
Abstract
Aims
To determine whether incident minor and major lower extremity amputations (LEAs) have declined in recent decades in type 2 diabetes.
Methods
Participants with type 2 diabetes from the community-based Fremantle Diabetes Study Phases I (FDS1; n = 1,296, mean age 64.0 years, recruited 1993–1996) and II (FDS2; n = 1,509, mean age 65.4 years, recruited 2008–2011) were followed from entry to incident minor/major LEA, death or five years. Cox regression determined hazard ratios (HRs) for each outcome for FDS2 versus FDS1 and independent predictors of incident minor and major LEA in the combined cohort.
Results
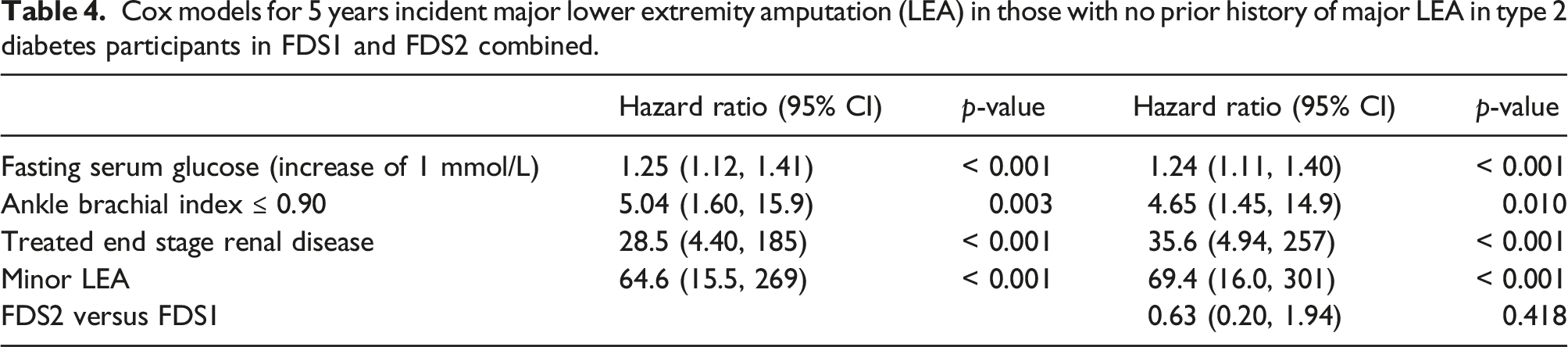
Age- and sex-adjusted HRs (95% CIs) in FDS2 versus FDS1 for incident minor and major LEA were, respectively, 0.60 (0.27, 1.35) and 0.59 (0.22, 1.59). Higher glycated haemoglobin, urine albumin: creatinine (uACR) ratio and peripheral sensory neuropathy (PSN) were independent predictors of incident minor LEA. Higher fasting serum glucose, peripheral arterial disease (PAD), end-stage kidney disease and prior diabetes-related minor LEA were associated with incident major LEA.
Conclusions
There were non-significant reductions of approximately 40% in incident minor and major LEA in community-based people with type 2 diabetes during the 15 years between FDS Phases. Predictors of minor/major LEA confirm distinct high-risk patient groups with implications for clinical management.
Introduction
The incidence of lower extremity amputation (LEA) is an important outcome measure in the management of diabetes-related foot disease (DFD) and a key target for health system improvement. 1 Major complications of type 2 diabetes have been largely declining in developed countries over the past few decades, and trends in LEA incidence are similar albeit more variable.2-7 This variability likely reflects between-study differences in social, economic, organisational and patient-related factors, as well as methods of data collection and analysis.7-10 In addition, while more intensive cardiovascular risk factor management, increased DFD awareness, and improved access to multidisciplinary high-risk foot services should contribute to reduced LEA rates, the differentiation between minor and major LEAs as opposed to reporting total LEA rates alone is an important consideration in interpreting the epidemiological data. 9 Minor LEAs typically represent an attempt at limb salvage in moderate to severe DFD, and they differ markedly from major LEAs regarding their impact on morbidity, mortality and quality of life. 9 When longitudinal epidemiological studies have reported a decline in total LEA, this has been driven predominantly by decreased major LEAs while minor LEAs have remained stable or increased.2,5,6,10-14 Indeed, US data suggest that a recent resurgence in LEA incidence has resulted from an increase in minor LEAs in younger people with type 2 diabetes.14,15
Published Australian estimates of the incidence of LEA have also varied widely depending on the source of data and ascertainment, and there are limited detailed data related to temporal changes in incident minor and major LEAs.5,6,9,11,16-18 We previously reported a non-significant 50% decrease in incidence of all LEA over a 15 year period between the community-based Fremantle Diabetes Study Phases I (FDS1) and II (FDS2), as well as a reduction of > 50% in the incidence rate difference for people with versus without diabetes type 2 diabetes over the same period. 5 The detailed patient-level data and long follow-up that characterise the FDS circumvent some limitations associated with published LEA data that have been derived from administrative datasets and clinic-based samples, which may not be representative, and can have incomplete phenotypic data and a lack of validation of key outcome measures. Given this background, we have utilised baseline and longitudinal data from the FDS1 and FDS2 to determine whether 5 years incidence rates (IRs) of minor and major LEA have changed in people with type 2 diabetes in the 15 years between FDS Phases, and to examine independent predictors of minor and major LEA in the pooled FDS cohorts.
Methods
Study site, participants and approvals
The FDS is an observational, longitudinal study of diabetes in a postcode-defined area surrounding the port of Fremantle in the state of Western Australia (WA).19,20 There were approximately 120,000 people residing in the catchment area at the start of FDS1 in 1993 and 157,000 when FDS2 recruitment began in 2008. Socio-economic data from this area during FDS2 recruitment showed an average Index of Relative Socio-economic Advantage and Disadvantage 21 of 1033 with a range by postcode of 977–1113, figures comparable to the Australian national mean ± SD of 1000 ± 100.
Recruitment to FDS1 was between 1993 and 1996, with follow-up of diabetes complications and mortality in the present sub-study to end-2013. The FDS2 utilised the same design as FDS1, 20 with recruitment between 2008 and 2011 and follow-up to end-2016. Participants in both Phases were identified from hospital, clinic/primary care patient lists, health care professional networks, pharmacies, optometrists, local media advertisements and, in the case of FDS2, third-party mail-outs to registrants of the Australian National Diabetes Services Scheme and the National Diabetes Register. 20 Details of recruitment, sample characteristics including classification of diabetes types, and non-recruited patients have been published.19,20 In FDS1, patients who were identified as eligible but who declined participation were a mean of 1.4 years older than participants, but their country of birth, sex distribution and diabetes treatment modalities were similar. 20 In FDS2, non-recruited patients were a mean of 1.2 years younger than participants at recruitment, but their sex distribution was similar and available data for other variables including ethnicity did not show significant differences. 20 The FDS1 was approved by the Fremantle Hospital Human Rights Committee, and the FDS2 by the Human Research Ethics Committee of the Southern Metropolitan Area Health Service. All participants gave written informed consent.
Baseline and follow-up assessments
In FDS1, 2258 people with diabetes were identified and 1426 (63%) were recruited, 1296 (91%) of whom had clinically-defined type 2 diabetes; the equivalent figures in FDS2 were 4,639, 1668 (36%), and 1509 (90%), respectively. In both Phases, assessment at entry and at each annual (FDS1) or second-yearly (FDS2) face-to-face review included a comprehensive questionnaire, physical examination, and fasting biochemical tests performed in a single nationally accredited laboratory. 19 In addition to details of medical conditions, demographic, socio-economic and lifestyle data were collected. Patients were requested to bring all medications to each visit and full details were recorded. In FDS2, comprehensive questionnaires were posted out in the years between face-to-face reviews.
Complications were identified using standard definitions 22 including albuminuria assessed by first morning urine albumin: creatinine ratio (uACR) measurement and renal impairment from the estimated glomerular filtration rate (eGFR). 23 A general foot inspection was performed to detect presence/absence of DFU located at or below the level of the malleoli, deformity, corns/callus, fissures, infections and nail pathology. Peripheral sensory neuropathy (PSN) was defined using the Michigan Neuropathy Screening Instrument clinical portion. 24 Patients were classified as having prevalent coronary heart disease (CHD) if there was a history of myocardial infarction, angina, coronary artery bypass grafting, or angioplasty, and as having prevalent cerebrovascular disease if there was a history of stroke and/or transient ischaemic attack. Peripheral arterial disease (PAD) was defined as an ankle brachial index ≤ 0.90 or the presence of a diabetes-related LEA.
Ascertainment of 5 years minor and major lower extremity amputation incident rates
Participants in both Phases were followed to incident minor or major LEA, death or five years, whichever came first. The Hospital Morbidity Data Collection (HMDC) contains information regarding all public/private hospitalisations in WA since 1970, and the Death Register contains information on all deaths in WA. 25 Both FDS phases have been linked through the WA Data Linkage System (WADLS) to these databases, as approved by the WA Department of Health Human Research Ethics Committee, to provide validated data on incident events to end-2017 for FDS1 and end-2016 for FDS2. Relevant International Classification of Disease (ICD)-9-CM and ICD-10-AM diagnosis codes were used to classify for minor and major amputation. A minor LEA was defined as being a lower limb resection at/distal to the ankle and a major LEA was defined as being a lower limb resection proximal to the ankle. 26 The HMDC was also used to supplement data obtained through FDS assessments relating to prevalent/prior disease.
Statistical analysis
The computer package IBM SPSS Statistics 28 (IBM Corporation, Armonk, NY, USA) was used for statistical analysis. Data are presented as proportions, mean ± SD, geometric mean (SD range), or, in the case of variables which did not conform to a normal or log-normal distribution, median and inter-quartile range [IQR]. Two-sample comparisons were by Fisher’s exact test, Student’s t-test or Mann–Whitney U test as appropriate to the data.
Five-year IRs for incident minor and incident major LEAs were derived for each FDS Phase and the crude incident rate ratio (IRR) calculated for those with type 2 diabetes in FDS2 versus FDS1. Cox regression was performed to determine unadjusted and age-and sex-adjusted hazard ratios (HRs) for each outcome by FDS Phase (FDS2 versus FDS1). For the pooled FDS1 and FDS2 type 2 diabetes cohort, Cox regression with backward conditional variable entry (p < 0.01) and removal (p ≥ 0.01) was used to determine independent predictors of the first episode of each outcome during follow-up from clinically plausible baseline variables with p < 0.20 in bivariable analyses. To assess the effect of FDS Phase, participation in FDS2 versus FDS1 was then added to each most parsimonious model. Missing values were multiply imputed.
Results
Incident minor and major lower extremity amputations
At baseline, 1.5% (20/1296) of FDS1 participants with type 2 diabetes had undergone at least one LEA prior to study entry. Of these 20, 16 (1.2% [95% CI] [0.7–2.0%]) had diabetes-related LEAs. Nine participants had major LEAs (eight diabetes-related), four of whom were bilateral amputees.
During follow-up to death or 5 years post-study entry, whichever came first, 23 FDS1 participants had 33 admissions for LEAs comprising 22 minor and 11 major (with or without a minor LEA during the same admission). Of these 23 participants, 13 had minor LEAs only, seven had major LEAs only, and three had both minor and major LEAs. Three of the 23 had a prior history of diabetes-related LEA (two minor, one major). Excluding the 16 participants with a prior history of any diabetes-related LEA, 14 participants had their first minor LEA during 5906 person-years (mean ± SD 4.6 ± 1.1 years) of follow-up to first minor LEA, death or 5 years, an incident rate of 23.7 (95% CI: 13.0, 39.8)/10,000 person-years. Excluding the 8 participants with a prior history of diabetes-related major LEA, 9 participants had their first major LEA during 5951 person-years (mean ± SD 4.6 ± 1.1 years) of follow-up to first major LEA, death or 5 years, an incident rate of 15.1 (95% CI: 6.9, 28.7)/10,000 person-years.
At baseline, 1.1% (16/1509) of FDS2 participants with type 2 diabetes had undergone at least one LEA prior to study entry. Of these 16, 14 (0.9% [95% CI] [0.5–1.6%]) had diabetes-related LEAs, the remaining two participants having had a LEA > 35 years before diagnosis of diabetes. Three participants had major LEAs, one of whom was a bilateral amputee.
During follow-up to death or 5 years post-study entry, whichever came first, 18 FDS2 participants had 25 admissions for LEAs (16 minor, 9 major). Of these participants, 11 had minor LEAs only, 4 had major LEAs only, and 3 had both minor and major LEAs. Six of the 18 had a prior history of diabetes-related minor LEA. Excluding the 14 with a prior history of diabetes-related LEA (major or minor), 10 participants had their first incident minor LEA during 7079 person-years (mean ± SD 4.7 ± 0.9 years) of follow-up to first minor LEA, death or 5 years, an incident rate of 14.1 (95% CI: 6.8–26.0)/10,000 person-years. Excluding the three participants with a prior history of diabetes-related major LEA, 7 participants had their first major LEA during 7127 person-years (mean ± SD 4.7 ± 0.9 years) of follow-up to first major LEA, death or 5 years, an incident rate of 9.8 (95% CI: 4.0–20.2)/10,000 person-years.
Five year incidence rate ratios for minor and major lower extremity amputations
The crude incidence rate ratio (IRR) (95% CI) for incident minor LEA in FDS2 versus FDS1 was 0.60 (0.24, 1.44), p = 0.211 and for incident major LEA in FDS2 versus FDS1 was 0.65 (0.21, 1.96), p = 0.399. In unadjusted Cox regression, the HRs (95% CIs) in FDS2 versus FDS1 for incident minor and major LEA were, respectively, 0.60 (0.27, 1.34), p = 0.212, and 0.65 (0.24, 1.75), p = 0.393. After adjustment for age and sex, these HRs were, respectively, 0.60 (0.27, 1.35), p = 0.216, and 0.59 (0.22, 1.59), p = 0.295.
Associates of incident minor and major lower extremity amputation
Characteristics at study entry of type 2 diabetes participants in FDS1 and FDS2 combined by 5 years incident minor lower extremity amputation (LEA) in those with no prior history of any LEA.

aDue to patient confidentiality, numbers≤ 5 cannot be specifically reported.
bIn the last 5 years, excluding diabetes and its complications.
Cox models for 5 years incident minor lower extremity amputation (LEA) in those with no prior history of LEA in type 2 diabetes participants in FDS1 and FDS2 combined.

aAn increase of 1 in ln(uACR) corresponds to an increase of 2.72 in uACR; uACR: Urinary albumin: creatinine ratio.
Characteristics at study entry of type 2 diabetes participants in FDS1 and FDS2 combined by 5 years incident major lower extremity amputation (LEA) in those with no prior history of major LEA.

aDue to patient confidentiality, numbers ≤ 5 cannot be specifically reported.
bIn the last 5 years, excluding diabetes and its complications.
Cox models for 5 years incident major lower extremity amputation (LEA) in those with no prior history of major LEA in type 2 diabetes participants in FDS1 and FDS2 combined.
Discussion
The present study demonstrates non-significant reductions of 40% in incident minor LEA and 35% in incident major LEA in community-based people with type 2 diabetes during the mean 15 years between FDS Phases. Although constrained by limited numbers of endpoints, these data suggest that the recent increase in minor LEAs found in a contemporaneous US study14,15 may not apply to a representative Australian urban population. The detailed data collection in both FDS phases allowed the identification of significant predictors of incident minor and major LEA. Glycated haemoglobin, uACR and the presence of PSN were associates of incident minor LEA across the FDS phases. By contrast, higher fasting plasma glucose, PAD (ABI ≤ 90), end-stage kidney disease and history of diabetes-related minor LEA were associated with incident major LEA. These different risk factor profiles could inform clinical management in facilitating targeted screening and rapid intervention at the onset of any new foot lesion.
As reflected in the variability in LEA trends across different cohorts and populations,2-7 there are differences in study design, methodology and local clinical management that complicate comparisons. For example, the recent US administrative data showing an increase in minor LEAs neither excluded people with LEAs prior to the data collection period nor identified those who had multiple LEAs during follow-up 14 as was done in the present study. The US minor and major amputation IRs were, therefore, generally higher than those in the present study. Given the recurrent and relapsing natural history of diabetes-related foot ulcers (DFU) and the relatively high rates of re-operation after minor LEA,27,28 it is plausible that first incident minor LEAs may be declining as shown in the FDS data but that those requiring a minor LEA are at increasing risk of subsequent repeat minor surgical procedures rather than progression to a major LEA, as shown in the US dataset. Alternatively, the increasing incidence of diabetes and its complications including LEA at a relatively young age that has been seen in the US14,15 has not yet had the same impact on minor LEA IRs in Australia.
The decreasing if non-significant trend in both incident minor and major LEA between the two FDS Phases may seem paradoxical since hospitalisations for DFU have, by contrast, increased significantly. 29 As we have hypothesized previously, clinical management changes and government incentives favouring early identification and referral of people with DFUs, as well as improved initial management by hospital-based specialists in FDS2 versus FDS1, may have increased DFU hospitalizations but contributed to lower LEA rates at the same time. 29 In addition, there is increasing recognition of the pros and cons of amputation which, given its potentially profound effects on quality of life, 9 should be restricted to the unsalvageable diabetic foot. 30
We found clusters of risk factors that differed between minor and major LEAs. The only other longitudinal study reporting predictors of LEA in community dwelling patients with type 2 diabetes was the Seattle Diabetic Foot Study which followed male veterans over 22 years and included a detailed assessment of clinical and limb characteristics. 31 PSN and PAD were important predictors of LEA, as were lower eGFR, impaired vision, a lower BMI and younger age. 31 There was overlap between a number of these risk factors and those identified in the present study, but we were able to further refine those for both major and minor LEA. Our data show that minor LEAs were a more likely outcome in participants with poor glycaemic control and microangiopathy (albuminuria and PSN) at baseline, while major LEAs were a more frequent subsequent occurrence in those with macrovascular disease (PAD) and its risk factors (renal disease, and basal hyperglycaemia as a likely surrogate for insulin resistance). As might be expected, a history of prior minor LEA was also a predictor, consistent with the progressive nature of DFD. In Australia, marked variation in amputation rates has been reported across a number of studies,5,6,9,11,16-18 with higher rates amongst Aboriginal and Torres Strait Islander (ATSI) people and people living in rural and regional areas.32-34 We did not find that Aboriginality was an independent predictor of either minor or major LEA in the present study. However, these outcomes were associated with risk factors such as PSN, albuminuria, PAD and higher HbA1c which are more prevalent amongst ATSI people than other Australian ethnic groups.34,35
The present study had limitations. The trends in both LEA groups were non-significant and had wide confidence intervals, consistent with limited statistical power. LEA is a low frequency event which increases the risk of a type II statistical error and thus the risk of missing a true reduction in minor and/or major LEAs with time across the FDS Phases. However, our findings are consistent with a report of a significant reduction in initial major LEA and a non-significant decline in minor LEAs between 2000 and 2010 in all Western Australians coded as having type 2 diabetes in the WADLS. 11 This latter study covered a shorter, largely non-overlapping intermediate period of follow-up, did not have detailed patient-level data including that required to accurately ascertain diabetes type, and miscoding leading to underestimation of diabetes cases was an acknowledged limitation. 11 Nevertheless, the total initial LEA rate (34/10,000 patient-years 11 ) lay, as expected, between FDS1 (39/10,000 patient years) and FDS2 (24/10,000 patient-years), and the majority of LEAs were minor as in both FDS1 and FDS2. These observations suggest a limited potential influence of people who were eligible for FDS1 or FDS2 but who were not recruited on our findings. The present data and those of other longitudinal studies could contribute to future pooled analyses with more confident statistical outcomes. Additional limitations included the restricted number of endpoints which influenced the number of significant predictors in multivariable analyses. Nevertheless those identified were highly clinically plausible. The ABPI may be falsely elevated in people with diabetes due to medial arterial wall calcification and this may have impacted on the strength of the association between this variable and LEA in the bivariable analyses and Cox models. The strengths of the present study include its use of well characterized community-based cohorts, long duration of follow-up and highly detailed participant level data including comprehensive clinical assessment of the lower limb.
We report non-significant reductions in both minor and major LEA in community dwelling Australians with type 2 diabetes between the two FDS phases. Key drivers of minor LEA were higher glycated haemoglobin, albuminuria and PSN, indicating that efforts to improve glycaemic control and prevent microvascular complications of diabetes are important in the prevention of DFD severe enough to lead to amputation. Predictors of major LEA were recognised risk factors including end-stage renal disease, PAD and history of minor LEA as well as suboptimal glycaemic control in the form of an elevated fasting serum glucose. These findings confirm known high-risk patient groups who should be targeted for intervention and support including optimisation of glycaemic control, regular foot screening and rapid assessment and specialist management in the event of development of a new DFU.
Footnotes
Acknowledgements
The authors wish to thank the FDS1 staff, investigators and participants, the staff at the Western Australian Data Linkage Branch, the Hospital Morbidity Data Collection, the Registry for Births, Deaths and Marriages, and the National Coronial Information System.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: seeding funding for FDS1 was provided by the Raine Foundation University of Western Australia and FDS2 was funded by the National Health and Medical Research Council of Australia (project grants 513781 and 1042231). EJH is supported by a Raine Clinician Research Fellowship. TMED is supported by a Medical Research Future Fund Practitioner Fellowship. The funding bodies had no involvement in the study design, data collection, analysis and interpretation of results or writing this manuscript.