
Abstract
To provide synthesized evidence on the association of diabetes with clinical outcomes of patients with acute myocardial infarction (AMI) and associated cardiogenic shock (CS). We analyzed observational studies on patients with AMI and CS, identified through a systematic search using PubMed and Scopus databases. The main outcome was mortality and other outcomes of interest were risk of major bleeding, re-infarction, cerebrovascular adverse events, and need for revascularization. We conducted the meta-analysis with data from 15 studies. Compared to patients without diabetes, those with diabetes had an increased risk of in-hospital mortality (OR, 1.34; 95% CI, 1.17–1.54) and cerebrovascular complications (OR, 1.28; 95% CI, 1.11–1.48). We found similar risk of major bleeding (OR, 0.68; 95% CI, 0.43–1.09), re-infarction (OR, 0.98; 95% CI, 0.48–1.98) and need for re-vascularization (OR, 0.96; 95% CI, 0.75–1.22) as well as hospital stay lengths (in days) (WMD 0.00; 95% CI, −0.27–0.28; n = 4; I2 = 99.7%) in the two groups of patients. Patients with diabetes, acute MI and associated cardiogenic shock have increased risks of mortality and adverse cerebrovascular events than those without diabetes.
Keywords
Introduction
Cardiogenic shock (CS) is responsible for high rates of in-hospital mortality among patients with acute myocardial infarction (MI).1,2 Approximately 5–10% of patients with acute myocardial infarction develop CS.1–3 Acute MI is present in more than 4/5 of the patients with CS. 4 Cardiogenic shock is characterized by severely abnormal cardiac activity resulting in reduced cardiac output with hypotension, end-organ hypoperfusion, and critical hypoxia.1,2,5 An important feature of CS that differentiates it from other types of shock is that it is usually unresponsive to fluids or volume resuscitation.1,2
The underlying mechanisms of cardiogenic shock among patients with MI are not fully understood. The decreased myocardial activity during cardiogenic shock substantially reduces the cardiac output and results in hypotension, peripheral vasoconstriction, end-organ damage, and cardiac ischemia.1,6 Peripheral vasoconstriction initially improves the coronary perfusion, but later on, it leads to increased cardiac afterload, thereby damaging the myocardium even more. 6 In addition, accompanying systemic inflammation with release of NO (nitric oxide), interleukins, and TNF (tumor necrosis factor)-alpha exerts a cardiotoxic effect.6,7
Several CS risk factors have been documented. These include older age, presence of diabetes, previous infarction, anterior and large infarct, and peripheral vascular disease.2,8–10 Out of these factors, diabetes increases the risk of developing CS by approximately 2–3 times that of patients without diabetes. 11 Studies have suggested a strong link between diabetes and cardiovascular diseases. 12 Patients with diabetes frequently have obesity, abnormal lipid levels, and high blood pressure, all conditions that increase their risk for adverse cardiac events.13–15 However, whether the presence of diabetes alters the prognosis in patients with cardiogenic shock remains unclear. The current meta-analysis is probably the first attempt to synthesize the evidence on the effects of diabetes on clinical outcomes among patients with cardiogenic shock.
Materials and methods
Search strategy
We ensured our study processes complied with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) guidelines. 16 The protocol was registered in the International Prospective Registry of Systematic Reviews (PROSPERO; registration number CRD42021286109). We carried out a systematic search of PubMed and Scopus databases for English language papers published until 10th November 2021. The search strategy used included the following terms: (cardiogenic shock OR, myocardial infarction) AND (diabetes mellitus OR diabetes OR high blood glucose) AND (mortality OR death OR survival OR clinical outcomes OR all-cause mortality OR need for revascularization OR need for thrombolysis). We aimed at identifying studies that examined the association of diabetes with outcomes of interest in patients with acute myocardial infarction (MI) and associated cardiogenic shock (CS). Mortality was the main outcome of interest, whereas risk of major bleeding, re-infarction, cerebrovascular adverse events, and the need for revascularization were other outcomes of potential interest.
Selection criteria and methods
The first step was to remove the duplicates and arrive at the unique citations identified through the systematic search of the databases. This was followed by two study authors independently screening the title and abstract of the studies. As a subsequent step, the full text of suitable studies was reviewed in detail. In case of any disagreements pertaining to the inclusion of studies, the two authors arrived at a mutual consensus upon discussion. The reference/bibliographic list of the included studies was also reviewed in an attempt to identify additional studies for inclusion.
We considered observational studies, including those based on analysis of registry data or clinical records for inclusion. All the studies considered were done in patients with MI and associated cardiogenic shock that mentioned the association of diabetes with the outcomes of interest.
We excluded case-reports, review articles, and studies that did not provide findings based on diabetes status.
Statistical analysis including data extraction and quality assessment
We used a pretest data extraction sheet to fill in relevant data from the included studies. This process of data extraction was carried out by two study authors independently. The quality assessment of the studies was done using the Newcastle-Ottawa Quality Assessment Scale for observational studies. 17
We used STATA version 16.0 for all the statistical analyses. For the primary outcome i.e. mortality, we included only those studies that reported adjusted risk of mortality. We considered some set of variables (such as age, sex, treatment modality adopted, presence of comorbidities, previous history of myocardial infarction, prior coronary artery bypass, any fluid or electrolyte disorder, presence of obesity/body mass index) that should preferably be adjusted for. Studies that adjusted for some or most of these variables were included for analysis.
The pooled effect sizes, along with 95% confidence intervals (CI), were reported as odds ratios (ORs) for categorical outcomes and weighted mean differences (WMDs) for continuous outcomes. Selection of the final analytic model was based on the observed value of I2 (used to denote the degree of heterogeneity) For outcomes where I2 value exceeded 40%, we applied a random effects model and where it was ≤40%, we used fixed effects model. 18 We considered p-values lower than 0.05 as representing statistical significance. Presence or absence of publication bias was assessed using Egger’s test. 19
Results
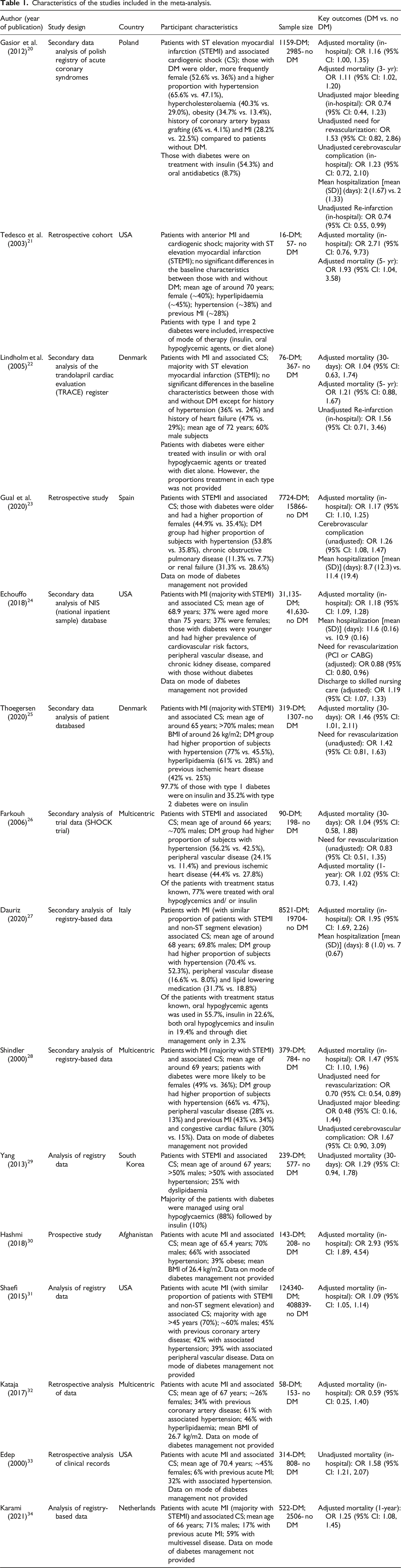
We identified 1077 citations after our initial search and elimination of duplicates. We analyzed the data from 15 studies.20–34 Specific steps in the process of selection of articles have been detailed in Figure 1. Included studies had an observational study design (Table 1). All, except one, presented data either from registry or clinical records. The study by Hashmi et al. was prospective in design (30). Three studies were multicentric, 4 were done in the USA and 2 in Denmark. The others were each conducted in Poland, Spain, Italy, South Korea, Afghanistan, and the Netherlands (Table 1). In almost all the studies, the study participants presented ST-segment elevation MI (STEMI). The included studies were judged to have good quality (Supplementary tables 1 and 2). Selection process of the studies included in the review. Characteristics of the studies included in the meta-analysis.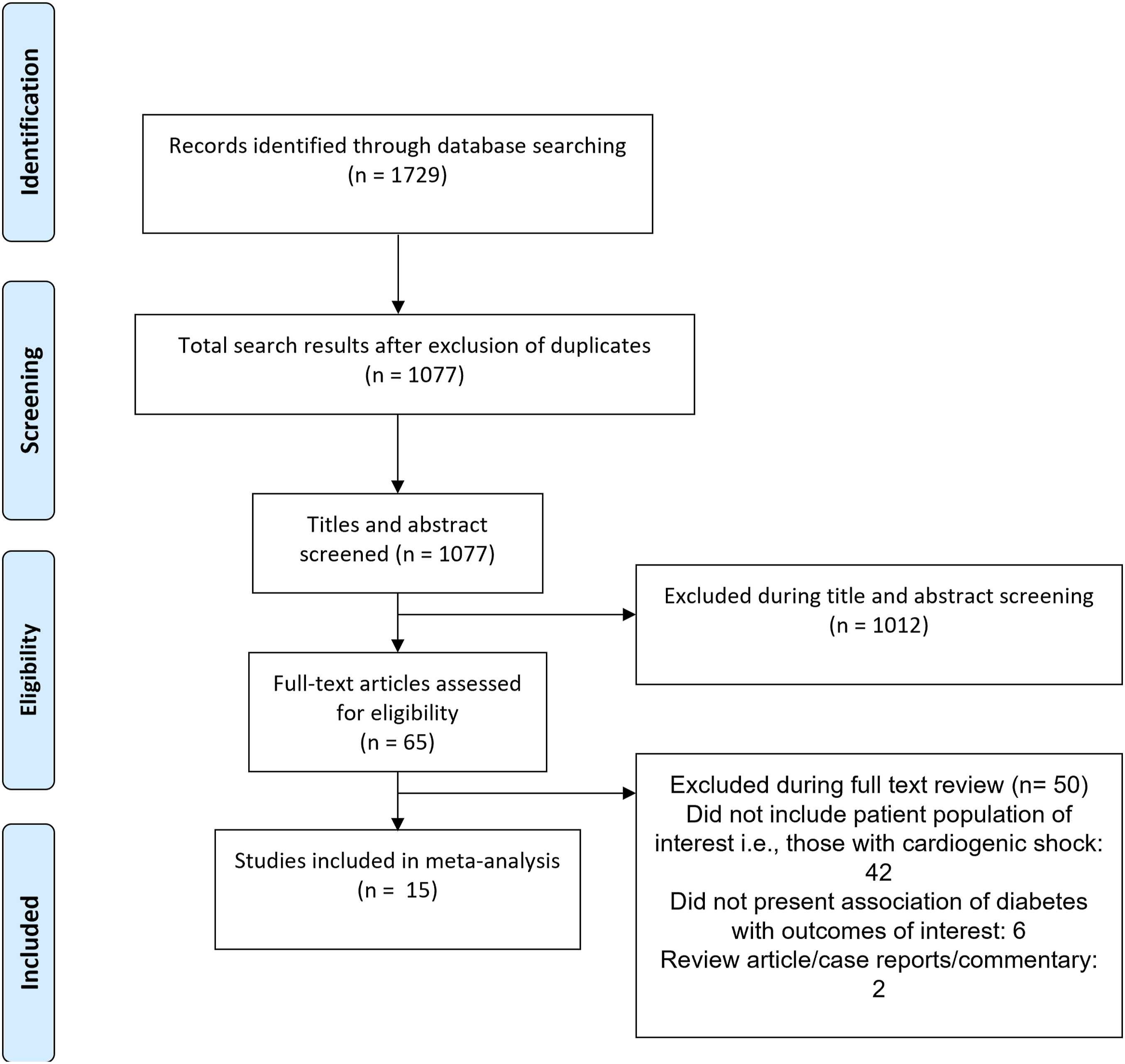
Association of diabetes with mortality in patients with cardiogenic shock
Compared to the patients without diabetes, those with diabetes had an increased risk of in-hospital mortality (OR, 1.34; 95% CI, 1.17, 1.54; n = 9; I2 = 90.2%). The increased risk of mortality was also noted at 30-days post discharge (OR, 1.24; 95% CI, 0.95, 1.62; n = 3; I2 = 0.0%) and at 1-year post-discharge (OR, 1.20; 95% CI, 1.01, 1.41; n = 2; I2 = 16.7%) (Figure 2). The increased risk of mortality persisted beyond 12 months of the post-operative period (OR, 1.19; 95% CI, 0.98, 1.45; n = 3; I2 = 38.1%) (Figure 2). For these outcomes, we did not find any statistical evidence of publication bias (p > 0.05) Pooled risk of mortality among individuals with cardiogenic shock with or without diabetes.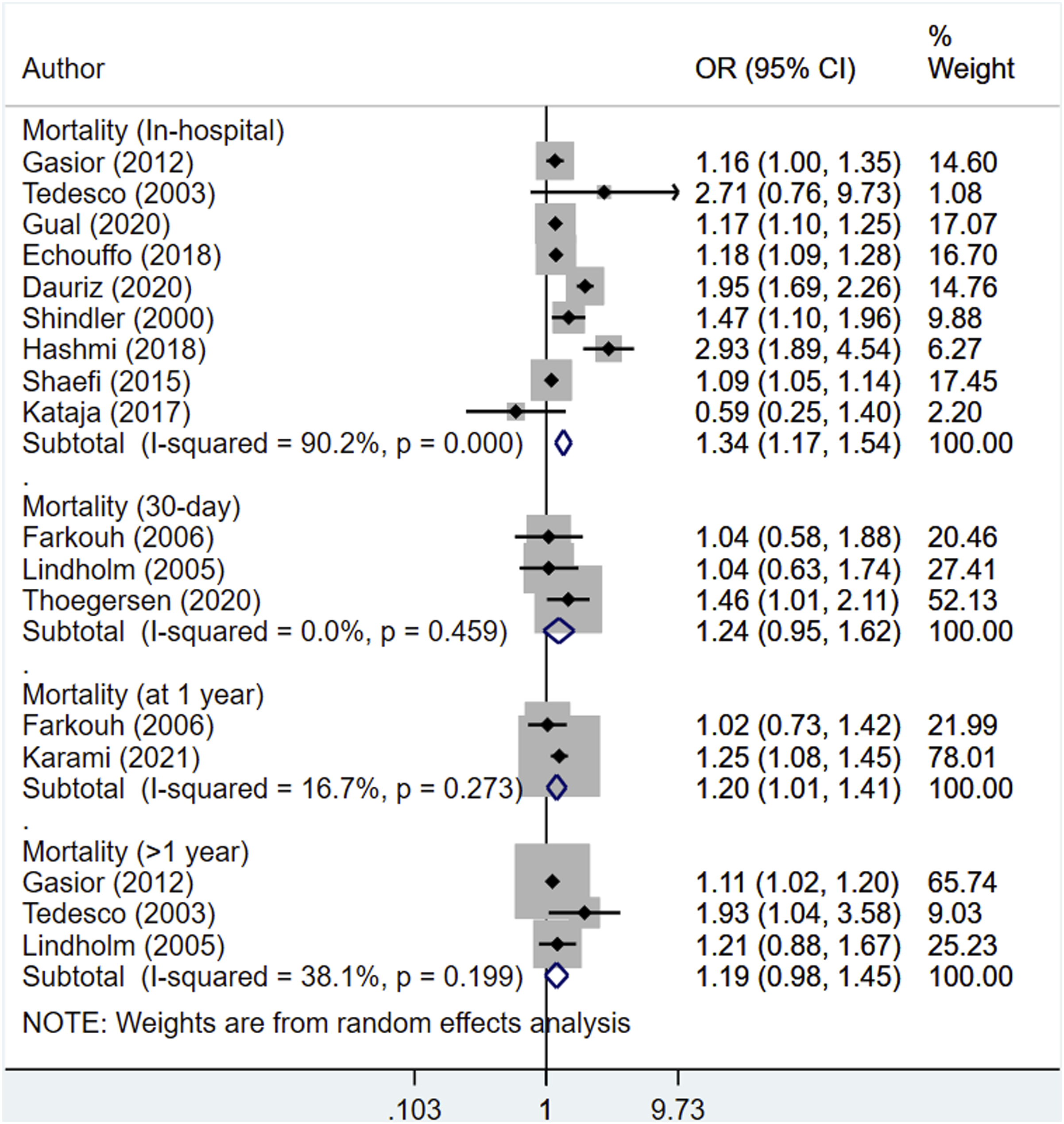
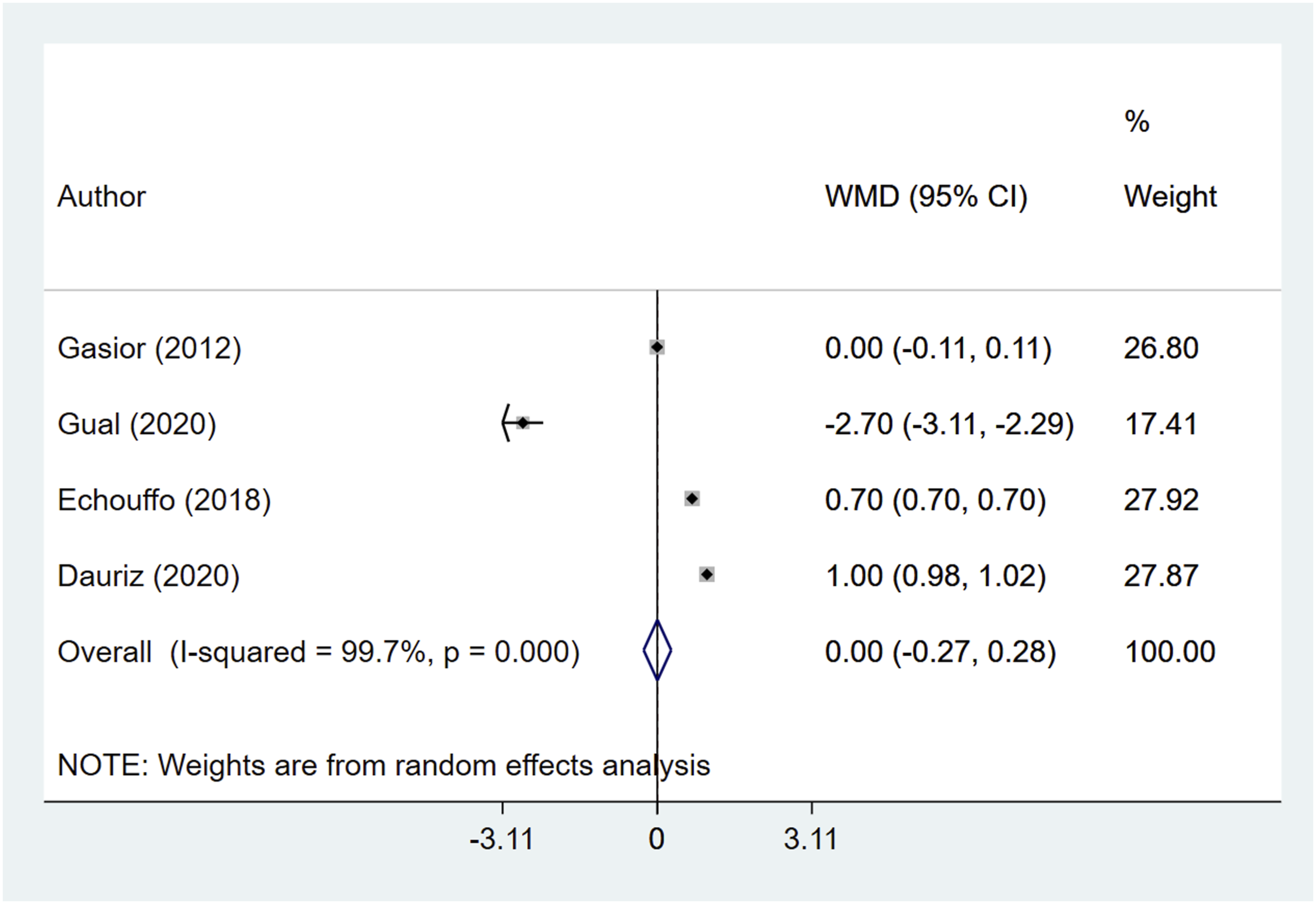
Association of diabetes with adverse outcomes and length of hospital stay in patients with cardiogenic shock
Compared to the patients without diabetes, those with diabetes had an increased risk of cerebrovascular complications (OR, 1.28; 95% CI, 1.11, 1.48; n = 3; I2 = 0.0%) (Figure 3). We found similar risks of major bleeding (OR, 0.68; 95% CI, 0.43, 1.09; n = 2; I2 = 0.0%) and re-infarction (OR, 0.98; 95% CI, 0.48, 1.98; n = 2; I2 = 66.6%) as well as similar re-vascularization needs (OR, 0.96; 95% CI, 0.75, 1.22; n = 5; I2 = 70.2%) in both groups of patients (Figure 3). We found no evidence of publication bias for the above outcomes (p > 0.05). Moreover, we found similar hospital stay lengths (in days) (WMD 0.00; 95% CI, −0.27, 0.28; n = 4; I2 = 99.7%) regardless of the presence of diabetes (Figure 4). Pooled risk of adverse outcomes among patients with cardiogenic shock with or without diabetes. Length of hospital stay (in days) among patients with cardiogenic shock with or without diabetes.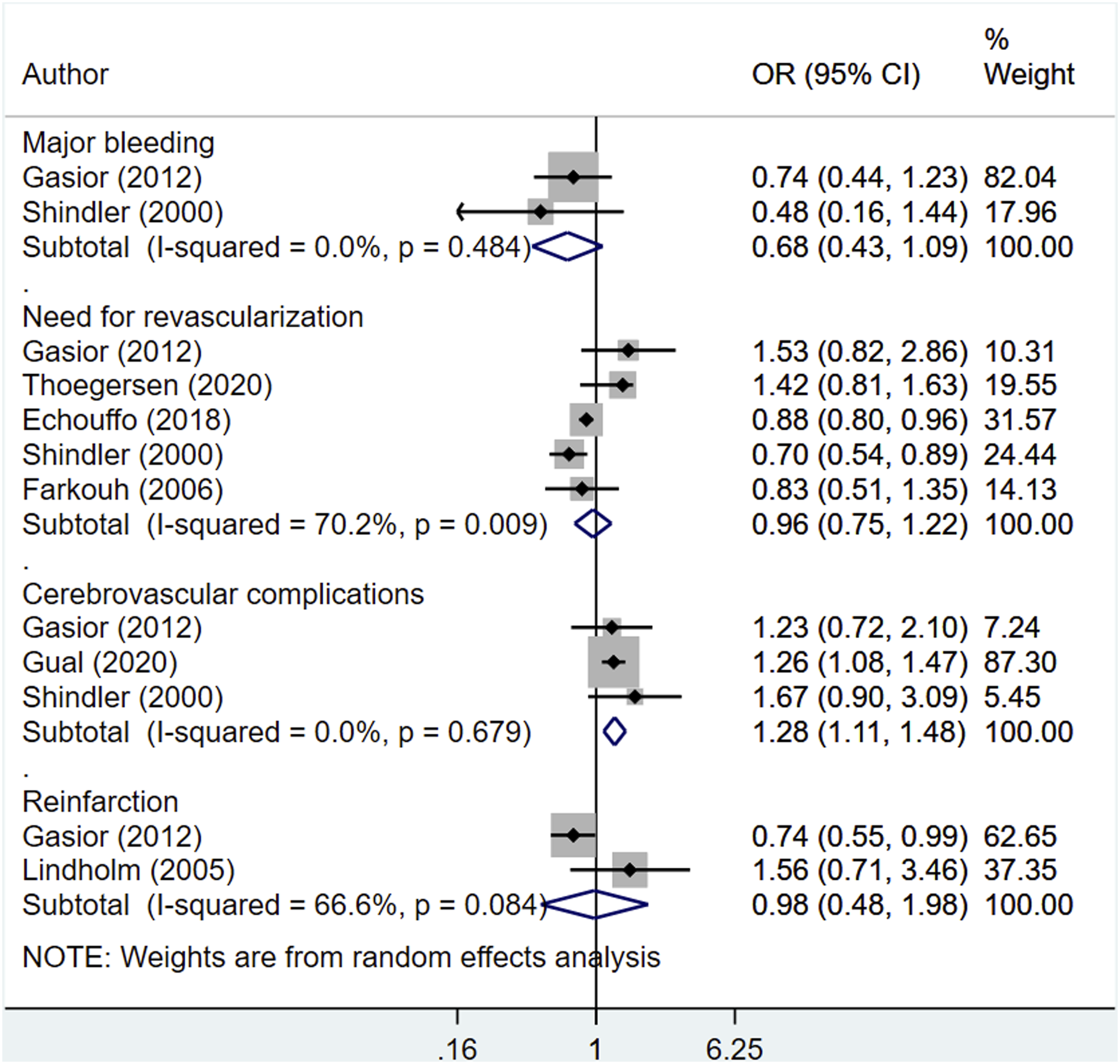
Discussion
There has been a global upsurge in the incidence of diabetes mellitus. According to the Global Burden of Disease estimates, the worldwide incidence of diabetes was close to 23 million in the year 2017. 35 The incidence of acute myocardial infarction complicated with cardiogenic shock is 3–10% and has remained stable over the years.9,36,37 Patients with diabetes mellitus have a 2-3 times higher risk of cardiogenic shock than individuals without diabetes. 11 We conducted this meta-analysis to provide updated evidence on the influence of diabetes on outcomes of patients with acute MI and cardiogenic shock. Our findings suggest that the presence of diabetes in patients with acute MI and cardiogenic shock raises their risk for in-hospital mortality as well as mortality in the follow-up period (during at least 12 months post-operatively). Further, the presence of diabetes increases the risk of adverse cerebrovascular events. These findings underscore the need for better care and follow-up in patients with diabetes.
While we noted a poor survival among patients with diabetes, the underlying mechanisms through which diabetes may underlie other diseases is still under investigation. One possibility is that diabetes leads to extensive pre-existing coronary artery disease (CAD) and multivessel involvement due to its ability to induce micro- and macrovascular changes. 38 Studies have also suggested that individuals with diabetes may have a comparatively larger infarct size, substantially reduced reperfusion, and a heightened susceptibility to arrhythmias of the ventricle than individuals without diabetes.39–41 In addition, hyperglycemia triggers the stress response, increasing levels of circulating cytokines and the leucocyte count. 42 Moreover, leukocytosis has been associated with increased risk of mortality in patients with STEMI. 42 Another factor that could partially explain the poor outcomes in individuals with diabetes is the low left ventricular function reserve in diabetic cardiomyopathy. 43 The underlying inflammation and micro- and macro vessel changes due to diabetes and associated hyperglycemia possibly explain the increased risk of adverse cerebrovascular events we found in this review.
Adequate glycemic control is of utmost importance as the evidence suggests that normoglycemic patients tend to have only mild abnormalities in arterial PH and lactate levels indicating less severe hypoperfusion than patients with hyperglycemia. 44 Stress-related hyperglycemia has been associated with increased risk of developing cardiac failure, cardiogenic shock, and death.32,44 Hyperglycemia may be considered a reliable sign of deranged homeostasis. Management of hyperglycemia is important and insulin therapy provides adequate glycemic control and may offer additional benefits through its positive ionotropic effect on the heart. 45 Moreover, studies in animal models have suggested that insulin has an anti-apoptotic effect on myocytes in the presence of ischemia. 46 An important practical challenge is to identify “persons-at-risk” with STEMI complicated by cardiogenic shock. One of the most commonly used tools is the GRACE risk score applicable during all forms of acute coronary syndrome. 47 The TIMI risk score for STEMI is another alternative, derived from its application to patients treated with fibrinolytics. 48 However, a robust risk model that is thoroughly applicable to the whole of the population is still needed.
We are aware of the limitations of this meta-analysis. As included studies had an observational design and many of them used data collected as part of registry or used data from clinical records, the possibility of important variables or potential confounder(s) being not accounted for in the final analytic model cannot be ruled out. Because almost all the studies had patients with STEMI, subgroup analyses based on the nature of MI (non-ST elevation MI and STEMI) could not be done. Also, the included studies had a heterogenous diabetes population (type 1 or type 2) and their results were not stratified based on these. This prevented us from performing subgroup analyses based on type of diabetes. It is clinically well known that patients with acute myocardial infarction and associated cardiogenic shock have a poor prognosis. Further, if there is associated diabetes, then the prognosis is even poorer. Based on these considerations, an analysis based on the mode of management of diabetes would have helped to understand this issue better. However, most of the studies did not provide required information on the mode of diabetes management. While some studies provided this information, majority of them did not furnish data on the management of diabetes in patients with diabetes. This is an important limitation as in general practice, clinical management of diabetes is quite heterogenous and this might have influenced the outcomes. It would also have been desirable to conduct an analysis based on blood glucose level at admission and HbA1c (%) but the studies lacked the relevant variables. Another limitation stems from the differences in the baseline socio-demographic and clinical characteristics among the patients with diabetes and those without diabetes. It was not completely clear whether the researchers of the studies in our analyses had adjusted for these differences or how these differences impacted the final effect sizes reported. For the analysis related to the primary outcome (mortality), we included studies that had presented adjusted risk estimates. However, we could not follow the similar principle for the secondary outcomes as almost all the included studies had presented unadjusted measures of risk. Therefore, especially for the secondary outcomes, the interpretation must be made cautiously as unadjusted estimates are likely to be biased.
Conclusions
Our current meta-analysis, after synthesizing the findings from 15 observational studies, suggests an increased risk of mortality for patients with acute MI with associated cardiogenic shock if they also present diabetes. The findings stress the need for close and careful monitoring of patients with AMI and associated CS. More research is needed to identify optimal management strategies for improving survival of such patients.
Supplemental Material
Supplemental Material - Impact of diabetes on outcomes of cardiogenic shock: A systematic review and meta-analysis
Supplemental Material for Impact of diabetes on outcomes of cardiogenic shock: A systematic review and meta-analysis by Chao Luo, Feng Chen, Lingpei Liu, Zuanmin Ge, Chengzhen Feng and Yuehua Chen in Diabetes and Vascular Disease Research
Footnotes
Author contributions
CL, FC conceived and designed the study; LL, ZG, CF and YC were involved in literature search and data collection; FC, LL, ZG and CF analyzed the data; CL and YC wrote the paper; and YC reviewed and edited the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Jinhua City Science and Technology Plan Project Social Development Key Project (2019-3–007).
Inclusion Criteria
We considered observational studies, including those based on analysis of registry data or clinical records for inclusion. All the studies considered were done in patients with MI and associated cardiogenic shock that mentioned the association of diabetes with the outcomes of interest.
Exclusion Criteria
We excluded case-reports, review articles, and studies that did not provide findings based on diabetes status that failed to provide findings on the outcomes of interest.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.