
Abstract
Objective
This meta-analysis evaluated the efficacy and safety of nesiritide in patients with acute myocardial infarction (AMI) and heart failure.
Methods
PubMed, Embase, and the Cochrane Central Register of Controlled Trials were searched from inception through December 2018. Studies including patients with AMI and heart failure who received nesiritide were identified.
Results
Ten trials involving 870 participants were included in this meta-analysis. Nesiritide treatment significantly increased left ventricular ejection fraction, cardiac index, and 24- and 72-hour urine volumes. Additionally, pulmonary capillary wedge pressure, right atrial pressure, and brain natriuretic peptide and N-terminal brain natriuretic peptide levels were significantly decreased in patients treated with nesiritide compared with those treated with control drugs. However, patients treated with nesiritide did not have an increased risk of mortality compared with those treated with control drugs. There were no differences between the two groups with respect to heart rate or the risk of readmission, hypotension, or renal dysfunction.
Conclusions
Nesiritide appears to be safe for patients with AMI and heart failure, and it improves global cardiac and systemic function.
Keywords
Introduction
Heart failure is a major public health concern linked to increasing morbidity, and it represents a growth health burden globally.1,2 It is a complex clinical syndrome that can result from a variety of heart diseases. 3 Among all causes of heart failure, acute myocardial infarction (AMI) can directly lead to heart dysfunction, owing to necrosis, apoptosis, and deletion of myocardial cells caused by the infarction. Although emergency revascularization with percutaneous coronary intervention (PCI) has proven effective for treating AMI, heart failure still occurs after PCI. Heart failure is currently one of the most severe complications of AMI, and it leads to higher in-hospital mortality. Therefore, patients with AMI and heart failure are commonly encountered in clinical practice.
Many drugs used to treat acute heart failure after AMI can increase myocardial oxygen consumption and the risks of arrhythmia and mortality while increasing cardiac output.4,5 The safety of these drugs in the treatment of AMI complicated by heart failure has received extensive attention. In addition to the traditional treatment of heart failure using diuretics, vasodilators, and other oral agents, new drugs are constantly being developed. Nesiritide, a recombinant B-type natriuretic peptide, was approved by the US Food and Drug Administration for the treatment of acute decompensated heart failure in 2001. 6 It has been widely used since its approval7–9 owing to its potent effects on natriuresis, diuresis, and vasodilation, in addition to reducing cardiac pre-load, increasing cardiac output, inhibiting the renin-angiotensin-aldosterone system,10–13 and improving ventricular remodeling. 14 In recent years, numerous studies have investigated the safety of nesiritide in patients with heart failure, but no consistent conclusions were drawn. Several reviews suggested that nesiritide therapy was associated with lower in-hospital mortality and readmission rates in patients with heart failure.15–17 However, other recently published meta-analyses indicated that nesiritide was not associated with a change in the risk of mortality compared with the effects of control treatments.13,18,19 The difficulty in reaching definitive conclusions may be attributable to the different drugs used in the control groups and the characteristics of the different participants included in each study. Among these studies, several investigated the role of nesiritide in treating patients with AMI and heart failure, but no consistent conclusions were drawn. Therefore, we performed a meta-analysis of randomized controlled trials (RCTs) that compared nesiritide with other anti-heart failure agents to evaluate its efficacy and safety in patients with AMI and heart failure.
Methods
Literature search and study selection
The following databases were searched from inception through December 2018: PubMed, Embase, and the Cochrane Central Register of Controlled Trials (CENTRAL). The following key words were used for the database searches: nesiritide, natriuretic peptide brain, recombinant human brain natriuretic peptide (rhBNP), myocardial infarction, heart infarction, heart failure, cardiac failure, and randomized controlled trial. An additional manual search was also performed using Google Scholar and the Chinese Wan Fang Database.
Studies were assessed for suitability using the following inclusion criteria: 1) only patients with AMI and heart failure were included, 2) patients received nesiritide as a treatment, 3) the study design was an RCT, 4) one or more efficacy and/or safety outcomes were reported in the individual trials, and 5) the language used for the individual studies was English or Chinese. Only studies with full text available online were included in the meta-analysis. The major exclusion criteria were systematic reviews, case reports, and studies with animal data.
Two authors independently performed the search processes and study selection according to the aforementioned criteria. Discrepancies were settled by discussion or by consultation with a third reviewer.
Assessment of risk of bias and data extraction
Two reviewers independently evaluated the risk of bias and collected the data from each study. The Cochrane risk of bias tool was used to assess the quality of each trial included in the meta-analysis. Seven biases were included in the tool: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other biases. Results were presented as low, high, or unclear risk using the Cochrane risk of bias tool. Any disagreement regarding the evaluation was resolved by discussion.
The following baseline information was extracted from each included study: first author, publication year, study period, study design, participants, sample size, test group dosage, control group dosage, follow-up time, and number of outcomes.
Statistical analyses
Review Manager software (version 5.3) was used to perform all statistical analyses. The Mantel–Haenszel method was used for dichotomous outcomes, and the inverse variance method was used for continuous outcomes. The pooled effect was calculated using the risk ratio (RR) with 95% confidence intervals (CIs) for dichotomous outcomes and the mean difference (MD) with 95% CIs for continuous outcomes. Heterogeneity was measured using the I2 test. I2 < 50% indicated homogeneity, and a fixed-effect model was used; otherwise, a random-effect model was selected. P < 0.05 was regarded as statistically significant in all our estimations, and the publication bias was assessed by drawing funnel plots.
Results
Literature search and study selection
A total of 837 published studies were identified in the three databases (PubMed = 343, Embase = 101, and CENTRAL = 393). In addition, 12 records were identified through other sources. After removing duplicates, 657 records remained. After reading the titles and abstracts, 640 studies were excluded, leaving 17 studies for further review. Another seven studies were further removed because they satisfied the exclusion criteria. A total of 10 studies involving 870 participants were included in the meta-analysis.14,20–28 The study selection process is shown in Figure 1.

Flowchart of the study selection process for the meta-analysis.
Characteristics and data extraction for the studies
Table 1 shows the basic characteristics of the 10 included studies. The publication years ranged from 2006 to 2017. All studies were conducted in China, and all participants were Asian. All studies were designed as RCTs. The study period of each trial was at least 1 year. The detailed characteristics of the participants for each individual trial are shown in Table 1. Patients with AMI mainly presented with ST-segment elevation myocardial infarction or non-ST elevation myocardial infarction, and they were deemed to have Killip class II to IV heart failure. Trials that mentioned left ventricular ejection fraction (LVEF) at enrollment involved patients with heart failure and reduced ejection fraction. Trials that mentioned the type of revascularization referred to patients with PCI and a similar time-to-reperfusion. Thus, the two patients groups were considered comparable.
Characteristics of the 10 studies included in this meta-analysis

Abbreviations: NA, not available; AMI, acute myocardial infarction; LVEF, left ventricular ejection fraction; PCI, percutaneous coronary intervention; HFrEF, heart failure with reduced ejection fraction; STEMI, ST-segment elevation myocardial infarction; NSTEMI, non-ST elevation myocardial infarction.
The basic data extracted from each study are shown in Table 2. Four studies had sample sizes of more than 100 subjects.20,25–27 The dose administered to the experimental group was similar in each individual study. However, the drug dose in the control group differed, and the drugs used in the control groups were different. Three studies involved a follow-up time of 3 months or longer,20,25,28 whereas five studies involved a follow-up shorter than 3 months.21–24,27 The number of outcomes was also calculated (Table 2).
Data extraction from the 10 studies included in this meta-analysis

Abbreviations: rhBNP, recombinant human brain natriuretic peptide; NA, not available.
Risk of bias assessment of the included studies
Quality assessments were performed for the 10 included studies. The detailed assessment of each individual study is illustrated in Figure 2, and the summary assessment is shown in Figure 3. Six of the studies provided specific sequence generation methods,22,24–28 and the remaining four studies had an unclear risk of bias in this domain.14,20,21,23 Seven studies had an unclear risk of bias for allocation concealment,14,20,21,23–26 whereas the other three trials had a low risk.22,27,28 Concerning performance or detection bias, we found a low risk of bias in all of the included studies. In terms of attrition bias, two studies14,26 had an unclear risk of bias, and the remaining studies20–25,27,28 had a low risk of bias. Regarding reporting bias, only one study had a high risk of bias. 14 No other risk of bias was identified across the included studies. Our results indicated that most of the included studies had a low risk of bias.

Risk of bias graph of studies comparing nesiritide and control groups.

Risk of bias summary of studies comparing nesiritide and control groups.
Efficacy outcomes
Table 3 summarizes the meta-analysis outcomes comparing nesiritide with control drugs in patients with AMI and heart failure. Our results indicated that treatment with nesiritide significantly increased LVEF (MD = 3.29; 95% CI = 2.05–4.54; P < 0.00001) and the cardiac index (MD = 0.20; 95% CI = 0.07–0.32; P = 0.003) compared with the effects of control treatment. The 24- (MD = 277.11; 95% CI = 143.72–410.49; P < 0.0001) and 72-hour urine volumes (MD = 409.43; 95% CI = 199.54–619.32; P = 0.0001) were significantly higher in patients who received nesiritide than in those who received control treatment. Nesiritide significantly decreased pulmonary capillary wedge pressure (PCWP; MD = −5.47; 95% CI = −9.25 to −1.69; P = 0.005) and right atrial pressure (RAP; MD = −1.50; 95% CI = −2.31 to −0.69; P = 0.0003) compared with the effects of control treatment. The levels of heart failure biomarkers, namely brain natriuretic peptide (BNP; MD = −84.18; 95% CI = −151.4 to −16.97; P = 0.01), and N-terminal brain natriuretic peptide (NT-proBNP; MD = −1478.16; 95% CI = −2192.29 to −764.02; P < 0.0001) were significantly lower in patients who received nesiritide than in those who received control medication.
Summary of meta-analysis outcomes comparing nesiritide with control drugs in patients with AMI patients and heart failure

Abbreviations: AMI, acute myocardial infarction; LVEF, left ventricular ejection fraction; CrIn, cardiac index; PCWP, pulmonary capillary wedge pressure; RAP, right atrial pressure; BNP, brain natriuretic peptide; NT-proBNP, N-terminal brain natriuretic peptide; MACE, major adverse cardiovascular events; HR, heart rate; SBP, systolic blood pressure; DBP, diastolic blood pressure; SCr, serum creatinine; Cys-C, cystatin C; eGFR, estimate glomerular filtration rate; CI, confidence interval; I2, heterogeneity.
Safety outcomes
None of the safety outcomes was significantly different between the nesiritide and control groups (Table 3). The risk of mortality was discussed in nine trials, and no difference was observed between the two groups (RR = 0.92; 95% CI = 0.46–1.83; Figure 4). Subgroup analysis was further performed according to the different follow-up times in each individual trial, and the results revealed no significant difference in the risk of mortality (RR = 1.17; 95% CI =, 0.51–2.70) between the nesiritide and control groups when the follow-up time was less than 3 months (Figure 5). However, in the subgroup with a follow-up time of 3 months or longer, patients in the nesiritide group had an insignificantly lower risk of mortality (RR = 0.55; 95% CI = 0.15–1.96; P = 0.35). Figure 6 compares the risk of mortality after treatment with nesiritide and nitroglycerin. Similarly, patients in the nesiritide group had an insignificantly lower risk of mortality (RR = 0.64; 95% CI = 0.17–2.37; P = 0.50).
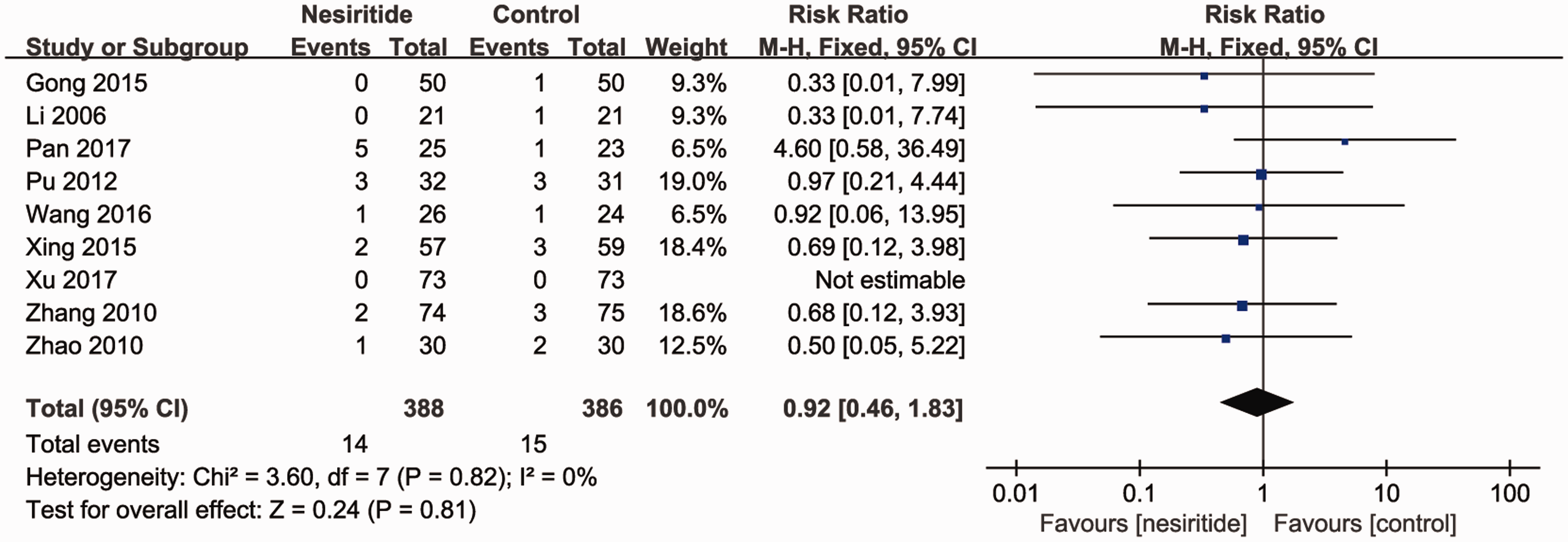
Risk of mortality between nesiritide and control groups.

Subgroup analysis for risk of mortality between nesiritide and control groups.
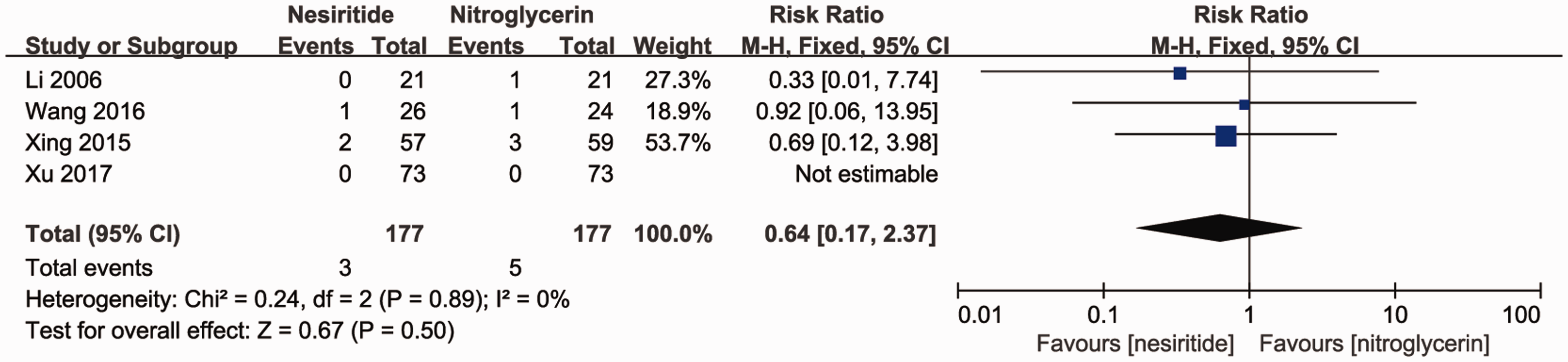
Risk of mortality between nesiritide and nitroglycerin.
No significant difference was found between the nesiritide and control groups regarding the risk of readmission (RR = 0.78; 95% CI = 0.30–2.03; Figure 7). Patients treated with nesiritide had a lower risk of hypotension (RR = 0.63; 95% CI = 0.25–1.63), although this difference was not statistically significant (Figure 8). There were no significant differences in the risks of major adverse cardiovascular events (MACE; RR = 0.64; 95% CI = 0.38–1.08) or ventricular tachycardia (RR = 1.61; 95% CI = 0.22–11.91) between the two groups. Ventricular extrasystole, cardiac arrest, bradycardia, and angina pectoris were not reported in any of the included studies. Figures 9 and 10 illustrate the results of the funnel plots.

Risk of readmission between nesiritide and control groups.

Risk of hypotension between nesiritide and control groups.

Funnel plot of risk of mortality between nesiritide and control groups.

Funnel plot of subgroup analysis of the risk of mortality between nesiritide and control groups.
The occurrence of other adverse events such as changes in heart rate (HR; MD = −0.39; 95% CI = −2.40–1.61), systolic blood pressure (SBP) (MD = −1.18; 95% CI = −4.97–2.62), and diastolic blood pressure (DBP; MD = −0.39; 95% CI = −6.60–5.81) was not significantly different between the two groups. No significant differences were found in sodium (MD = −1.77; 95% CI = −5.69–2.15) and potassium levels (MD = 0.13; 95% CI = −0.08–0.33) between the nesiritide and control groups. Serum creatinine (SCr) levels were lower in patients who received nesiritide than in those who received control treatments (MD = −5.46; 95% CI = −12.11–1.18); however, the difference was not statistically significant. Other renal function indicators, such as cystatin C (Cys-C) levels (MD = −0.01; 95% CI = −0.19–0.17) and the estimated glomerular filtration rate (eGFR; MD = 1.12; 95% CI = −2.64–4.88), were also not significantly different between the two groups. The risk of renal dysfunction did not differ between the two groups (RR = 1.81; 95% CI = 0.18–18.12), and no cases of dialysis were noted. Regarding non-cardiovascular adverse events, only one study reported the risk of headache, and no studies reported the risk of nausea, abdominal pain, or dyspnea.
Sensitivity analysis
The study published by Xu et al. 26 reported NT-proBNP levels 4 hours after treatment; however, another three studies14,22,28 provided NT-proBNP levels more than 24 hours after treatment. The study by Xu et al. 26 was a major source of heterogeneity across the four studies; therefore, the sensitivity analysis was performed after excluding their study. The sensitivity analysis confirmed the robustness of this result; that is, nesiritide significantly decreased NT-proBNP levels compared with the effects of the control drugs (MD = −1747.17; 95% CI = −1748.18 to −1746.15; P < 0.00001), whereas I2 decreased from 98 to 0.
Discussion
Heart failure is a complex clinical syndrome that affects systemic organs. Patients with heart failure who have experienced AMI are commonly encountered in clinical practice. Drugs used to treat these diseases need to improve heart failure without increasing myocardial oxygen consumption, mortality, or other adverse reactions. Vasodilators constitute one of the three main pharmacological agents used in the treatment of decompensated heart failure, followed by diuretics and, when indicated, inotropic agents. The goal of therapy for heart failure using vasodilators is to guarantee cardiac output and the perfusion of peripheral organs including the kidneys, lungs, and brain. Their effects are mediated by the increase in LVEF and other variables. In an era in which the heart can be studied using several multimodality imaging approaches,29,30 a global assessment of patient features is extremely important for targeted therapies and better heart failure management. Nesiritide has been widely used for the treatment of heart failure, and numerous studies have investigated its role in the treatment of patients with AMI and heart failure. However, no consistent conclusions have been drawn. What is the role of nesiritide in patients with AMI complicated by heart failure? Is it safe? The major difference between our study and previous meta-analyses was that our study focused on “patients with AMI and heart failure” rather than “patients with heart failure.” Our results indicated that nesiritide treatment was significantly more effective than control treatments for patients with AMI and heart failure because it increased LVEF, the cardiac index, and 24- and 72-hour urine volumes and decreased cardiac preload and the levels of heart failure markers. The effect of nesiritide on PCWP and RAP was similar to that in several previous studies.11,13,31 An increased ejection fraction and increased urine output are other important indicators of effective heart failure treatment, and the results were similar to those of a previous study. 19 In addition, because BNP and NT-proBNP are major markers of heart failure,32–34 we further analyzed their levels for the first time and observed significant differences. In summary, our results indicated that nesiritide significantly improved cardiac function and increased urine volume in patients with AMI and heart failure. However, only four studies reported efficacy outcomes; therefore, additional evidence is needed to confirm these findings.
Several safety outcomes, including the risks of mortality, readmission, and hypotension, as well as HR, BP, and renal function, were also evaluated in this meta-analysis. Similarly as previous studies,13,18,35 no differences in mortality were observed between the nesiritide and control groups. We performed a further detailed analysis of mortality according to the follow-up duration. Our findings revealed no difference between the two groups even after subgroup analysis. Additionally, the drugs used in the control groups differed among the individual trials. Four studies used nitroglycerin in the control group,21,24–26 one used 0.9% sodium chloride, 27 one used nitroprusside, 28 and one used dobutamine. 23 The drugs used in the control group were not indicated in the other two studies.20,22 Because nitroglycerin is also a standard drug for the treatment of heart failure, we further compared the risk of mortality between patients who received nesiritide or nitroglycerin. We found no difference in the risk of mortality after treatment with nesiritide or nitroglycerin, which was consistent with the results of a previous study. 19 Thus, in patients with AMI and heart failure, treatment with nesiritide did not increase the risk of mortality compared with the effects of control treatments. Three trials provided information regarding readmission, and all readmissions were attributable to heart failure.24,25,28 No difference was observed in the risk of readmission between the nesiritide and control groups in our analysis, which was similar to the conclusion of one previous study 35 but differed from those of other studies.15–17 Hypotension is the most common adverse reaction of rhBNP therapy. 35 However, our results indicated that treatment with nesiritide resulted in a non-significantly lower risk of hypotension. In addition, this finding was different from the conclusion of another study. 13 Different patient populations and methods were reported for each study, and the different risks of bias may have led to different conclusions.
Four studies provided information regarding MACE. In the study by Gong et al. 20 MACE consisted of a composite of cardiac death, recurrent nonfatal myocardial infarction, and acute left ventricular failure. In the study by Zhang et al. 27 MACE included reinfarction, repeat heart failure, malignant arrhythmia (ventricular tachycardia, ventricular fibrillation, and cardiac arrest), and cardiogenic death. Detailed descriptions were not available in the other two studies.21,24 No difference was found in the risk of MACE between the nesiritide and control groups in our analysis; however, given the different definitions of MACE in four of the studies, we analyzed each specific cardiovascular adverse reaction individually and found no differences between the two treatment groups. SBP, DBP, serum sodium, serum potassium, SCr, and Cys-C levels, and eGFR were measured to evaluate the effects of nesiritide on renal function. Similar to the results of a previous study,35,36 nesiritide did not affect renal function. Two included studies reported information about dialysis,25,27 but no patients required dialysis in either trial. Elevated SCr was a common adverse reaction after nesiritide treatment; however, our analysis found no differences between the two groups, which was similar to the results of the study by Xiong et al. 37 Nausea, headache, abdominal pain, and dyspnea are the most common non-cardiovascular adverse reactions during nesiritide treatment. However, in our study, only one patient receiving nesiritide reported a tolerable headache, and it was uncertain whether this was related to the drug. 23 The other three types of non-cardiovascular adverse reactions were not reported in any trial. The HR, BP, and MACE results indicated that nesiritide did not increase myocardial oxygen consumption or the risk of arrhythmia in patients with AMI and heart failure, which was an improvement compared with the outcomes of dobutamine treatment.4,5
Limitations in current study evidence
First, unpublished papers were not included in this meta-analysis, which may have induced publication bias and a smaller sample size. Therefore, larger
Conclusion
Nesiritide treatment can significantly increase cardiac output and urine volume in patients with AMI and heart failure without increasing myocardial oxygen consumption or the risk of mortality. Furthermore, the improvements of heart failure indicators were superior to those induced by other drugs, with no significant differences in the rates of adverse reactions between the nesiritide and control groups. In short, nesiritide can improve global cardiac function and subsequently enhance systemic function in patients with AMI and heart failure, and it appears to be a safe treatment for these patients.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethical approval
This study was a meta-analysis of published literatures, and it does not contain data from studies with human participants or animals performed by the authors; thus, a statement from the Ethics Committee was unnecessary.
Funding
This study was supported by the National Natural Science Foundation of China (Grant No. 51573211).