
Abstract
Aim
The objective of the present real-life study in France was to assess and compare characteristics and outcomes in a cohort of pregnant women with type 1 diabetes (T1D) using intermittently scanned continuous glucose monitoring (isCGM) or conventional blood glucose monitoring (BGM).
Material and Methods
We performed an observational study of a cohort of 153 women with T1D: 77 women were using isCGM, and 76 were using BGM. We compared the groups’ maternal characteristics and maternal-fetal complications. The level of HbA1c was measured before pregnancy and then four times (after 8–12, 24–28, 30–33, and 35–37 weeks of gestation).
Results
The two groups were similar in terms of age, prepregnancy BMI, diabetes duration, and diabetic vascular complications. There were no significant intergroup differences in the obstetric history. The spontaneous abortion rate was lower in the isCGM group than in the blood glucose monitoring group (5.3% vs. 20%, respectively; p = .0129), while the prepregnancy and first-trimester HbA1c levels were similar. There were no significant intergroup differences in the incidence of other maternal-fetal complications.
Conclusions
This observational study demonstrates that isCGM use is associated with lower spontaneous abortion compared with conventional BGM. Large prospective studies are needed to corroborate our findings and fully understand the relationship between glucose data at the time of conception/early pregnancy and foetal outcome.
Keywords
Introduction
Although continuous glucose monitoring has been available for the past 20 years, it is only recently that people with diabetes have gained access to devices specifically approved for use during pregnancy. The increasing available, affordable and user-friendly intermittently scanned CGM (isCGM) technique has undoubtedly transformed the clinical management of diabetes before and during pregnancy. 1 In most of recent work, for adults with diabetes, the use of isCGM is associated with lower glycated hemoglobin (HbA1c) levels, lower hypoglycemia, greater treatment satisfaction and greater well-being.2–4 However, the data are still sometimes controversial 5 with sometimes none effect or sometimes more episodes of severe hypoglycemia and diabetic ketoacidosis in isCGM.6–8 In the context of pregnancy, it has been suggested that isCGM may have an important role in reducing the risk of maternal-fetal complications by increasing glycemia control and the quality of life for pregnant women with T1D. 9 Recently, the CONCEPTT study found that CGM during pregnancy in women with T1D was associated with lower HbA1c levels, more time spent in the target range, less time spent above the target range, and less variability. Furthermore, neonatal outcomes were better; these included a lower incidence of large-for gestational-age infants and a lower incidence of neonatal hypoglycemia. 10 In a study of 796,346 child births in France, Billionnet et al. found that .16% of the women had pregestational T1D. This condition was associated with a higher risk of maternal-fetal complications, with incidences of 43.7% for macrosomia, 57.1% for cesarean section, and 30.4% for prematurity. 11 More recently, Murphy et al.‘s 5-year, national, population–based cohort study reported that the prevalence of congenital anomalies was 44.8 per 1000 livebirths, terminations, and fetal losses among women with T1D. 12
Today’s guidelines on pregnancy for women with diabetes advocate an HbA1c goal of between 6 and 6.5%, while limiting the number of hypoglycemic episodes as much as possible. 13 Indeed, an elevated blood sugar level around the time of conception and early in the first trimester is associated with abnormally high birth defect rates and a higher prevalence of spontaneous abortion, intrauterine fetal death, preeclampsia, preterm birth, and perinatal mortality.14–16 During pregnancy, the goal is to increase the percentage of time in the target zone as soon as possible, while reducing the time over target and blood sugar variability. For women with conventional BGM, the targets are currently <100 mg/dL (5.5 mmol/L) before a meal and <140 mg/dL (7.78 = mmol/L) after a meal. 13 The international consensus guidelines on CGM recommend reporting the readings as the proportions of time in the target range, above the target range, and below the target range. 17
Based on the trial results for CGM data, all pregnant women with T1D in the United Kingdom will receive government-funded rtCGM for a 12-month period. 18 In France, similar guidelines were implemented recently. 19 However, few data are available and need more documentation. So, the objective of the present real-life study in France was to assess and compare characteristics and outcomes in a cohort of pregnant women with T1D using isCGM or conventional BGM.
Materials and methods
Study design and population
We performed a single-center, retrospective, observational study of women with T1D attending the Center for Pregnant Women with Diabetes at Lille University Medical Centre (Lille, France) during early pregnancy over the period from 2017 to 2020. The study was based on an analysis of electronic medical records, including the metabolic and obstetric data that are routinely collected for all births. According to French legislation, all patients are informed that healthcare-related data may be used for research purposes unless the person opposes such use. The data were analyzed after anonymization, and our database was registered with the French National Data Protection Commission (Commission nationale de l’informatique et des libertés (Paris, France). In this observational cohort, we included all type 1 diabetic women with a live intrauterine singleton and who, routinely used isCGM or BGM during pregnancy according to the French guidelines. All included patients had a viable pregnancy at the time of inclusion. The main exclusion criteria were as follows: age under 18; another type of diabetes (type 2 diabetes, monogenic diabetes, syndromic diabetes, or secondary diabetes); missing data or the absence of consent; persistent diagnostic doubt; loss of follow-up; and twin/multiple pregnancy.
Routine care
All women were receiving the recommended dietary treatment with scheduled meals, in accordance with the French guidelines. The women were told to count carbohydrates, in order to match the insulin dose to the meal’s carbohydrate content. At least 30 min of physical activity per day was also recommended. Patients were treated with short-acting insulin analogues before meals and long-acting insulin analogues in the morning and/or at bedtime, or received continuous subcutaneous insulin infusion (CSII). The insulin dose was titrated on the basis of the BGM or isCGM glucose values data, and the women were encouraged to adjust the planned insulin dose every 3–5 days as appropriate. Women who were already using isCGM routinely before pregnancy continued to use this technique. For women who started to use isCGM after becoming pregnant, the device was applied for the first time by a nurse, and the women were then trained in the use of the device. In all cases, the isCGM device was the Freestyle Libre 1 Flash Glucose Monitor (Abbott Diabetes Care, Alameda, CA) and was placed on the upper arm. The women were advised to scan the isCGM device (using the corresponding mobile app) at least six times daily, i.e. before and 2 h after each of the day’s three meals. All isCGM data were recorded and automatically uploaded using the software provided with the device (Libre View (Abbott)). For the women using BGM, the targets were <100 mg/dL (5.5 mmol/L) before a meal and <140 mg/dL (7.78 mmol/L) 2 h after a meals.
Diabetes and obstetric follow-up were performed monthly and patients were called twice a week by a specialist nurse to assess glucose control and adjust the insulin dose if needed.
The follow-up consultations with a diabetologist and an obstetrician complied with the guidelines issued respectively by the French-speaking Society of Diabetes (Société francophone du diabète) and French National College of Obstetricians and Gynecologists (Collège National des Gynécologues et Obstétriciens Français). The patients were all followed up by the same diabetology and obstetrics teams in a tertiary center.
Collection of clinical data
The women’s demographic, obstetric and medical data, the diabetes duration, and the presence of complications were extracted from the hospital’s electronic medical records.
Age, height, and body weight were recorded, and the pre-pregnancy BMI (weight/height2, in kg/m2) was calculated. Any history of smoking was noted.
The diabetes history was specified as follows: date of diagnosis or first symptoms, multiple daily injections (MDIs) vs. continuous subcutaneous insulin infusion (CSII), the last preconception plasma HbA1c level, micro/macrovascular complications, a history of nephropathy (albuminuria ≥30 mg/24 h, or renal insufficiency), any history of retinopathy, the result of the last preconception fundus examination, and any history of hypertension (defined as a blood pressure >140/90 mmHg or the use of antihypertensive drug before pregnancy. Vascular complications during pregnancy were noted: the appearance or aggravation of diabetic retinopathy, the latter’s characteristics if present, and the appearance or aggravation of proteinuria.
Obstetric outcomes
The obstetric history was assessed as the date of pregnancy, parity, gravidity and any history of preeclampsia, spontaneous abortion, stillbirth, or macrosomia. Loss of pregnancy was assessed: spontaneous abortion was defined as the loss of pregnancy before 22 WG (weeks of gestation), and stillbirth was defined as the loss of pregnancy after 22 WG. The frequency of malformations leading to death, emergency care or disability was determined.
Pregnancy hypertension was defined as the appearance or aggravation of hypertension during pregnancy. Preeclampsia was defined as the combination of a systolic blood pressure >140 mmHg or a diastolic blood pressure >90 mmHg and proteinuria >300 mg/24 h after 20 WG. Prematurity was defined as delivery before 37 WG. The newborn’s birthweight (BW, in g) and phenotypic sex (male or female) were recorded.
Macrosomia was defined as a BW ≥ 4000 g. The BW was adjusted for the newborn’s sex and gestational age for singleton pregnancies, using customized percentiles. Large for gestational age (LGA) was defined as a birthweight above the 90th percentile (according to the AUDIPOG reference curves, and small for gestational age (SGA) was defined as a birthweight below the 10th percentile.
We also noted the type of delivery (vaginal delivery or cesarean section) and whether or not delivery was scheduled. Shoulder dystocia was defined as the use of obstetrical maneuvers other than a gentle pull on the head or a restorative maneuver to free the fetus’s shoulders. The volume of blood loss during delivery was recorded. Major blood loss was defined as the loss of more than 500 mL of blood.
The doses of total insulin, long-acting insulin, and rapid-acting insulin (in IU) during pregnancy were recorded for the periods between 8 and 12, 24 and 28, 30 and 33, and 35 and 37 WG. The insulin ratio (IU/kg) corresponded to the ratio between the total insulin dose and the patient’s weight at the time of data collection.
The HbA1c level was measured before pregnancy and then at 8–12, 24–28, 30–33 and 35-37 WG, using capillary electrophoresis (Capillaris Tera SEBIA, normal, range: 4.0 – 6.0%; coefficient of variation below 3%). The Certified Quality Engineer has been given by Bio-Rad.
Statistical analysis
Statistical analyses were performed using R software (version 3.6.3) and Prism software (version 8, GraphPad Software LLC, San Diego, CA, USA). Categorical variables were quoted as the frequency (percentage). Quantitative variables were quoted as the mean ± standard deviation (when the distribution was Gaussian) or as the median [interquartile range (IQR)]. Associations between a qualitative variable with more than two modalities and a quantitative variable were studied in an analysis of variance (when the distribution was Gaussian) or the Kruskal–Wallis test. Associations between a qualitative variable with more than two modalities and a qualitative variable were investigated using a chi-squared test or Fisher’s test, depending on the sample size. Associations between quantitative variables was assessed using Pearson’s correlation test. All statistical tests were two-sided, and the threshold for statistical significance was set to p < .05. Odds ratios (ORs) were calculated with their 95% confidence interval (CI).
Results
Demographic characteristics of the study population
During the study period, we included 400 pre-gestational pregnant women. We excluded 247 women: 201 with type 2 diabetes, 32 with other forms of diabetes, and 14 with T1D but who met other exclusion criteria (missing data (n = 8), lost to follow-up (n = 5), or twin pregnancy (n = 1)). Thus, our analysis included a total of 153 pregnant women with T1D, of whom 77 used isCGM, and 76 used BGM (Figure 1). Patient enrolment flow chart. Abbreviations; T1D:Type 1 Diabetes; isCGM, intermittently scanned continuous glucose monitoring; BGM, blood glucose monitoring.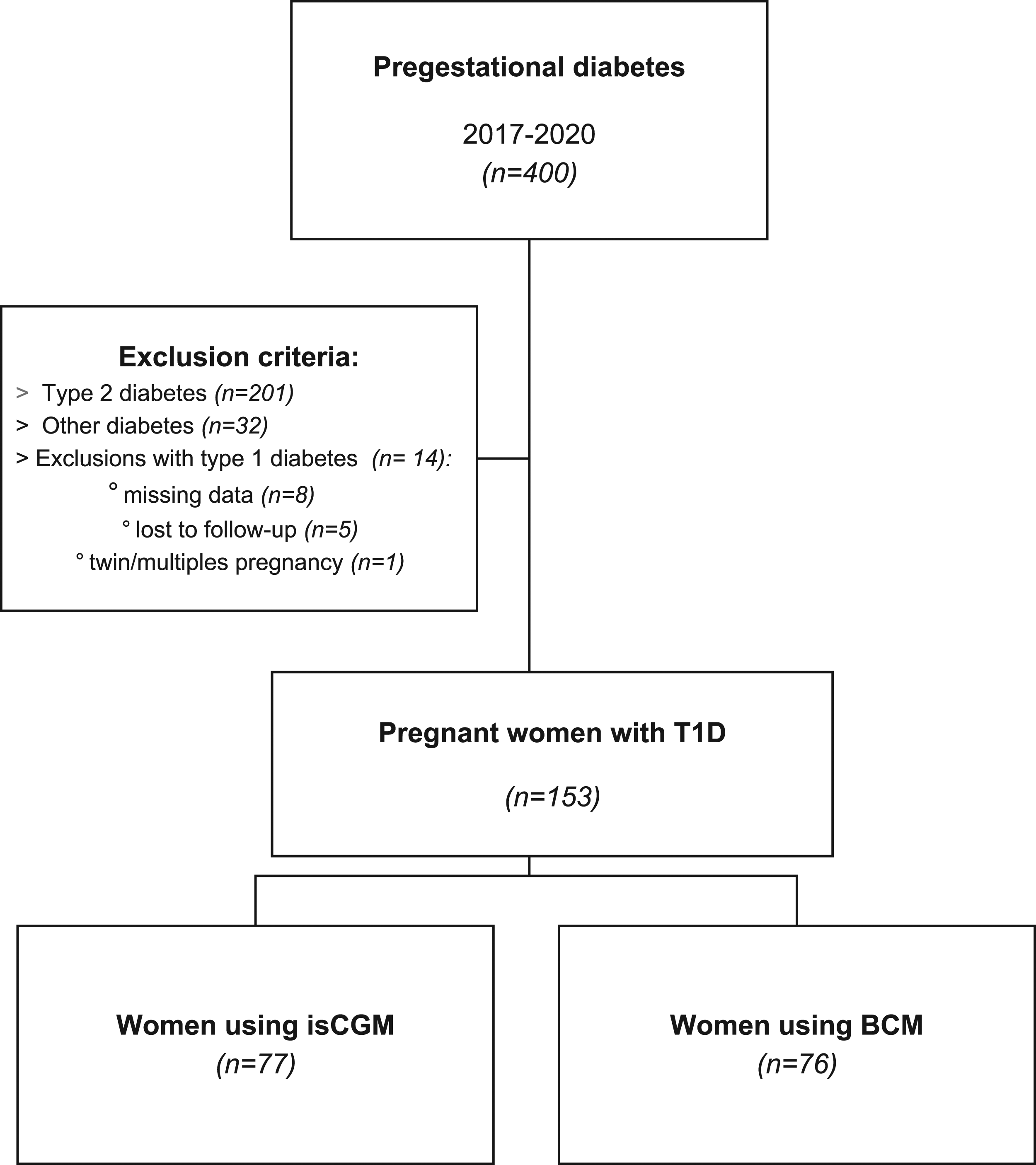
Maternal characteristics at baseline.
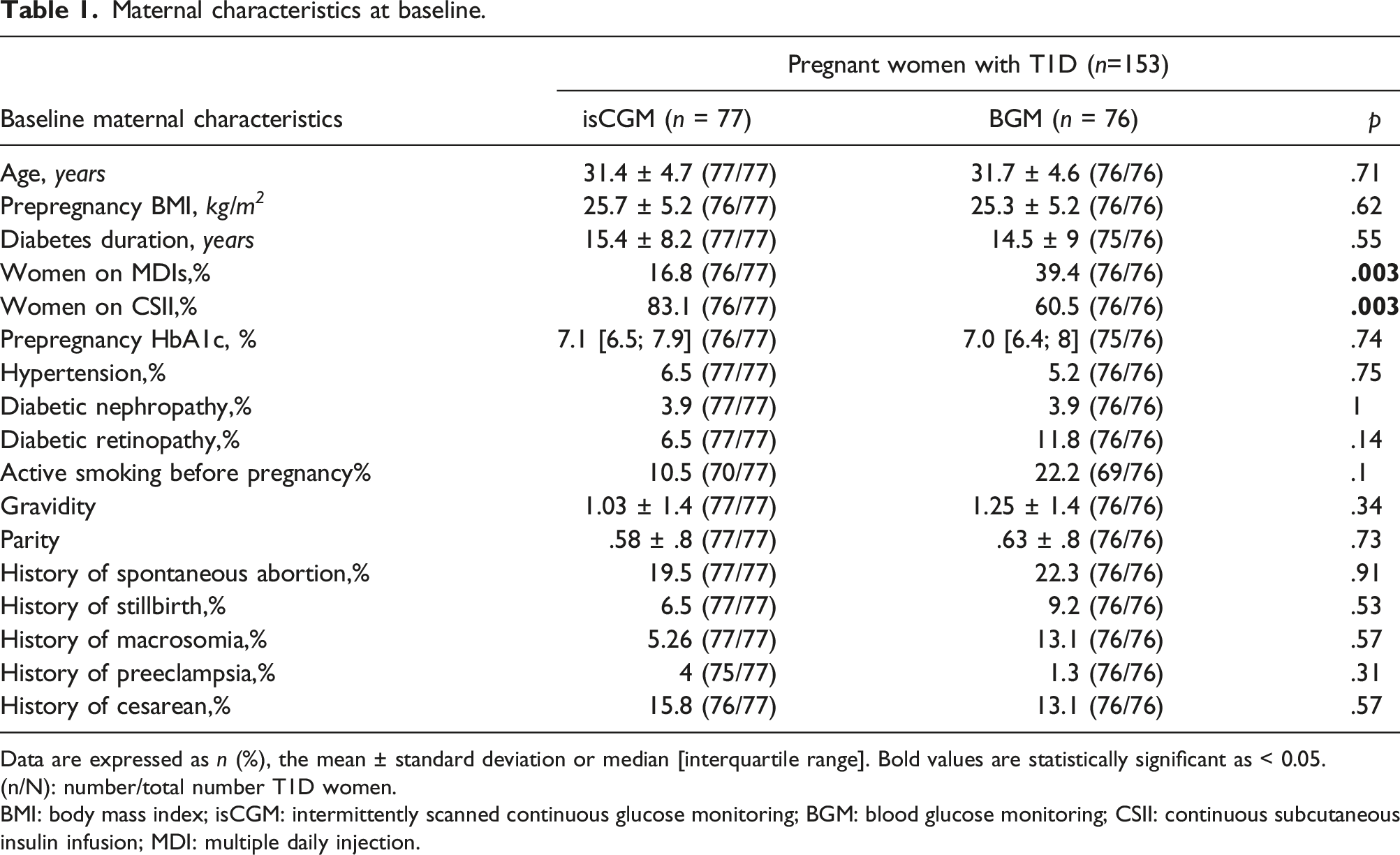
Data are expressed as n (%), the mean ± standard deviation or median [interquartile range]. Bold values are statistically significant as < 0.05.
(n/N): number/total number T1D women.
BMI: body mass index; isCGM: intermittently scanned continuous glucose monitoring; BGM: blood glucose monitoring; CSII: continuous subcutaneous insulin infusion; MDI: multiple daily injection.
Metabolic data recorded during pregnancy
Metabolic data during pregnancy.
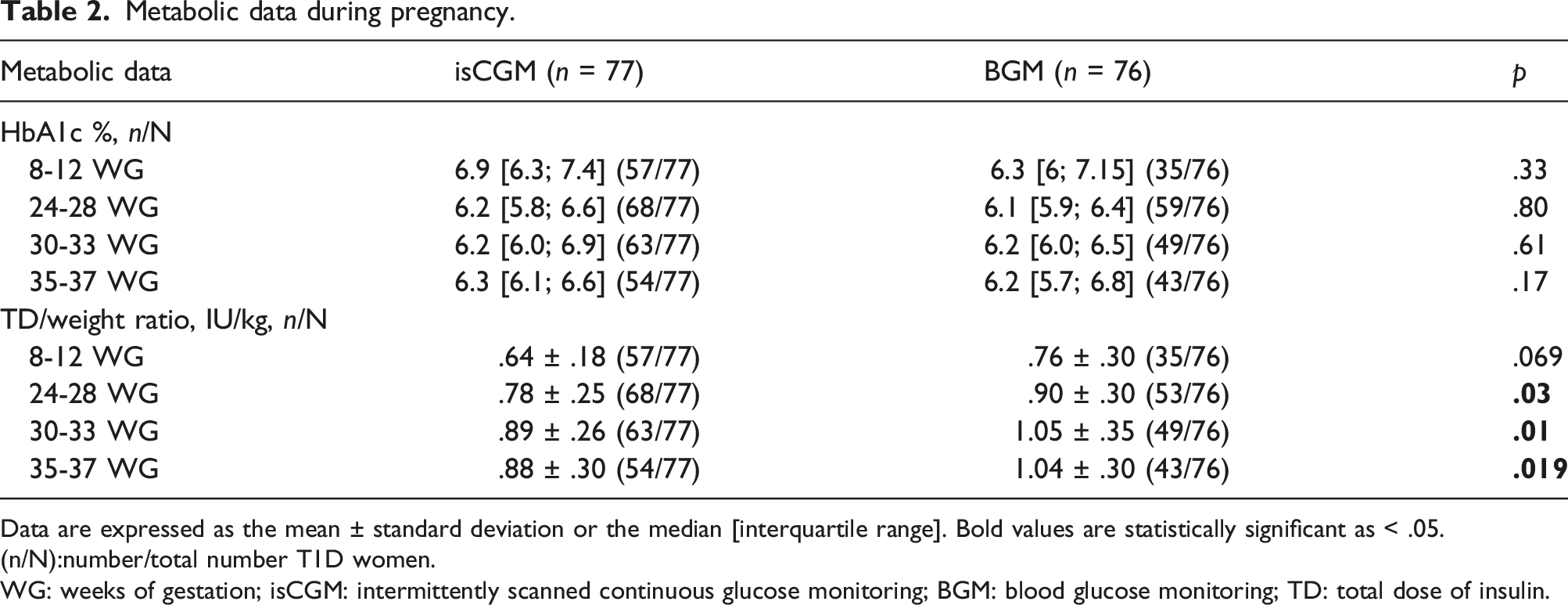
Data are expressed as the mean ± standard deviation or the median [interquartile range]. Bold values are statistically significant as < .05.
(n/N):number/total number T1D women.
WG: weeks of gestation; isCGM: intermittently scanned continuous glucose monitoring; BGM: blood glucose monitoring; TD: total dose of insulin.
Adverse pregnancy outcomes in women with T1D
Adverse pregnancy outcomes during pregnancy in women with T1D.
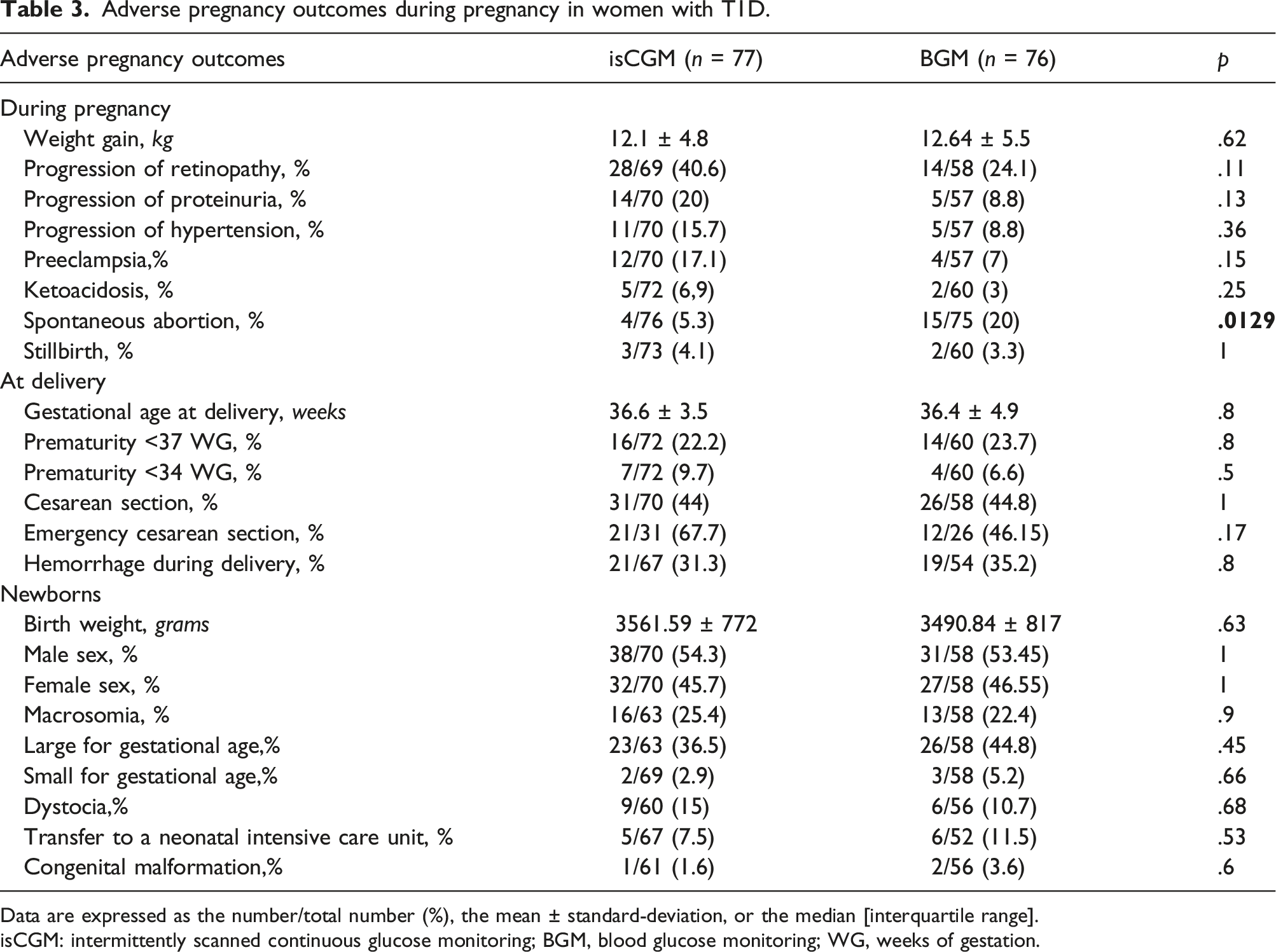
Data are expressed as the number/total number (%), the mean ± standard-deviation, or the median [interquartile range].
isCGM: intermittently scanned continuous glucose monitoring; BGM, blood glucose monitoring; WG, weeks of gestation.
The proportion of newborns with a congenital malformation rate was lower in the isCGM group than in the BGM group (1.6% vs. 3.6%, respectively) but the difference was not statistically significant. The same was true for the proportion of LGA newborns (36.5% in the isCGM group vs. 44.8% in the BGM group; p = .45), the proportion of SGA newborns (2.9% vs. 5.2%, respectively; p = .66), and the proportion of newborns requiring immediate postnatal medical care.
Discussion
There is a growing body of evidence from randomized, controlled trials and cohort studies in favor of the use of CGM during pregnancy as a means of improving obstetric and neonatal outcomes. Accordingly, new guidelines in the UK have introduced 12 months of government-funded rtCGM for all pregnant women with T1D. 19 In France, an expert committee of diabetologists has endorsed this position. 20
Our real-life study’s primary objective was assess the risk of maternal-fetal complications in type 1 diabetic women using isCGM or, in comparison, BGM. All the women had been referred to our Center for Pregnant Women with Diabetes before the application of the new guidelines on CGM. Our most striking finding was a significantly lower spontaneous abortions rate in the isCGM group than in the BGM group (5.3% vs. 20%, respectively; p = .0129), whereas the pre-pregnancy HbA1c level was similar in the two groups. There were no statistically significant differences in the frequency of other complications.
Even though we performed an observational, nonrandomized study, the women in the isCGM and BGM groups did not significantly differ with regard to their antenatal characteristics, except for the treatment modality. Indeed, there was a significantly higher proportion of patients on CSII in the isCGM group than in the BGM group. This might be because the indication for CSII is poorly controlled, glycemic instability and/or complicated diabetes; hence, CSII and isCGM might have been suggested before conception as a way of preparing for pregnancy. When restricting our analysis to patients treated with ambulatory CSII in both groups (isCGM: n = 64 and BGM: n = 46), we were able to demonstrate that there was a significant reduction in the rate of spontaneous abortion in the isCGM group compared with BGM (6.35% vs. 22.2%, p = .020). Recently, a meta-analysis of 24 trials (3104 pregnancies) revealed that the first-trimester HbA1c level was almost .5% lower in a CSII group than in an MDI group, although there was significant heterogeneity between studies during the first trimester (I2 = 7 8%), second trimester (I2 = 59%) and third trimester (I2 = 64%). 21 The American Diabetes Association recommends a pre-pregnancy HbA1c level of 6.5% (48 mmol/mol) or less or 6% (42 mmol/mol) or less in the absence of hypoglycemic episodes. 13 Over the last decade, several research groups have confirmed the favorable impact of good preconception metabolic control on maternal-fetal morbidity. 22 Most of the women in our study did not meet the preconception targets for metabolic control, and the difference between the mean values in the isCGM and BGM groups (7.1% ± 1.7 and 7.2% ± 1.2, respectively) was not significant.
Hence, near-optimal glycemic control (HbA1c ≤ 7.0% (53 mmol/L) is not good enough. 23 With regarding maternal-fetal complications, we observed that the spontaneous abortion rate was markedly lower for women isCGM than women using BGM. The intergroup differences in the prepregnancy and first-trimester HbA1c levels were not significant.
More recently, the CONCEPTT study randomized 325 women with T1D according to whether or not CGM was used. The pregnancy loss (<20 WG) rate was 5% in the CGM group and 4% in the control group. 9 These values are similar to that observed in our isCGM group but are much lower than that in our BGM group. Another observational cohort study of 186 pregnant women with T1D using either rtCGM (n = 92) or isCGM (n = 94) did not report data on spontaneous abortions. 24
The CARNATION study has investigated the effect of comprehensive T1D management on pregnancy outcomes. The spontaneous abortions/stillbirth rates were lower in the prospective interventional cohort (1.50%) than in the 2015–2017 retrospective cohort (20.7%; p < .001) and the 2012–2014 retrospective cohort (9.80%; p < .001). 25
In most published studies, the maternal HbA1c level was the only marker of metabolic control. According to the most popular hypothesis, glycemic imbalance increases the risk of chromosomal abnormalities at conception, placental abnormalities, malformations incompatible with embryonic or fetal survival, and thus miscarriage. 27 Other studies have highlighted a hypoglycemia-association elevation in the risk of first-trimester spontaneous abortion. The putative mechanisms involves an impaired supply of nutrients to the fetus, 28 and a potential teratogenic effect has been demonstrated in animal models. 29 However, the prospective, US-based DIEP study of 204,239 pregnant women with various types of diabetes and 316,332 non-diabetic pregnant women did not find a significant association between the spontaneous abortion rate and low HbA1c. This might have been because spontaneous abortion was related to short-term changes in blood glucose levels during the 8 weeks that can be monitored in the first trimester, whereas the red blood cells’ life span is longer (120 days, on average). HbA1c was therefore not considered to be a good marker of hypoglycemia in early pregnancy. 30
IMPACT study found that the use of isCGM was associated with more time spent on-target and less glycemic variability but not with a difference in HbA1c. 31 We speculate that even if HbA1c is not modified, a reduction in glycemic variability before conception and during the first trimester might influence the maternal-fetal outcomes – regardless of the treatment modality. We further hypothesize that glycemic variability during the first trimester might induce epigenetic modifications in the fetus and thus lead to fetal complications. Norgaard et al. recently demonstrated that the mean glucose levels reported by isCGM and rtCGM were similar. 32 However, the type of CGM device used might influence adjustments of the insulin dose, based on the level of concern about nocturnal hypoglycemia.
Along with evidence from randomized, controlled trials, real-world data on the use of rtCGM and isCGM monitoring in T1D pregnancies have confirmed the association between CGM and better neonatal outcomes. 10 A Swedish study of 186 women described the use of rtCGM (the Dexcom G4) and isCGM in pregnant women with T1D. Even though the incidence of LGA remained high study (53% in the isCGM group and 52% in the rtCGM group), a greater proportion of time in-range during the second and third trimesters was associated with a lower risk of LGA and a composite poor neonatal outcome. 24 Our study population was similar to those in the CONCEPTT study and in Kristensen et al.‘s study with regard to age, BMI, and diabetes duration. However, there were differences in the treatment modalities. We speculate that the lack of a significant difference in the maternal-fetal complications was due to the smaller number of patients included in our observational study.
The insulin requirements observed in our two study groups were similar to those reported in the literature on pregnant women with T1D. 33 We noted an increase in insulin requirements during pregnancy; this was doubtless due to the increase in insulin requirements up to the 35 WG threshold, after which insulin resistance decreases until the time of childbirth. There was a significant difference in the total insulin dose/weight ratio in the second trimester, which increased as the pregnancy progressed; the insulin requirement was greater in the BGM group than in the isCGM group. Unfortunately, the data on the insulin requirement were not reported in the GLucoMOMS study, in which a CGM device was compared with standard BGM. Our results differ from those of the CONCEPTT study, which showed that an improvement in glucose control was achieved without changing the total daily insulin dose. 9
Our study had various strengths. Firstly, we collected real-world clinical data. Even though the latest governmental guidelines now recommend that rtCGM should be offered to all pregnant women with T1D, real-world data on the impact of CGM are useful; they describe contemporary glucose levels in pregnant women with T1D and the levels’ relationships with specific pregnancy outcomes. For example, data on spontaneous abortion are not always collected in controlled trials randomized. Furthermore, it is difficult to obtain data on specific complications (like early fetal loss) in women with T1D even though the main factor is metabolic control (as evaluated by the HbA1c level) during the first 8 WG. Secondly, all the patients in our study were followed up by the same multidisciplinary team (a diabetologist, an obstetrician and a pediatrician). It is important to note that there is no difference between the 2 groups regarding the history of spontaneous abortion rate. Thirdly, our retrospective data collection reliably captured the history of spontaneous abortion because affected women with T1D had been specifically referred to our specialist center. Fourthly, all our HbA1c data were generated in the same hospital laboratory, which provided a robust dataset.
Our study also had some limitations. Firstly, our study’s retrospective and observational design prevented us from making causal interferences. These data are preliminary and will require larger studies to confirm the results. Secondly, the collection of data single-center, the long study period and the retrospective design of this study with some missing data and the number of patients in each group could generate a lack of power in statistical comparisons. Secondly, we did not evaluate many of the factors thought to increase the risk of spontaneous abortion, many of which were not; indeed, genetic causes, iatrogenic factors and autoimmune diseases have been described as risk factors for spontaneous abortion. The influence of active smoking on our study results cannot be ruled out, even though there was no significant different in the active smoking rate before pregnancy between the isCGM and BGM groups. We did not collect data on active smoking during pregnancy. Indeed, the risk of spontaneous abortion is 20%–80% higher in women who smoke during pregnancy. 34 Lastly, the study’s retrospective design prevented us from identifying episodes of maternal hypoglycemia in the pregnant women with T1D.
Conclusions
In the present study, we sought to gain local experience of CGM use during pregnancy because most women with T1D of childbearing age can now access this technology. Over time, CGM has become increasingly user-friendly. In France, some glucose sensors are now approved for use during pregnancy. Although the use of CGM is known to be associated with better pregnancy outcomes in T1D, more data are needed to explain the residual risk of maternal-fetal complications. CGM’s major impacts on metabolic control are mainly related to better glycemic control, fewer hypoglycemic episodes, and reduced glycemic variability throughout pregnancy. Indeed, the use of a CGM device to improve glycemic control and reduce glycemic variability in the periconceptional period might decrease the risk of maternal-fetal complications, such as spontaneous abortion. Given that spontaneous abortion has several causes, data on glucose levels gathered prospectively around the time of conception and in early pregnancy are needed to corroborate this hypothesis.
Footnotes
Acknowledgements
The authors thank the nurses at the Center for Pregnant Women with Diabetes (Céline Bergamaschi, Florence Commien, Iréne Hermann, and Nadége Sawicki) for their invaluable collaboration during the study. KF collected data. ML and AV wrote the manuscript. FB and DS reviewed the manuscript. AV initiated and directed the study and reviewed the manuscript. AV is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. The authors also thank the statistics advisor, Georges Alexandre.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent Statement
Informed consent was obtained from all study participants.