
Abstract
Purpose of Study:
Diabetes mellitus accelerates the development of atherosclerosis. Patients with diabetes mellitus have higher incidence and mortality rates from cardiovascular disease and undergo a disproportionately higher number of coronary interventions compared to the general population. Proper selection of treatment modalities is thus paramount. Treatment strategies include medical management and interventional approaches including coronary artery bypass graft (CABG) surgery and percutaneous coronary interventions (PCI). The purpose of this review is to assimilate emerging evidence comparing CABG to PCI in patients with diabetes and present an outlook on the latest advances in percutaneous interventions, in addition to the optimal medical therapies in patients with diabetes.
Key Methods:
A systematic search of PubMed, Web of Science and EMBASE was performed to identify prospective, randomized trials comparing outcomes of CABG and PCI, and also PCI with different generations of stents used in patients with diabetes. Additional review of bibliography of selected studies was also performed.
Main Conclusions:
Most of the trials discussed above demonstrate a survival advantage of CABG over PCI in patients with diabetes. However, recent advances in PCI technology are starting to challenge this narrative. Superior stent designs, use of specific drug-eluting stents, image-guided stent deployment, and the use of contemporary antiplatelet and lipid-lowering therapies are continuing to improve the PCI outcomes. Prospective data for such emerging interventional technologies in diabetes is however lacking currently and is the need of the hour.
Introduction
Diabetes mellitus and prediabetes affected 10% and 34% of the United States population in 2015 respectively and is the seventh leading cause of death in the US. 1 Diabetes is strongly associated with greater atherosclerotic burden, quicker coronary disease progression, and worse coronary outcomes with or without treatment. 2
Management of stable CAD in diabetes involves medical management of risk factors and in certain cases, utilization of interventional strategies. Interventional approaches include percutaneous coronary intervention (PCI) and coronary artery bypass grafting (CABG), with CABG historically having superior outcomes. Current evidence and guidelines lag behind rapid evolution in PCI technology and evaluating these new systems is bound to change future treatment paradigms. The aim of this review is to (a) enlist important clinical trials comparing CABG to PCI and comparing different stent types in diabetes, (b) discuss the strengths and weaknesses of the different coronary interventions, and (c) outline the latest technological advances paving the way for improved interventional outcomes.
Section I. Accelerated coronary artery disease in diabetes mellitus
The pathophysiologic milieu in diabetes accords a high risk of atherosclerosis 3 and leads to complex coronary lesions with multi-segment, multivessel involvement. 4 Atherosclerotic plaques in diabetes have a greater predilection for ulceration. 5 Left anterior descending (LAD) artery is more severely affected and collateral vessel network is poorly developed 6 - anatomical variants at greater risk of poorer outcomes.
Hyperglycemia leads to the formation of advanced glycosylation end products (AGEs), 7 which modify cell surface proteins and lipids, causing signaling abnormalities, excessive oxidative stress, and reduce vessel wall compliance. Diabetes promotes protein kinase C (PKC) activation and di-acyl glycerol (DAG) production. PKC/DAG accelerates atherosclerosis by promoting inflammation and smooth muscle cell recruitment. 8 PKC activation also decreases endothelial nitric oxide (NO) production by inhibition of endothelial NO synthase (eNOS) and increases endothelin production, thus inhibiting vasodilation and increasing oxidative stresses. 9
Diabetes mellitus promotes vascular inflammation by enhancing the expression of pro-inflammatory genes like nuclear factor-kB (NF-kB), which drives leukocyte and smooth muscle recruitment and increases macrophage lipid uptake. Diabetes accelerates vascular remodeling by activating matrix metalloproteinases (MMP-1 and 2), leading to vulnerable plaque physiology and heightens the risk of thrombosis and rupture.
Diabetes coexists with obesity and hypertension as part of the metabolic syndrome, both of which increase the risk of CAD. Lipid metabolism is altered in diabetes. 10 Hypertriglyceridemia is the most common dyslipidemia associated with diabetes and exerts atherogenic effects indirectly through the metabolism of triglyceride-rich lipoprotein (TGRL). Smaller low-density lipoprotein cholesterol (LDL-C) particles in diabetes are more readily oxidized, which amplifies their atherosclerotic potential by permitting easier vessel wall uptake. 11 Protective lipid components like high-density lipoprotein cholesterol (HDL-C) and apolipoprotein A1 have diminished levels in diabetes. 12
Diabetes mellitus enhances platelet activity13,14 (Figure 1 for the conceptual framework). Hyperglycemia promotes the expression of thromboxane (TxA2), p-Glycoprotein, and von-Willebrand Factor (vWF) - activators of platelet adhesion and activity.15,16 Diabetes impairs platelet responsiveness to NO and prostaglandin I2 (PGI2) 17 -agents suppressing platelet activation. Diabetes modifies platelet receptor profile, decreasing anti-platelet drug effectiveness.
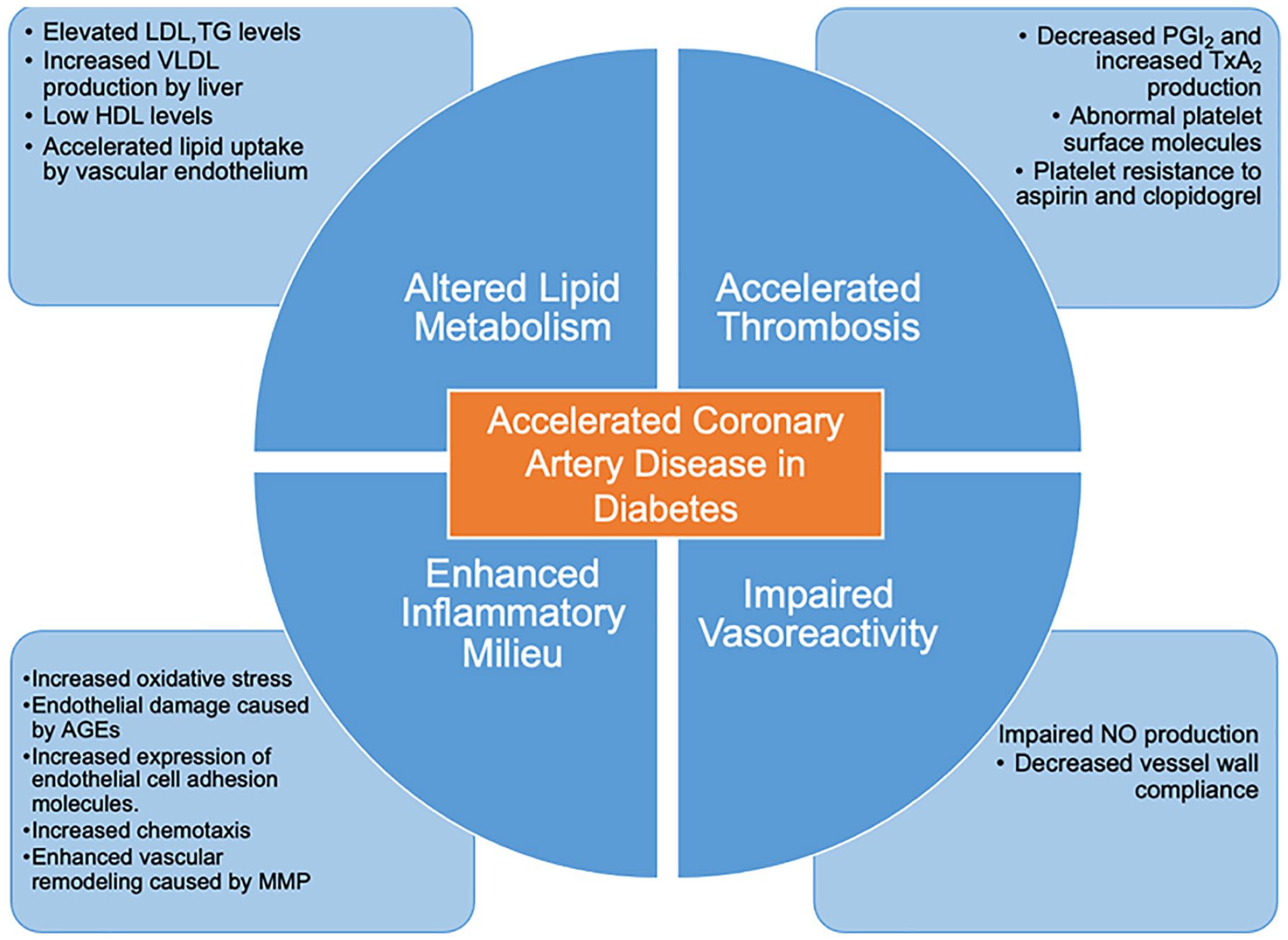
Risk factors for coronary artery disease in diabetes. Progression of coronary artery disease is hastened in diabetes due to rapid atherosclerosis, impaired vessel wall reactivity, elevated circulating lipid levels, and thrombogenic platelet profile.
Intravascular imaging and histopathology have demonstrated decreased thickness of fibrous cap, higher lipid, calcium, and inflammatory burden in atherosclerotic plaques in patients with diabetes, 18 histological variants that portend a higher risk of adverse event occurrence in these plaques. 19
Section II: Treatment approaches in stable coronary artery disease in diabetes mellitus
Optimal medical therapy (OMT) is the cornerstone of stable CAD management. Guideline based medical therapeutics have demonstrated similar outcomes compared to interventional strategies in many large scale trials including COURAGE, 20 and ISCHEMIA 21 trials. OMT is also the initial therapy for CAD in diabetes. BARI-2D 22 and sub-analysis of the COURAGE trial showed no significant benefit of adding interventions over OMT (except for decrease in cardiovascular events in the CABG + OMT cohort in BARI-2D). Current anti-diabetic armamentarium includes sodium-glucose transporter-2 (SGLT-2) inhibitors and glucagon-like peptide (GLP)-1 agonists, which provide significant improvement in combined cardiovascular outcomes in patients with diabetes.23–25
Anti-platelet therapy is another core component of CAD management and efficacy of antiplatelet agents in diabetes differ compared to patients without diabetes, necessitating careful selection of drugs. Optimal management of hyperlipidemia and hypertension is essential in decreasing the risk of cardiovascular events in diabetes mellitus, especially post PCI. 26
Procedural interventions for the treatment of CAD in diabetes is only recommended in particular situations (Table 1). A comprehensive assessment of coronary disease in diabetes using non-invasive testing is required to define risk and support interventional decision making. This can occur in the form of either dynamic (radionuclide, electrocardiography, echocardiography-based stress testing) or anatomic assessment (coronary computed tomography angiography [CCTA]). 27 Appropriate selection of patients and procedures is dependent on testing results and targeted outcomes. Our review will be focused on discussing aspects of interventional management in diabetes mellitus that can be utilized after proper clinical assessment.

Optimal medical therapy is the initial line of management of stable CAD in diabetes and includes anti-diabetic drugs like SGLT-2 inhibitors/GLP-1 analogs, statins, anti-hypertensives, and antiplatelet agents.
CABG: coronary artery bypass graft; CAD: coronary artery disease; GLP: glucagon-like peptide; PCI: percutaneous coronary interventions; SGLT: sodium-glucose co-transporter.
Conventional approaches of revascularization
Patients with diabetes mellitus comprise one-third of all performed percutaneous interventions. 31 Rates of incomplete revascularizations and complications from these procedures are much higher in patients with diabetes compared to the general population.32,33 There are two main interventional approaches for the treatment of CAD and their outcomes have varied over the years, largely depending on varying clinical factors and technological advances (Figure 2).
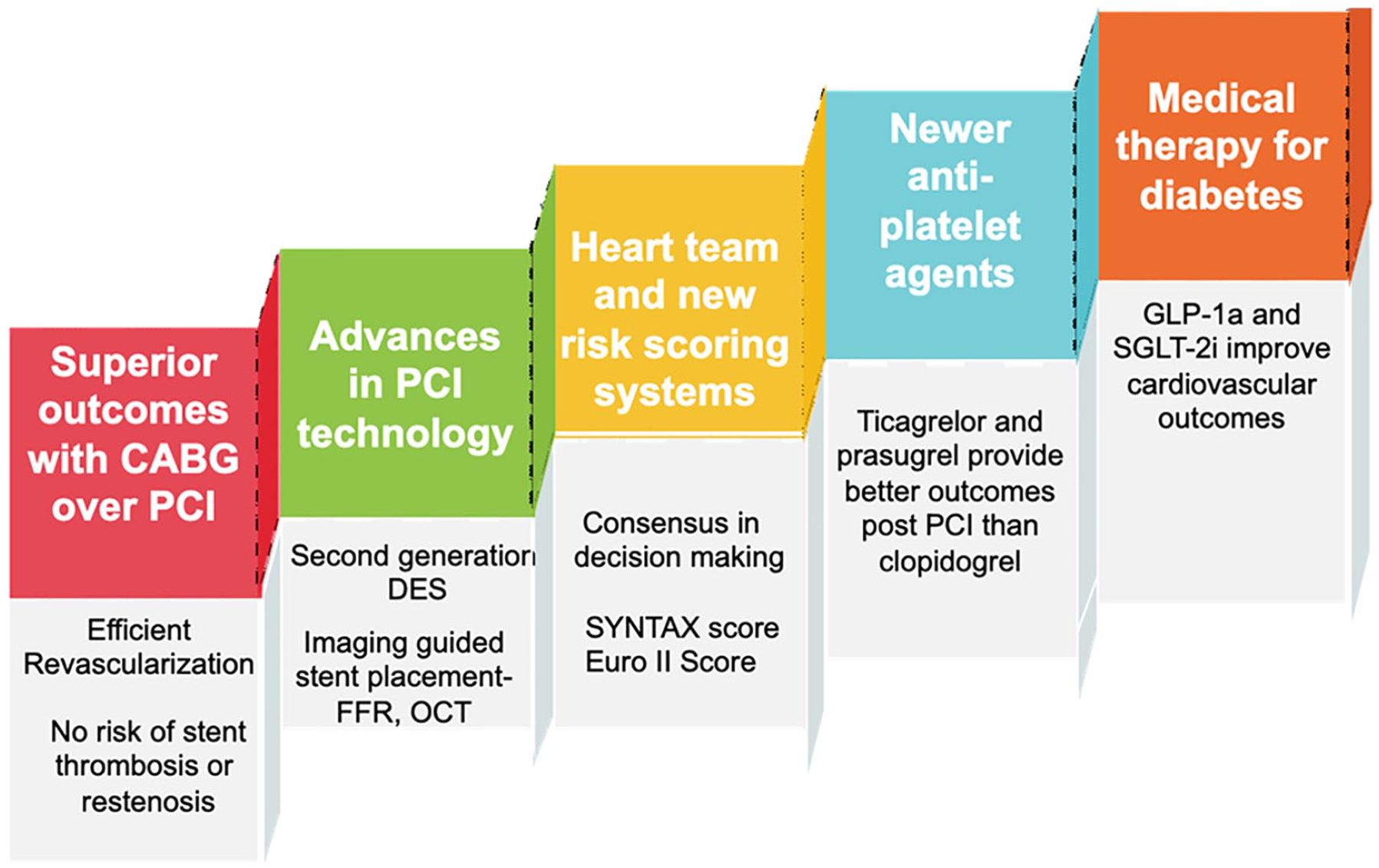
Major determinants of clinical outcomes after coronary artery interventions in diabetics. CABG is superior to PCI in diabetics, as per current evidence. However, rapid advances in PCI technology and drugs have improved outcomes of coronary stenting. The current best practices in decision making involve a “Heart Team,” comprising of cardiologists and cardiothoracic surgeons.
Coronary artery bypass grafting (CABG) involves the surgical transposition of autologous arteries/veins to bypass coronary artery blockages, providing coronary flow to the downstream myocardium.
Percutaneous coronary intervention (PCI) is the minimally invasive approach, which uses ballooning/stenting to open occluded coronary lesions. Early percutaneous interventions consisted of balloon dilation angioplasty. PCI currently involves stenting of the culprit lesions, which prevents vessel recoil and promises long term patency.
Comparative evidence of PCI and CABG diabetes
Early comparisons assessed CABG and PCI with balloon angioplasty. The diabetic cohort in CABRI trial (1994) (n = 125) had a statistically non-significant higher all-cause mortality rate in patients undergoing angioplasty. 34 The diabetic sub-group in BARI trial (1996) demonstrated significantly better 5-year survival rates in CABG (80.3%) group compared to the balloon angioplasty group (60.5%) (p = 0.003) and continued benefit of CABG even after 7 years. 35
Tables 2 to 4 summarize important trials comparing outcomes of CABG and PCI with BMS/1st/2nd generation drug-eluting stents (DES) and outcomes of BMS/1st generation compared to second generation DES, in patients with diabetes. Many of these studies are a subgroup analysis of the diabetic cohort of the main study population- thus decreasing their power.
Major trials comparing PCI using BMS and 1st generation DES to CABG.

In many of the trials, data was obtained from sub-group analysis and thus lacked power.
CABG: coronary artery bypass graft; CI: confidence interval; DES: drug-eluting stent; HR: hazard ratio, MACCE: major adverse cardiovascular and cerebrovascular events; MI: myocardial infarction; PCI: percutaneous coronary intervention; PES: paclitaxel-eluting stent; SES: sirolimus-eluting stents.
Efficacy of PCI with second generation DES compared to first generation DES in diabetics.

Most of the trials have results generated from a subgroup analysis, thus being only hypothesis-generating.
EES: everolimus-eluting stent; PCI: percutaneous coronary intervention; MACE: major adverse cardiovascular event; PES: paclitaxel eluting stent; RR: relative risk; SES: sirolimus-eluting stent; TVF: target vessel failure; TVR: target vessel revascularization; ZES: zotarolimus-eluting stent.
Efficacy of second generation DES in diabetics compared to CABG.

CABG: coronary artery bypass graft; EES: everolimus-eluting stent; LMCAD: left main coronary artery disease; PCI: percutaneous coronary intervention; MACCE: major adverse cardiovascular and cerebrovascular events; RR: relative risk.
Section III. CABG now and PCI for the future?
Superior cardiovascular outcomes of CABG over PCI in diabetes are primarily powered by higher rates of complete revascularization and preservation of natural endothelial responses in CABG, in comparison to maladaptive endothelial pathophysiology in a stented vessel. 50 This advantage is important in diabetes due to the severity of atherosclerosis noted in diabetes.
CABG introduces an “endogenous stent,” which bypasses multiple stenosed areas, leading to more complete revascularization and greater protection against future thrombosis, compared to stents, which revascularize single lesions. Autologous vessels are less immunogenic and thrombogenic than stents and provide a more physiologic milieu. Saphenous venous grafts (SVG) were initially used and are being increasingly replaced by arterial conduits due to higher rates of long-term venous graft failure from vessel remodeling.51,52 Data from Coronary Artery Surgery Study (CASS) and other large-scale trials have demonstrated better long-term patency of arterial over venous grafts.53–55 Internal mammary arterial (IMA) grafts, in particular, have preserved endothelial functions like vasodilation and have higher flow reserve (due to higher compliance). 56 Noncompliance with anti-platelet therapy is not lethal in CABG, as it can be in PCI.
Restenosis and thrombosis are the primary pathogenic mechanisms involved in poorer outcomes in PCI treated vessels and these are intensified in diabetes. Restenosis involves narrowing of the stented sites due to fibro-inflammatory deposition, starting as an initial thrombogenic reaction, followed by migration of inflammatory cells and finally intimal hyperplasia and remodeling. 57 Stents are foreign bodies and thus more thrombogenic, which translate into increased risk of early (<1-month) or late (1-month–1-year) in-stent thrombosis. 58 Delayed healing and impaired endothelialization of the stented area play a role in this process. 59 Multivessel disease, requiring multiple stents, amplifies these risks.
Intervention rates are, however, disproportionately skewed toward the use of PCI,60,61 despite the evidence-based superiority of CABG. Minimal invasiveness and shorter post-procedural stay times make PCI a very attractive approach for patients. CABG entails a greater risk of early post-procedural stays and events including deep tissue infection due to open sternotomy and higher stroke risk due to use of cardiopulmonary bypass. 62 The “test and treat” approach involving diagnostic catheterization getting converted into a PCI procedure might be another possible reason for increasing PCI utilization. Physician biases can affect disclosures, especially when the diagnostic and therapeutic options are intertwined. 63 The benefits of new PCI technologies are occasionally applied by conjecture, as rapidly changing advances result in the sparsity of prospective data.
Case-based therapeutic adjudication
Risk factor-based individualized assessment is essential to stratify patients for the best interventional approach. A “Heart Team” comprising primarily of cardiologists and cardiothoracic surgeons, helps achieve a multi-disciplinary consensus and is seen to improve outcomes. 64 Scoring systems such as EUROscore and SYNTAX also guide decision making. EuroSCORE I & II predict mortality post-cardiac surgery.65–67 These scores are however not well validated in the diabetic population. SYNTAX score 68 estimates CAD severity and complexity. Higher SYNTAX scores are associated with a greater benefit of CABG over PCI. Post-hoc analysis of SYNTAX scores of treated diabetic patients in the FREEDOM trial noted the correlation of SYNTAX scores with PCI outcomes but showed no benefit of SYNTAX score calculation in changing recommendations from CABG to PCI. 69 Many of the trials discussed in Tables 2 to 4 exclude high-risk surgical patients, patients with complex lesions, recent MI, heart failure, and prior revascularization, thereby creating an inclusion bias.
Left ventricular systolic dysfunction (LVSD), a major complication of CAD, is considered to be a risk factor for a major surgery like CABG. However, evidence from the STICH trial showed that the addition of CABG to medical therapy helped in a significant reduction of cardiovascular hospitalizations and cardiovascular mortality over medical therapy alone in patients with LVSD. 70 A 12-year follow-up retrospective study demonstrated significant improvement in MACCE and overall mortality with CABG over PCI in diabetic patients with LVSD (ejection fraction <35%). 71 Further prospective studies are needed to clear the air regarding the use of CABG in this population, who have a higher surgical risk, but might benefit more with the bypass option in the long run.
Left main coronary artery disease (LMCAD) in CAD portends a high risk of future complications and poorer outcomes and has typically been treated with CABG in the diabetes population. Comparative evidence in cases of isolated left main coronary artery disease (LMCAD) in diabetes has also been updated, with data from MAIN-COMPARE and EXCEL showing similar cardiovascular outcomes with PCI compared to CABG in diabetes.72,73
Chronic total occlusions (CTO), defined as chronic (>3 months) complete coronary occlusion (TIMI 0 flow), are more common in diabetes. 74 CTOs are mostly treated by anginal medical therapy and CABG. CTO PCI is considered high risk and is performed in centers with high volume and expertise. Single vessel CTO and patients with previous CABG are probable candidates for CTO PCI.
Another clinical situation for preferential PCI utilization in diabetes is post CABG worsening of CAD. Repeat surgery in such cases confers a high mortality risk and PCI is a decent option. 75
Recent advances in PCI and CABG technology
The advances in interventional cardiology are progressing at a breakneck speed. Major progress has been made in developing new-generation DES, which have thinner construction, bio-similar designs, and better and longer drug effect and delivery. Bioresorbable DES/scaffolds (BR-DES/BRS) are advanced generation stents with a bioresorbable design and a theoretically lower risk of thrombosis. However, early BRS stents demonstrated a higher incidence of very late thrombosis in BRS group,76,77 which led to their withdrawal from the market. Outcomes of newer BRS/BD-DES look promising, with long term data awaited.78,79
Imaging strategies including fractional flow reserve (FFR), optical coherence tomography (OCT), and instantaneous wave-free ratio (iFR) are used to re-stratify intermediate lesion severity in angiographic studies, which leads to a significant change in the treatment plan. However, the benefit in diabetes has not been proven. 80
Improved PCI outcomes with proper stent selection, placement location, and technique. Intravenous ultrasound (IVUS) and optical coherence tomography (OCT) guided stent placement techniques are being utilized in defining coronary lesion characteristics and severity. These intracoronary imaging techniques guide in appropriate stent selection, length, placement site, and technique to refine outcomes.81,82 IVUS and OCT also help in defining post-stenting expansion and possible mal-apposition and dissection, thus helping in post stenting risk minimization. 83 Targeted interventions in plaques with high risk characteristics diagnosed with OCT/IVUS allows selective PCI utilization in the most severe areas and narrows the therapeutic difference between PCI and CABG in patients with diabetes. 84
Aspirin and clopidogrel have sub-optimal activity in diabetics, due to modified platelet membranes, altered eicosanoid, and anti-platelet metabolism.85–87 Newer agents like prasugrel and ticagrelor have demonstrated better cardio and cerebrovascular event rates in PCI treated patients in diabetes compared to the old agents- a result of faster action, more effective platelet inhibition, additional endothelial benefit, and no first-pass requirement for these agents.88,89
SGLT-2i/GLP-1a also improve cardiovascular endpoints (discussed above) and should be used as first-line agents in diabetes with a history of or high risk of CAD. Patients with diabetes have a high residual coronary risk even after maximal therapy with statins. Treatment with ezetimibe and Proprotein convertase subtilisin/kexin type 9 (PCSK-9) inhibitors reduce the added lipidomic risk by further reduction of LDL-C levels.90–92 Omega 3 fatty acids are another tool in the CAD treatment armamentarium, eicosapentaenoic acid demonstrating a significant reduction in adverse cardiovascular outcomes in the large prospective REDUCE-IT trial. 93
In CABG, revascularization using bilateral IMA has shown mixed results in the general population with a mortality benefit in large observational studies and meta-analysis94,95 countered by results of the large ART trial (2019), which demonstrated no significant 10-year mortality benefit. 96 Off-pump CABG and minimally invasive CABG have not had a significant impact on outcomes with CABG.
Hybrid coronary revascularization (HCR)97,98 attempts to utilize left IMA for LAD bypass (providing maximal survival advantage) coupled with non-LAD small vessel PCI. This approach is particularly helpful when bypasses of particular vessels or an advanced thoracic approach is prohibitive or if second arterial conduits are not available. Current data points toward similar outcomes to traditional CABG.97,99 This option is not common practice and the lack of large prospective analysis limits widespread use.
Section IV. Conclusion
Coronary artery disease and diabetes mellitus are both modern era epidemics and have a closely dependent relationship. Typical approaches and outcomes of CAD therapies in the general population cannot be extrapolated to diabetics due to a significantly increased risk of CAD in the latter. Current evidence points to a very strong benefit of CABG over PCI in this patient population, both in terms of repeat events and mortality. With current advances in technologies in the domain of PCI and the latest anti-diabetes and anti-platelet drugs, we do anticipate improved outcomes in the future with minimally invasive techniques. Risk stratification and an open discussion with the patient about the risks and benefits of each procedure is essential. The role of the primary physician is vital for secondary prevention and maintaining compliance, which is important for thrombosis prevention. There have been tremendous advances in PCI technology. Nonetheless, on the evidence-based front, the superiority of CABG stands as of now.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under award number UL1TR001412 to the University at Buffalo. Dr. Sharma also received support from the NHLBI K08HL131987.