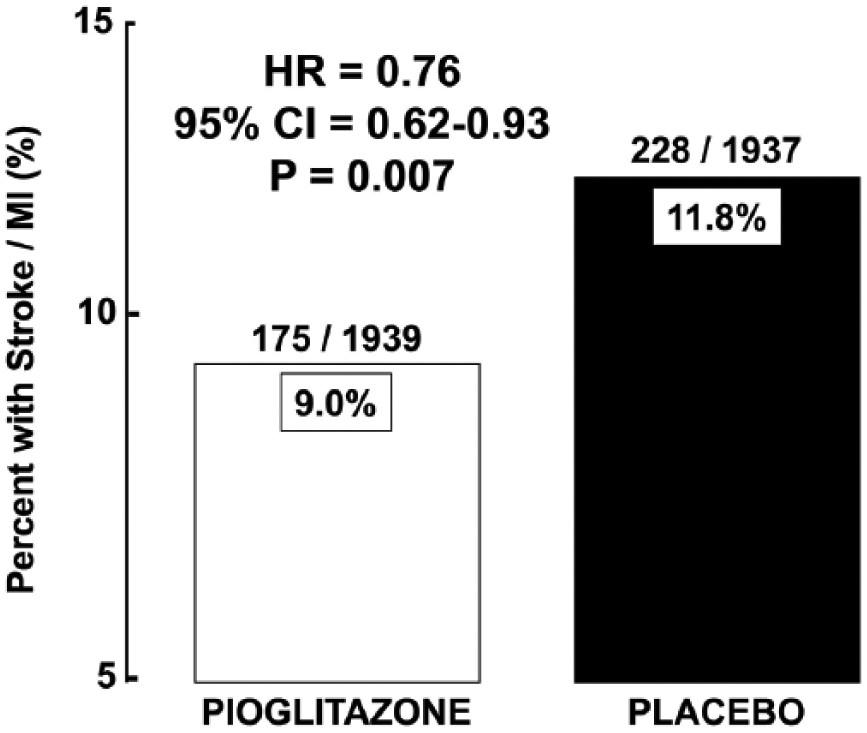
Effect of pioglitazone versus placebo on recurrent stroke and myocardial infarction in the Insulin Resistance Intervention after Stroke (IRIS) study. Drawn from the data in Kernan et al. 17
Observational ‘real-world’ data also support the CV benefits of pioglitazone. For example, a retrospective analysis of 91,511 patients in the UK Research General Practice Database (GPRD) who were followed for 7.1 years demonstrated that pioglitazone decreased all-cause mortality by 39% compared with metformin. 40 In a separate analysis of 27,457 GPRD patients who had a second agent added to metformin monotherapy, pioglitazone therapy was associated with a significantly decreased HR for all-cause mortality (HR = 0.71) and the combined endpoint of all-cause mortality/major adverse CV events (HR = 0.75). 24 In a more recent observational study, 25 pioglitazone significantly reduced both CV (HR = 0.58) and non-CV (HR = 0.63) mortality in a large (n = 62,266) European cohort of diabetic patients. In a study which compared 56,536 patients with T2DM who were first-time users of pioglitazone or insulin, propensity scores showed a 67% reduction in all-cause mortality in favour of pioglitazone. 26 In a meta-analysis of nine randomized controlled trials, pioglitazone significantly reduced the risk of major CV events in patients with diabetes [HR = 0.83, 95% confidence interval (CI) = 0.72–0.97] and prediabetes or insulin resistance (HR = 0.77, 95% CI = 0.64–0.93). 41 The results of this meta-analysis are consistent with a previous one by Lincoff et al. 21 Finally, consistent with the IRIS study, another retrospective study from the UK using Clinical Practice Research Datalink (CPRD) found a HR of 0.63 for incident stroke in T2DM patients who were users of pioglitazone versus other glucose-lowering drugs. 42
Smaller mechanistic studies are consistent with the findings from these large prospective and observational studies and meta-analyses. In the PERISCOPE study, pioglitazone, compared with glimepiride, retarded the progression of coronary atherosclerosis as measured by intravascular ultrasound (IVUS), 27 while in the CHICAGO study, pioglitazone slowed the rate of increase in carotid intimal thickness, a surrogate measure of atherosclerosis. 28 Pioglitazone has been shown to reduce intracoronary plaque volume in non-diabetic 43 and type 2 diabetic 44 subjects and to prevent restenosis after stent placement. 45
One negative pioglitazone study to consider is the recent CV outcome trial from Italy, TOSCA-IT. 46 A total of 3041 T2DM patients with suboptimal glycaemic control on metformin monotherapy were randomized to either pioglitazone or a sulphonylurea and followed for a mean of 4.8 years. Because only 11% had a prior history of CVD, this was essentially a primary prevention population. The primary outcome (all-cause death, non-fatal MI, non-fatal stroke and urgent coronary revascularization) occurred at a similar frequency between the two groups: pioglitazone 6.8% versus sulphonylurea 7.2% (HR = 0.96, p = 0.40). Unfortunately, the study had some methodological limitations, including its unblinded design and the fact that many patients in the pioglitazone arm had either terminated their participation early (10%) or had stopped the study drug (28%), likely stemming from controversy about the drug’s safety that had arisen during the trial. Furthermore, the CV event rate, 1.5 per 100 person years, was very low, rendering the study greatly underpowered to detect any effective CV events. This issue was underscored by an a posteriori per-protocol analysis focusing on just those patients taking their study drug. Here, a secondary outcome that included peripheral vascular events was significantly reduced by study drug (HR = 0.67, p = 0.03). Of course, this outcome must be interpreted cautiously.
In summary, a large body of evidence from clinical trials to observational studies to mechanistic investigations document that pioglitazone effectively prevents recurrent CV events in both diabetic and non-diabetic individuals, most likely through a beneficial effect on atherosclerosis. The only negative study to our knowledge, TOSCA-IT, involved patients generally without CVD and had multiple interpretative challenges.
Appropriate concern has been raised about ‘heart failure’ (HF) in PROactive. Due to increased renal sodium retention, all TZDs are associated with oedema, 47 which is a nonspecific sign of HF by clinicians. Since the HF cases in PROactive were not adjudicated, it remains possible that at least some of the excess events may have reflected cases of oedema without cardiac decompensation. HF is typically an ominous diagnosis in patients with diabetes, with a 5-year mortality in excess of 50%.1,45 Given that mortality in this cohort of individuals with HF in PROactive was decreased (not increased), albeit not significantly, it is possible even likely that not all (probably many) patients diagnosed with HF actually had HF. In fact, in smaller trials, pioglitazone has been demonstrated to have no deleterious effect on left ventricular (LV) function,48,49 to actually improve diastolic dysfunction,48–50 to reduce blood pressure,48,49 and to increase myocardial insulin sensitivity.48,49 Interestingly, prior to the concern about HF, observational data suggested that this drug class might actually decrease mortality after HF admissions. 16 Thus, participants in PROactive who were diagnosed with HF did not experience any increase in CV events compared to placebo-treated individuals. 16 In IRIS, HF was not increased, although this cohort of cerebrovascular patients had less CHD than did participants in PROactive.17,51 Also, the IRIS protocol allowed for dose reductions in the setting of significant weight gain or oedema. These observations are consistent with previous findings that pioglitazone improves diastolic function in diabetic rats 52 and humans48,53 by positively influencing matrix remodelling.52,53 A recent meta-analysis suggests that pioglitazone also reduces both new onset and recurrent atrial fibrillation by 27%. 54
Metabolic effects of pioglitazone
The insulin resistance syndrome (IRS), originally referred to as the metabolic syndrome, comprises a cluster of cardiometabolic disorders, each representing an independent CV risk factor. 2 Pioglitazone improves each component of the IRS (Table 1) (reviewed in previous studies2,55–58). It enhances insulin sensitivity and effectively reduces plasma glucose levels and HbA1c while also lowering blood pressure and having a favourable effect on the plasma lipid profile. The latter includes a reduction in triglycerides and free fatty acids (FFAs), increase in high-density lipoprotein (HDL) cholesterol and conversion of small dense low-density lipoprotein (LDL) particles to larger, more buoyant, less atherogenic ones. The drug also shifts fat from visceral abdominal depots, from liver and from skeletal muscle to subcutaneous abdominal depots,59–62 thereby ameliorating lipotoxicity.2,55,63–66 It normalizes adipocytokine secretion, especially adiponectin, improves endothelial dysfunction and reduces circulating concentrations of the procoagulant plasminogen activator inhibitor-1 and the pro-inflammatory mediator C-reactive protein (CRP).66,67 Although pioglitazone improves multiple CV risk factors, both preclinical68–70 and clinical16,17,21–23,27,28,71, data suggest that pioglitazone exerts direct anti-atherogenic effects on the arterial wall.
Effect of pioglitazone on established CV risk factors.
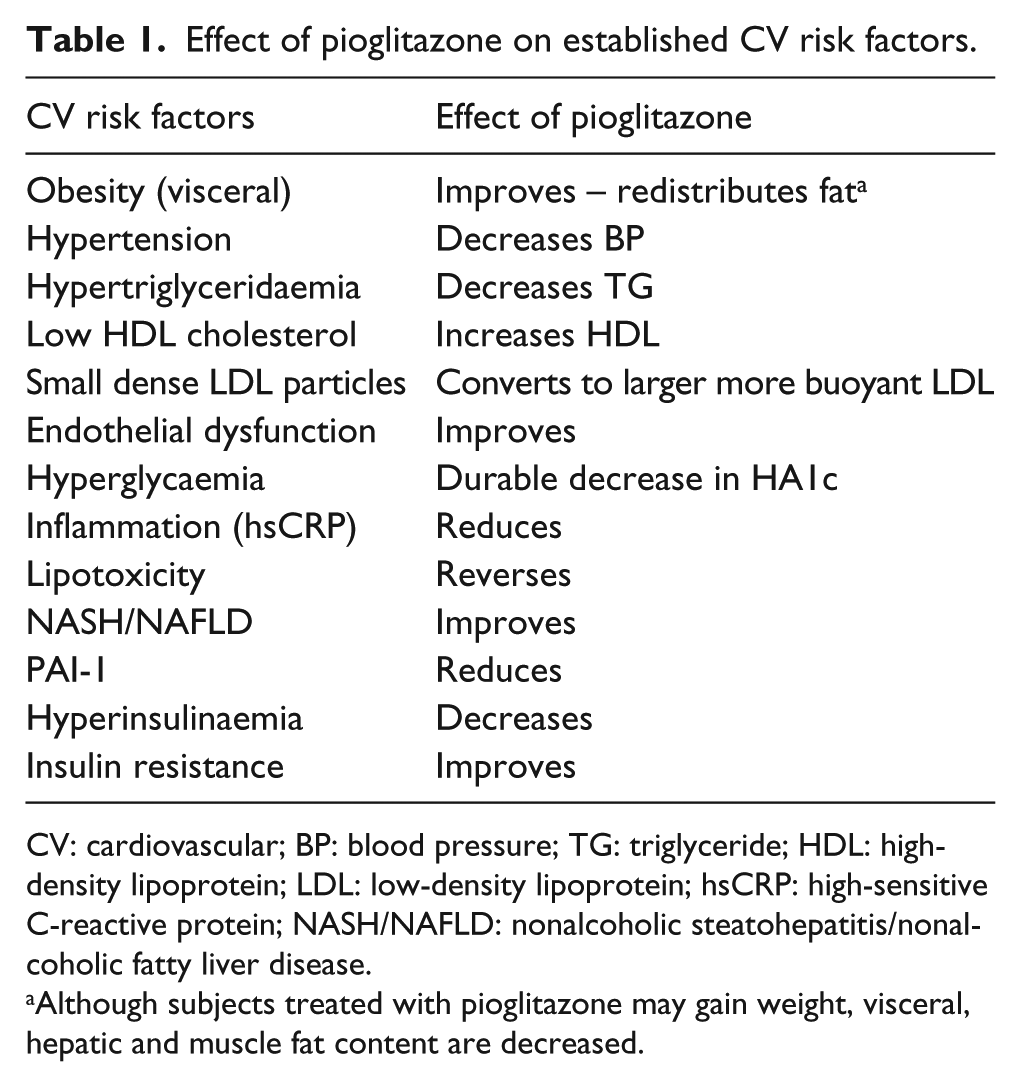
CV: cardiovascular; BP: blood pressure; TG: triglyceride; HDL: high-density lipoprotein; LDL: low-density lipoprotein; hsCRP: high-sensitive C-reactive protein; NASH/NAFLD: nonalcoholic steatohepatitis/nonalcoholic fatty liver disease.
Although subjects treated with pioglitazone may gain weight, visceral, hepatic and muscle fat content are decreased.
Pioglitazone transacts its effects through activation of the nuclear hormone receptor peroxisome proliferator–activated receptor-gamma (PPARγ). 72 PPARγ receptors are expressed in endothelial cells, arterial smooth muscle cells and monocytes/macrophages, providing a pathway for direct anti-inflammatory, antioxidant and other protective actions of pioglitazone.73–77 Pioglitazone is the only true insulin-sensitizing antidiabetic agent 78 and insulin resistance has been independently associated with atherosclerotic CVD in many cross-sectional and prospective studies.2,29,58,79–84
Pioglitazone is a potent insulin sensitizer
The core pathophysiologic defects in T2DM are insulin resistance in muscle and liver and beta-cell failure.2,55,85 Collectively, these three pathophysiologic disturbances have been termed the TRIUMVIRATE.2,55 Insulin resistance in liver results in excess glucose production during the sleeping hours and is the primary factor responsible for fasting hyperglycaemia, while insulin resistance in muscle is the primary factor responsible for postprandial hyperglycaemia. Impaired suppression of hepatic glucose production and reduced liver glucose uptake following a meal also contribute to the postprandial hyperglycaemia.55,85 Progressive beta-cell failure55,85–88 accentuates the insulin resistance in liver and muscle. In addition, the adipocyte is resistant to insulin,2,55,85 resulting in accelerated lipolysis and increased circulating plasma FFA concentrations.89,90 Elevated plasma FFA in turn exacerbate the muscle insulin resistance, 91 stimulate hepatic gluconeogenesis and inhibit hepatic glucose uptake 92 and impair beta-cell function. 93 Pioglitazone improves insulin sensitivity in skeletal2,55,72,94–96 and cardiac48,49 muscle, in liver 97 and in adipose tissue 98 via multiple mechanisms: PPARγ activation, stimulation of the insulin signal transduction system, improved glucose transport/glycogen synthesis/glucose oxidation, increased mitochondrial function, reduced plasma FFA levels and reversal of lipotoxicity.2,55,63–66
Pioglitazone improves beta-cell function
Insulin resistance is the earliest detectable disturbance in the natural history of T2DM.2,55,85 However, overt diabetes does not develop in the absence of beta-cell failure and progressive decline in insulin secretion.2,55,85–88 Although not well appreciated, TZDs, including pioglitazone, in addition to their insulin-sensitizing action, exert a potent effect to preserve beta-cell function99,100 and durability of glycaemic control has been demonstrated in eight long-term, double-blind, placebo-controlled or active comparator studies for up to 5 years (reviewed by DeFronzo 55 ). Multiple studies performed in subjects with impaired glucose tolerance (IGT) also have demonstrated a potent action of TZDs to augment beta-cell function (reviewed in previous studies86,100,101). For example, in the ACT NOW study,100,102 conversion of IGT to T2DM was reduced by 72% and improvement in the insulin secretion/insulin resistance (disposition) index (gold standard measure of beta-cell function) was the strongest predictor of diabetes prevention. 100 The improvement in beta-cell function is related to stimulation of PPARγ receptors on the beta cell, enhanced beta-cell sensitivity to glucose and reversal of lipotoxicity.55,103
Pioglitazone improves NASH/NAFLD
NAFLD has reached epidemic proportions in the United States and worldwide 104 and is the precursor for NASH. 105 Diabetic patients with NASH are at high risk for cirrhosis and hepatocellular carcinoma. 106 Patients with NAFLD/NASH are markedly resistant to insulin, often have the metabolic syndrome and are also at increased risk for CVD.107–110 Because pioglitazone improves insulin sensitivity, corrects multiple components of the IRS, ameliorates lipotoxicity and protects against atherosclerotic CVD, it would be an excellent agent for the treatment of NAFLD and NASH. Indeed, multiple studies have demonstrated that pioglitazone consistently reduces hepatic fat content and reverses hepatic fibrosis.59–62 No other antidiabetic agent other than rosiglitazone, a TZD, has shown benefit in the treatment of NAFLD/NASH.111,112
Safety concerns
Fat weight gain
Weight gain is common with pioglitazone therapy, typically amounts to ~2 to 3 kg of fat mass over 1 year16,113,114, and is dose related.113,115 Of note, the greater is the weight gain, the greater is the decline in HbA1c and the greater are the improvements in insulin secretion and insulin sensitivity.94,99,116 How is this explained? Pioglitazone causes an increase in body weight by stimulating PPARγ receptors in the hypothalamus to augment appetite. 117 However, pioglitazone simultaneously stimulates PPARγ receptors in subcutaneous adipocytes to induce genes involved in adipogenesis. 118 The newly formed, smaller fat cells take up FFA leading to a reduction in the plasma FFA concentration and decreased flux of FFA into liver, muscle and visceral fat depots. In addition, pioglitazone stimulates PPARγ coactivator-1 (PGC-1) which is the master switch for mitochondrial biogenesis.119,120 This causes transcription of mitochondrial genes involved in fatty acid oxidation, resulting in a further reduction in the intramyocellular and hepatocyte lipid content with reversal of lipotoxicity.2,55,121 It is noteworthy that weight gain, not weight loss, was associated with increased survival in the PROactive study. 122 This observation suggests that pioglitazone also mobilizes fat out of the arterial wall (see preceding discussion).
It is notable that no specific adverse effects of the fat weight gain have been observed in T2DM patients treated with pioglitazone for up to 3–6 years.16,17,23,62,123 Importantly, the weight gain is dose related and can be minimized by not exceeding a dose of 30 mg/day, 113 the point at which ~80% of the drug’s glucose-lowering efficacy is observed. Combination therapy of pioglitazone with metformin minimizes the weight gain, 124 while combination therapy with a SGLT2 inhibitor19,20 or with a GLP-1 RA19,125,126 reduces both the weight gain and fluid retention.
Fluid retention and HF
When used as monotherapy, oedema is observed in 5%–10% of pioglitazone-treated individuals and, like weight gain, is dose related.113,115 When used in combination with a sulphonylurea or insulin, the incidence of oedema is increased further. 115 The oedema results from two factors: peripheral vasodilation 127 and renal sodium retention. 128 Despite increased total body sodium, blood pressure consistently declines,48,49,56 indicating that the drug’s predominant effect is on the vasculature to decreased vascular tone, and that sodium retention is secondary to the vasodilation. Pioglitazone has no apparent negative effect on LV function48,49 and improves diastolic dysfunction.48–52 Nonetheless, pioglitazone should not be used in T2DM patients with symptomatic HF since fluid accumulation in a noncompliant ventricle can precipitate HF in such individuals, leading to clinical deterioration. 115 Salt and water retention respond best to diuretics that act in the distal tubule such as spironolactone, triamterene and amiloride. 115 Patients should be instructed to report new oedema or dyspnoea to their physician. If more than trace oedema is present, treatment with one of the distally acting diuretics should be instituted and/or the dose of pioglitazone reduced. Of note, in the IRIS study, 17 the number of patients who developed HF was similar in the pioglitazone-treated (n = 74) and placebo-treated (n = 71) groups and this study did allow for dose reduction for oedema or weight gain not responding to initial lifestyle recommendations.
Bone fractures
An increase in bone fractures has been reported in T2DM individuals treated with TZDs.17,129–132 The fractures primarily affect postmenopausal women, occur in the distal long bones of the hands and feet and are related to trauma. One study has reported an increase in fractures in men, 17 while some studies have failed to observe any increase in fractures in either sex. 46 The excess fracture risk amounts to 0.8 fractures per 100 patient-treatment years (1.9 vs 1.1 in pioglitazone vs comparator-treated group).129–132 Fractures are uncommon in premenopausal women and men. Pioglitazone should be used cautiously or not at all in individuals at high fracture risk, including postmenopausal women with osteoporosis or those with prior fracture.
Bladder and cancer
In PROactive, 16 there was a nonsignificant increase in the number (16 vs 6, p = 0.069) of patients who developed bladder cancer. Before unblinding of the results, external experts adjudicated that 11 cases could not plausibly be related to treatment (due to the temporal sequence of drug exposure and cancer diagnosis), leaving six cases in the pioglitazone group and three cases in the placebo group (p = 0.309). Of note, there were significantly fewer cases of breast cancer (3 vs 11, p = 0.034) in the pioglitazone-treated group and the overall incidence of cancer was similar in both groups. Also, after 10 years of follow-up, the incidence of bladder cancer was similar in pioglitazone-treated versus placebo-treated subjects (28 vs 26, respectively). 23 After PROactive, the FDA requested that the manufacturer of pioglitazone initiates a prospective study to examine the relationship between pioglitazone and bladder cancer. A midpoint analysis of this 10-year study 133 involving 193,099 patients revealed no significant association between pioglitazone and bladder cancer (HR = 1.2, 95% CI = 0.9–1.5, p = NS), but those who were exposed for at least 2 years had a small increased risk (HR = 1.4, 95% CI = 1.0–2.0). The 10-year follow-up data, however, failed to find any such association between pioglitazone and bladder cancer with sensitivity analyses showing that the neutral effect was present irrespective of dose and duration of therapy (HR = 1.06, 95% CI = 0.89–1.26, p = NS). 134 In a multinational cohort 135 involving 1.01 million T2DM patients with greater than 5.9 million person-years, the HR for bladder cancer with pioglitazone and rosiglitazone was 1.01 and 1.00, respectively (both p = NS). In the recently published IRIS study, 17 no increase in bladder cancer was observed in the pioglitazone group (0.6% vs 0.4%, p = 0.37). Based upon the preceding body of evidence, however, the FDA still cautions about this risk and recommends that pioglitazone not be used in diabetic patients with active bladder cancer or history of bladder cancer.
Summary
As we transition to a new evidence-based era of T2DM management in patients with CVD, 15 it is imperative that we choose therapies that not only improve glycaemic control but also improve CV outcomes–the latter representing the greatest cause of mortality in this population. Pioglitazone has been shown to reduce MACE (MI, stroke and CV mortality) in multiple studies including PROactive, 16 IRIS, 17 meta-analyses of multiple prospective studies;21,22 to reduce CV events and mortality in several large observational studies;24–26,40 to retard the anatomical progression of coronary and carotid atherosclerosis in PERISCOPE, 27 Chicago 28 and ACT NOW (Table 2). 102 Pioglitazone is the only available insulin-sensitizing agent and has a potent beneficial effect to improve and preserve beta-cell function, leading to a durable reduction in HbA1c (Table 2). Pioglitazone also corrects multiple components of the metabolic syndrome and is an effective treatment for NASH/NAFLD. Side effects remain a concern but can be mitigated by optimizing dosing strategies and combining therapy with other medications (metformin, SGLT2i, GLP-1 RA) that promote weight loss and sodium excretion. The benefit to risk ratio of pioglitazone is very favourable when caution is employed to avoid the known side effects of the drug (Table 2). Moreover, pioglitazone is now generically available and some 50 times less expensive than many branded glucose-lowering drugs with recent CV benefits. It, therefore, represents a highly affordable option for the treatment of patients with T2DM, especially those with prevalent CVD.
Benefits and risk associated with pioglitazone therapy.
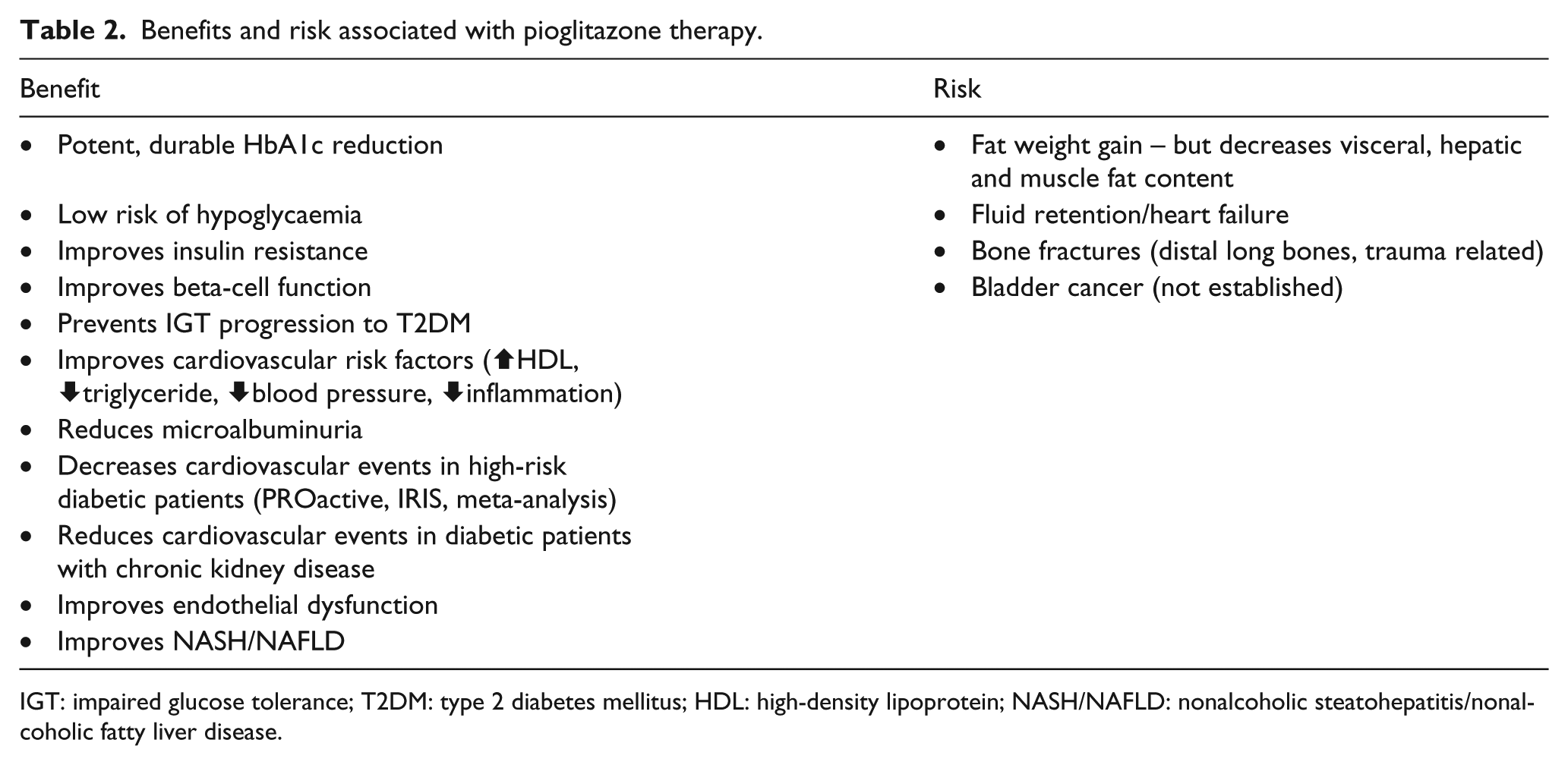
IGT: impaired glucose tolerance; T2DM: type 2 diabetes mellitus; HDL: high-density lipoprotein; NASH/NAFLD: nonalcoholic steatohepatitis/nonalcoholic fatty liver disease.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: R.A.D. serves the Advisory Board of AstraZeneca, Novo Nordisk, Janssen, Boehringer Ingelheim, Intarcia and Elcelyx; research support in Boehringer Ingelheim, Takeda, AstraZeneca and Janssen; speaker’s bureau in Novo Nordisk, AstraZeneca and Merck. S.I. serves the Clinical trial Steering/Executive Committees for Boehringer Ingelheim, AstraZeneca, Novo Nordisk and Eisai (TIMI); data monitoring committees for Intarcia; consultant for Janssen and vTv Therapeutics. M.A-G. has no conflict of interest with this manuscript. S.E.N. reports that the Cleveland Clinic centre for Clinical Research has received funding to perform clinical trials from AbbVie, AstraZeneca, Amgen, Cerenis, Eli Lilly, Esperion, Pfizer, The Medicines Company, Takeda and Orexigen. He is involved in these clinical trials, but receives no personal remuneration for his participation; consults for many pharmaceutical companies, but requires them to donate all honoraria or consulting fees directly to charity so that he receives neither income nor a tax deduction.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.