
Abstract
Background:
Stress hyperglycemia is a common finding during ST elevation myocardial infarction in diabetic patients and is associated with a worse outcome. However, there are limited data about stress hyperglycemia in non-diabetic patients and its outcome especially in patients undergoing primary percutaneous coronary intervention.
Methods:
The study was conducted on 660 patients with ST elevation myocardial infarction who were managed with primary percutaneous coronary intervention. Patients were classified into two groups according to the presence of stress hyperglycemia: group I (patients with stress hyperglycemia) and group II (patients without stress hyperglycemia). Patients were analysed for clinical outcome including mortality and the occurrence of major adverse cardiac events.
Results:
Incidence of stress hyperglycemia was 16.8%, multivariate regression analysis identified the independent predictors of stress hyperglycemia, that were family history of diabetes mellitus odds ratio 1.697 (95% confidence interval: 1.077–2.674, p = 0.023), body mass index >24 kg/m2 odds ratio 1.906 (95% confidence interval: 1.244–2.922, p = 0.003) and cardiogenic shock on admission odds ratio 2.517 (95% confidence interval: 1.162–5.451, p = 0.019). Mortality, cardiogenic shock, contrast induced nephropathy and no reflow phenomenon were significantly higher in stress hyperglycemia group with p value = 0.027, 0.001, 0.020 and 0.037, respectively.
Conclusion:
Stress hyperglycemia in non-diabetic patients with ST elevation myocardial infarction undergoing primary percutaneous coronary intervention is associated with increased incidence of no reflow phenomenon, contrast induced nephropathy, cardiogenic shock and higher mortality.
Keywords
Introduction
Stress hyperglycemia has been defined as hyperglycemia that occurring in critically ill patients, who have not been previously diagnosed to have diabetes mellitus (DM). Stress hyperglycemia is temporarily increasing in plasma glucose levels during critical illness. 1 The American Diabetes Association (ADA) guidelines described stress hyperglycemia as having a random glucose level greater than 140 mg/dL at any given time in hospitalized patients. 2 Stress hyperglycemia is a common condition, and has been described to occur in up to 30%–80% of many hospital units. 3 An elevated plasma glucose level on admission is a predictor of in-hospital and long-term adverse outcomes in patients with ST elevation myocardial infarction (STEMI), irrespective of diabetic status. 4
Hyperglycemia seen at the onset of STEMI seems to be associated with the stress mechanism, which is attributed to high free fatty acids, insulin resistance and steroid hormones. 5 Stress hyperglycemia creates a new glucose balance allowing a higher blood glucose diffusion gradient, which maximizes cellular glucose uptake in the face of mal-distributed micro-vascular flow. 6 In fact, this mechanism becomes injurious to the mitochondria, renders oxidative stress–related damage to the cells and disturbs the course of the disease in the worst manner.7,8
Stress hyperglycemia is a frequent complication in the setting of STEMI and affects patients with and without established DM, and associated with adverse outcomes in diabetic patients. However, the effect of stress hyperglycemia on non-diabetic patients is still controversy. So, the objective of the present study was to investigate the incidence, predictors and outcomes of stress hyperglycemia in non-diabetic patients with STEMI, who were treated with primary percutaneous coronary intervention (PPCI) in order to assess the effects of stress hyperglycemia on morbidity and mortality of those patients.
Patients and methods
Study population
This study was conducted on 660 patients with STEMI who were admitted to cardiovascular department for PPCI during the period from 1st of January 2017 to 31st of December 2018 with follow-up period for 3 months. The study was approved by the Local Research Ethics Committee of the Faculty of Medicine, Tanta University, and was in accordance with the principles of the Declaration of Helsinki II. All patients included in the study signed a written consent and a code number was given for every patient pointed to his name, address and telephone number. The diagnosis of STEMI was established if persistent chest discomfort or pain >20 min concurrently to the presence of ST segment elevation on two adjacent leads, or a presumably new left bundle branch block on electrocardiogram (ECG).
Exclusion criteria
We excluded patients known to have DM at the time of admission. Patients presented with high HbA1c were excluded from the study. Moreover, patients with new onset DM, their blood glucose levels still rising after the period of stress were also excluded from the study. Stable patients with STEMI with late presentation after 24 h of chest pain onset were excluded from the study. We excluded also patients with severe hepatic or renal impairment, concomitant neoplastic diseases, mental or intellectual impairment and those who were taking glucocorticoid therapy at the time of admission.
Demographic, clinical and laboratory data
All patients were subjected to detailed history taking about atherosclerosis risk factors, for example, hypertension, dyslipidemia and smoking. Family history of DM was taken. History of comorbidities, for example, chronic kidney disease and previous myocardial infarction. Previous medications history was interrogated. Full physical examination of the patients and resting standard 12-lead ECG was done for all patients. Venous blood samples were collected under sterile conditions and used for laboratory investigations including random blood glucose level, HbA1c%, lipid profile, serum creatinine level before and after the procedure and creatine kinase myocardial band (CK-MB). Stress hyperglycemia was defined as plasma glucose levels greater than 140 mg/dL at any given time in hospitalized patients who were not known to have DM. 2
Coronary angiography
Coronary angiography was done by either radial or femoral approach. After identification of the anatomy, culprit vessel, thrombus burden and thrombolysis in myocardial infarction (TIMI) flow, revascularization of the culprit vessel was done, aspiration catheter and glycoprotein IIb/IIIa inhibitors were used according to operator judgement. Volume of contrast agent was measured and post-procedural TIMI flow was assessed. Echocardiographic examination was done after the procedure with Vivid E9 dimension (General Electric Medical Systems, Horten, Norway) with assessment of left ventricular ejection fraction by Simpson method.
Endpoints
The primary end point of this study was the occurrence of stress hyperglycemia and patients were classified into two groups according to it: group I (patients with stress hyperglycemia) and group II (patients without stress hyperglycemia). The secondary endpoint was the clinical outcome including mortality or the occurrence of major adverse cardiac events (MACEs) in the form of heart failure, cardiogenic shock, cardiac arrest, contrast induced nephropathy which was defined as an increase in serum creatinine >25% from baseline in the first 72 h, re-infarction and the occurrence of major bleeding.
Statistical analysis
Statistical analysis was done using SPSS 23 (IBM, Armonk, NY, United States). Quantitative variables were expressed as mean ± standard deviation (SD). Categorical variables were expressed as absolute values and proportions. Student’s t-test was used to test significance between two groups in quantitative data. Chi-square (χ2) test of significance was used in order to compare proportions between two qualitative parameters. p value <0.05 was considered statistically significant. Multivariate regression analysis using binary logistic regression was performed to detect the independent predictors of stress hyperglycemia and factors affecting mortality.
Results
Demographic and clinical data of the studied groups
The present study included 660 patients with STEMI admitted to our cardiovascular department and subjected to PPCI. Patients were divided into two groups: group I (111 patients with stress hyperglycemia) and group II (549 patients without stress hyperglycemia). Patients with stress hyperglycemia were older in age, the incidence of hypertension, dyslipidemia and chronic kidney disease was higher in this group than group II. There was statistically significant difference between both groups regarding family history of DM, body mass index and cardiogenic shock on admission with p value = 0.019, 0.001 and 0.018, respectively, with more prevalence in group I. According to laboratory results, random blood sugar and serum creatinine levels post-procedural were significantly higher in group I (p value = 0.001 and 0.012, respectively). Mortality was higher in group I with p value = 0.027. Cardiogenic shock and contrast induced nephropathy were more predominant in group I with p value = 0.001 and 0.020, respectively, with no other statistically significant difference between both groups regarding other demographic, basal clinical characteristics, laboratory results and clinical outcome as shown in Table 1.
Demographic, clinical characteristics, laboratory results and outcome of all patients in the two groups.
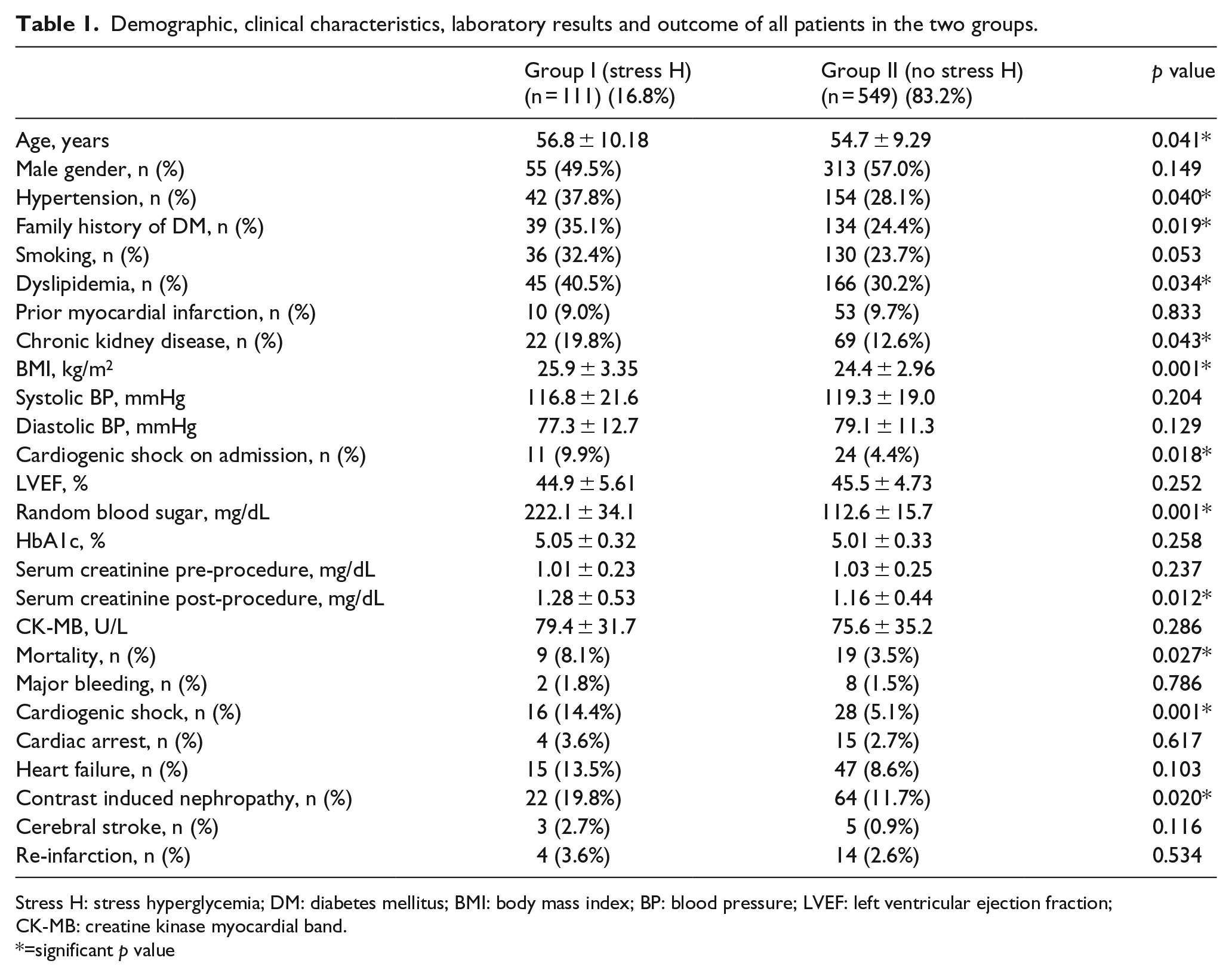
Stress H: stress hyperglycemia; DM: diabetes mellitus; BMI: body mass index; BP: blood pressure; LVEF: left ventricular ejection fraction; CK-MB: creatine kinase myocardial band.
=significant p value
Angiographic results of the studied groups
With respect to angiographic results, there was no statistically significant difference between both groups regarding the culprit vessel, thrombus burden or volume of contrast agent used during the procedure. However, there was statistically significant difference regarding the incidence of no reflow phenomenon (TIMI flow = 0, 1 and 2) that was higher in group I with p value = 0.037. Post-procedural TIMI 3 flow was lower in stress hyperglycemia group [77 (69.4%) vs 445 (81.1%)]. Moreover, there was statistically significant difference between both groups regarding the need for aspiration catheters, which was more in group I in addition to glycoprotein IIb/IIIa inhibitors with p value = 0.042 and 0.011, respectively, as shown in Table 2.
Angiographic results of all patients in the two groups.
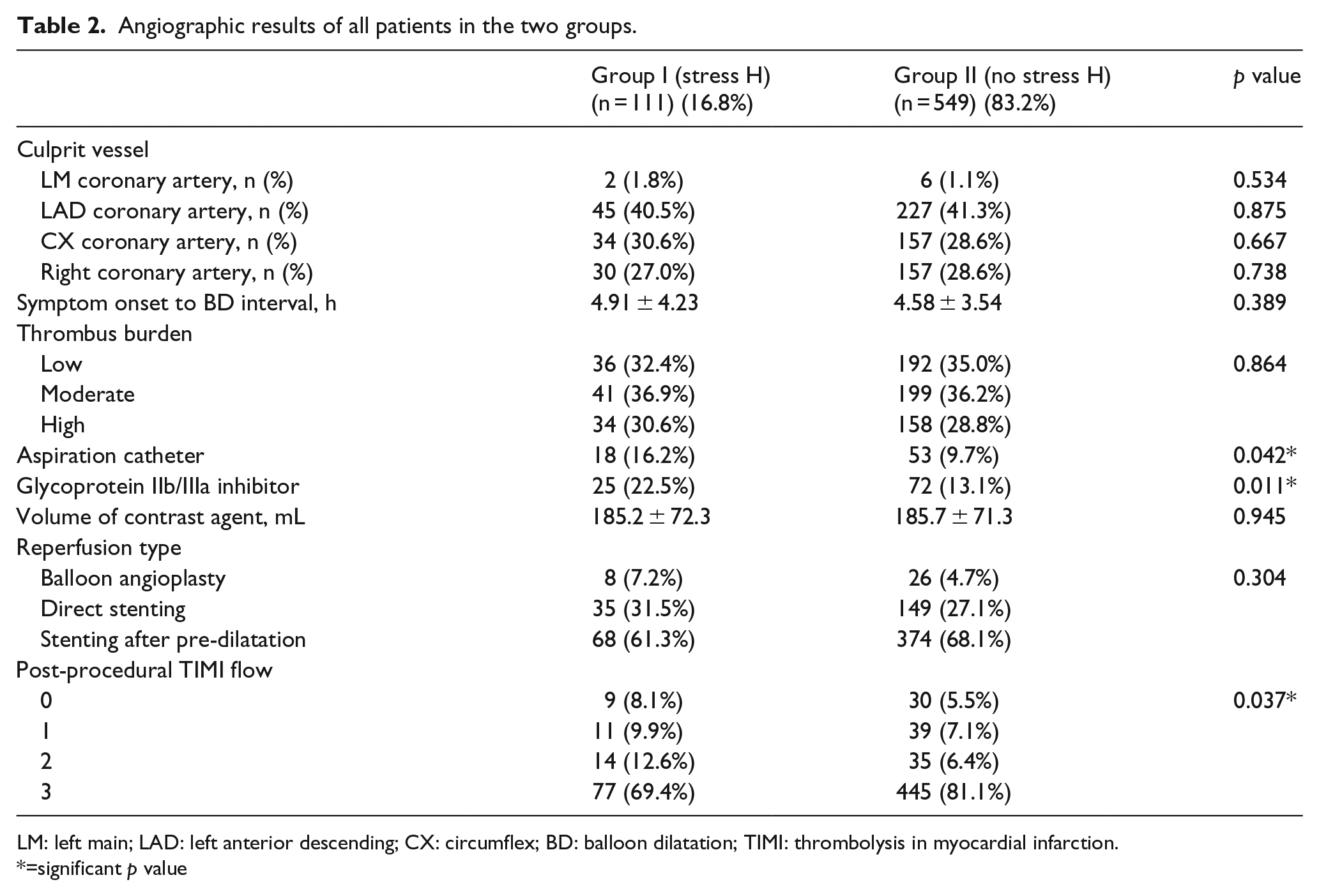
LM: left main; LAD: left anterior descending; CX: circumflex; BD: balloon dilatation; TIMI: thrombolysis in myocardial infarction.
=significant p value
Multivariate regression analysis
Multivariate regression analysis was performed to identify the independent predictors of stress hyperglycemia and the following results: family history of DM odds ratio (OR) 1.697 [95% confidence interval (CI95%): 1.077–2.674, p = 0.023], body mass index >24 kg/m2 OR 1.906 (CI95%: 1.244–2.922, p = 0.003) and cardiogenic shock on admission OR 2.517 (CI95%: 1.162–5.451, p = 0.019) were the independent predictors of stress hyperglycemia as shown in Table 3 and Figure 1.
Multivariate regression analysis for independent predictors of stress hyperglycemia.
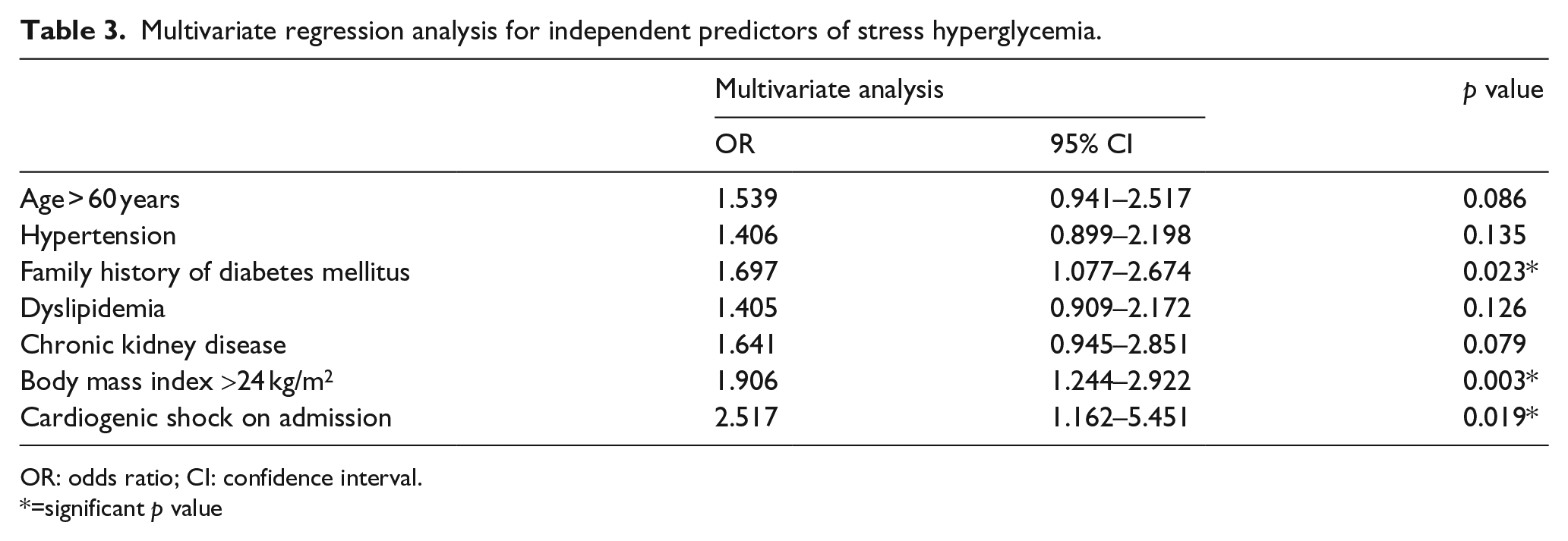
OR: odds ratio; CI: confidence interval.
=significant p value
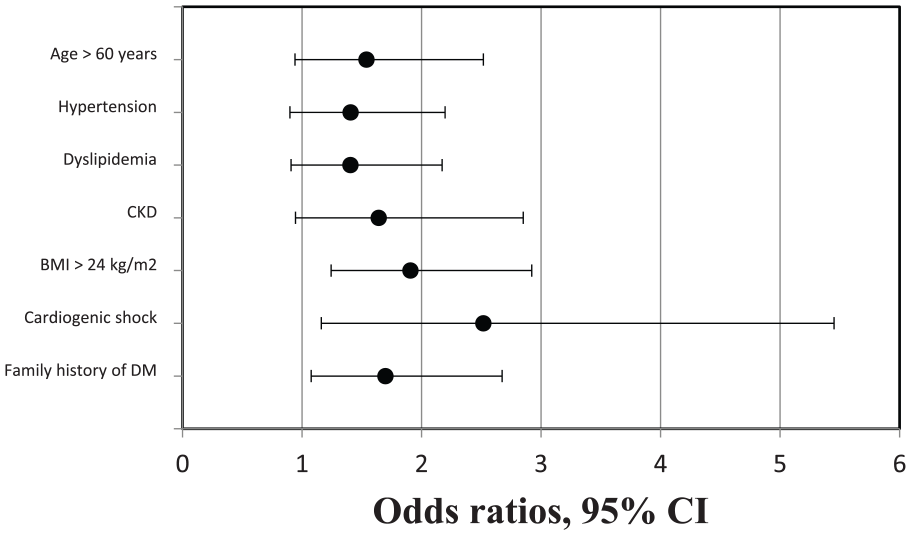
Forest plot of the multivariate regression analysis showing odds ratios, 95%CI of the independent predictors of stress hyperglycemia that were family history of diabetes mellitus, cardiogenic shock on admission and body mass index >24 kg/m2.
Multivariate regression analysis was also performed to identify factors predicting mortality as presented in Table 4 with the following results: heart failure OR 3.832 (CI95%: 1.568–9.367, p = 0.003) and contrast induced nephropathy OR 4.045 (CI95%: 1.708–9.578, p = 0.001) were the independent predictors of mortality. Kaplan Meir curve for comparing outcomes in the two groups was performed and showed better survival function in patients without stress hyperglycemia as shown in Figure 2.
Multivariate regression analysis for factors predicting mortality.
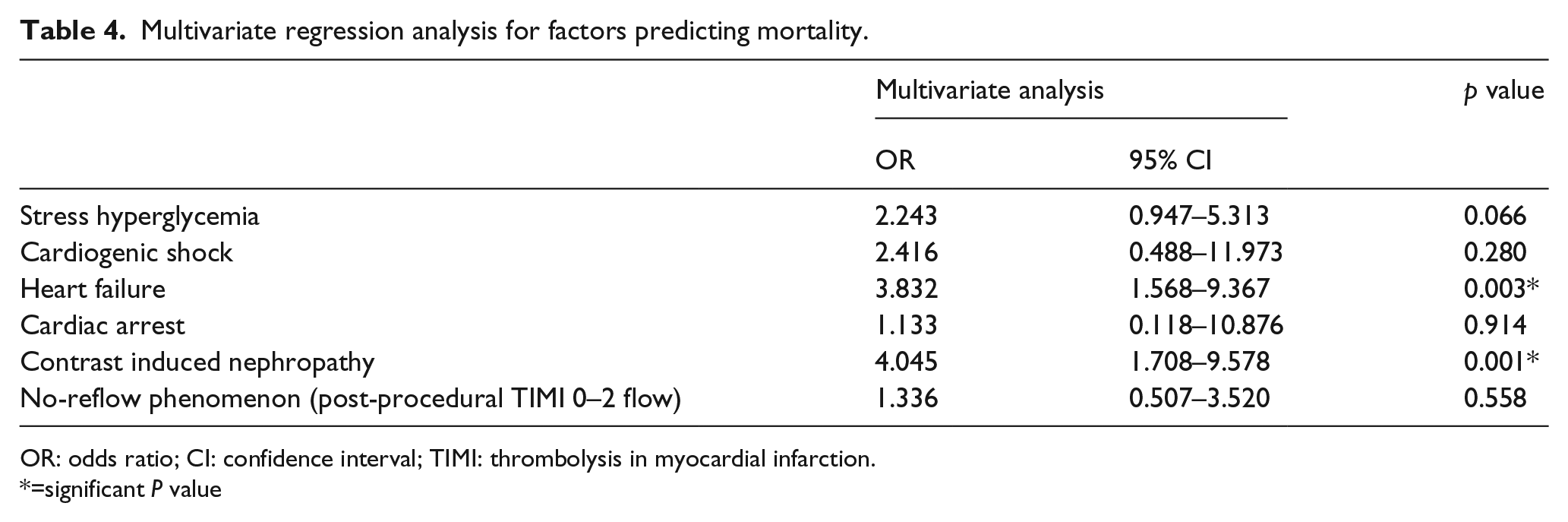
OR: odds ratio; CI: confidence interval; TIMI: thrombolysis in myocardial infarction.
=significant P value
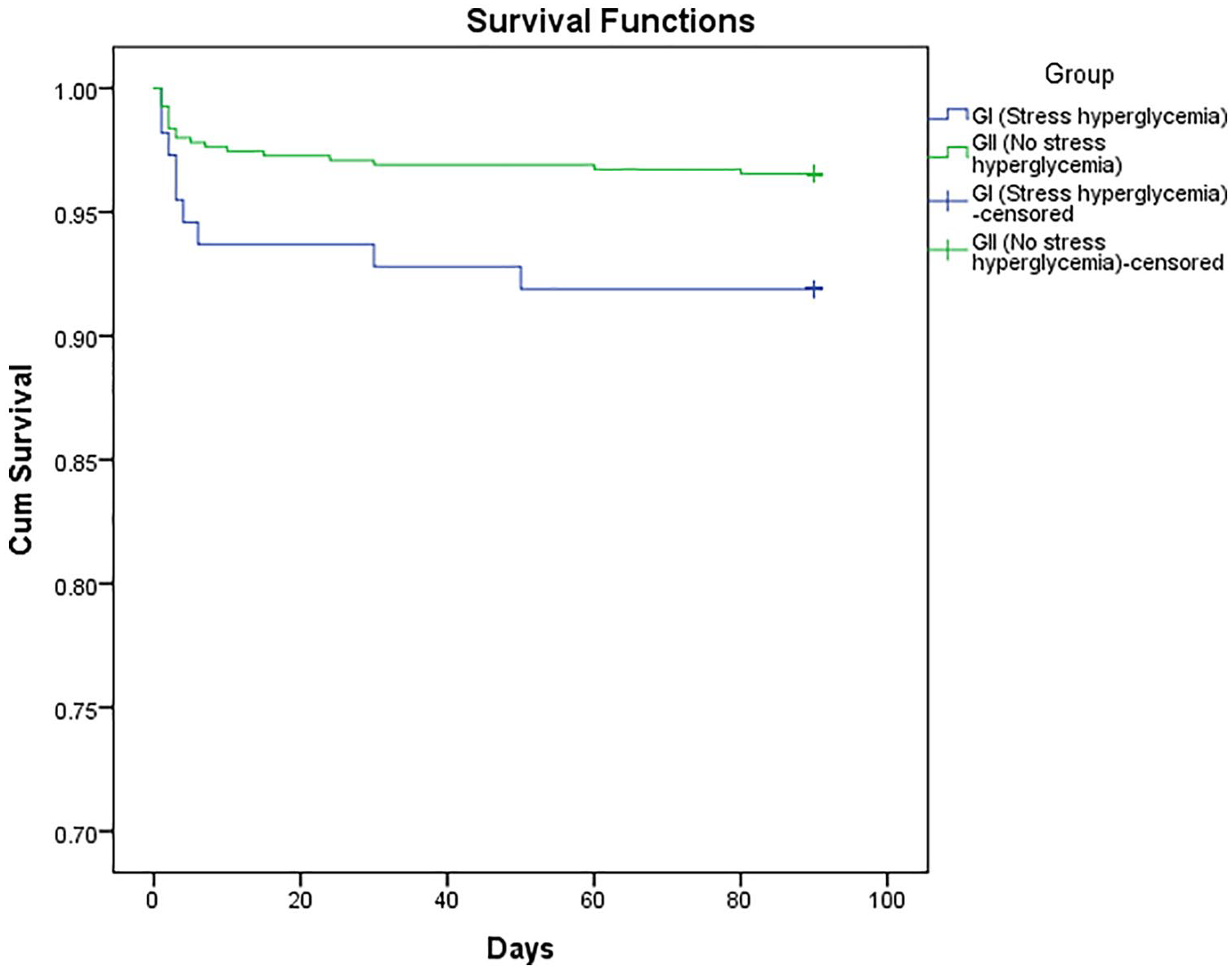
Kaplan–Meier curve showing survival function in patients with stress hyperglycemia (group I) and patients without stress hyperglycemia (group II) with better survival function in group II.
Discussion
Hyperglycemia in the setting of STEMI may be transient and stress induced, rather than a reflection of underlying gluco-metabolic state of the patient. Stress hyperglycemia is most probably induced by the acute release of catecholamine, cytokines and cortisol in the acute stage of myocardial infarction, but the mechanisms have not been fully elucidated; also, the evaluation and management of these patients remain challenging and uncertain. 9 Stress hyperglycemia in patients with STEMI seems to be transition phenomenon of detrimental effects rather than basic glucose metabolism. 10 Hyperglycemia can occur because of increasing levels of catecholamines, steroids, glucagon and decreasing levels of insulin due to stress. Moreover, inhibition of pancreatic beta cells caused by increasing levels of catecholamines could be another cause due to stress. 11 This response of the autonomic nervous system is associated with larger infarct size, heart failure and hemodynamic instability. 12 Several clinical studies have shown that acute increase in plasma glucose level causes several adverse effects, including oxidative stress, endothelial dysfunction, inflammation, apoptosis and hypercoagulability state that may contribute to worse outcomes in patients with STEMI.10–13 Esposito et al. 13 noticed that plasma cytokine levels increased as plasma glucose level increased during administration of consecutive pulses of intravenous glucose and immediately returned to normal levels as plasma glucose returned to normal levels.
The incidence of stress hyperglycemia in the current study was 16.8%. Norhammar et al. 14 demonstrated a high prevalence of impaired glucose tolerance and undiagnosed diabetes (35% and 31%, respectively) in a prospective study of 181 non-diabetic patients with acute myocardial infarction. In previous studies, the prevalence of stress hyperglycemia on admission ranged from 20% to 50% of patients with STEMI, although the exact definition of stress hyperglycemia has not been established.15,16 Nakamura et al., 17 who studied the impact of acute hyperglycemia during primary stent implantation in patients with STEMI reported that glucose level >11.0 mmol/L on admission was observed in 31% of all subjects and 15% of non-preexisting diabetic subjects.
The independent predictors of stress hyperglycemia in our study were family history of DM, body mass index >24 kg/m2 and cardiogenic shock on admission by multivariate regression analysis. The other major findings of this study were (1) stress hyperglycemia in non-diabetic patients with STEMI was associated with high mortality, (2) incidence of no reflow after PPCI was higher in stress hyperglycemia group and (3) cardiogenic shock and contrast induced nephropathy were significantly higher in patients with stress hyperglycemia. Several studies have demonstrated that hyperglycemia in the setting of acute myocardial infarction is an independent predictor of mortality regardless of diabetic status.16,18,19 Two of these studies showed that non-diabetic patients with hyperglycemia have higher mortality than diabetic patients with hyperglycemia.16,19 This may be explained by less aggressive medical treatment in the non-diabetic cohort; this justifies the importance of identifying and adequately treating stress hyperglycemia in non-diabetic patients with acute myocardial infarction. This is in accordance with several other reports. In HORIZONS-AMI trial, 20 all patients were managed with PPCI and hyperglycemia (serum glucose level more than 156 mg/dL) was associated with higher mortality rates and higher incidence of re-infarction and bleeding. In a large study evaluating long-term prognosis after acute myocardial infarction, non-diabetic patients who had admission blood glucose levels more than 200 mg/dL had mortality rate similar to that of patients who had established DM (42.6% and 43.1%, respectively). 19 Cooperative Cardiovascular Project identified 141,680 patients with acute myocardial infarction and reported that 30 days and 1 year mortality rate increases as glucose level on admission increases. Interesting point is that non-diabetics mortality is increasing as glucose level increases. 21
Our result showed that higher blood glucose levels on admission were associated with reduced TIMI flow after PPCI in patients with STEMI. The no reflow phenomenon, which is characterized by impairment of myocardial perfusion despite reopening of the epicardial coronary artery, is a predictive of poor prognosis. 22 Takahashi et al. 23 reported that acute hyperglycemia attenuates the protective effects of pre-infarction angina on micro-vascular function in patients with acute myocardial infarction. Several mechanisms are thought to be involved in the development of no reflow phenomenon and micro-vascular dysfunction. Micro-emboli associated with PPCI procedure may be a major cause of micro-vascular dysfunction. Micro-vascular plugging by neutrophils and platelets, inflammation, interstitial edema, endothelial dysfunction and oxidative stress may be involved in its pathogenesis and hyperglycemia could enhance these factors.24,25 Intracoronary thrombectomy may prevent or improve the no reflow phenomenon. The no reflow phenomenon is a predictor of infarct size and worse outcome after STEMI. 26 The incidence of contrast induced nephropathy in our study in patients with stress hyperglycemia was 22 (19.8%) vs 64 (11.7%) in group II with p value = 0.020. In agreement with our results, Marenzi et al. 27 who studied acute hyperglycemia and its relation to contrast induced nephropathy in PPCI reported that 148 (19%) patients had acute hyperglycemia and 113 (14.5%) patients developed contrast induced nephropathy and noticed that patients with acute hyperglycemia had a twofold higher incidence of contrast induced nephropathy than those without acute hyperglycemia.
Conclusion
Stress hyperglycemia on admission is a strong predictor of mortality in patients with STEMI, blood glucose levels should be monitored closely in patients with STEMI, regardless of diabetic status and based on the current evidence; consideration should be taken to maintain blood glucose level less than 140 mg/dL. Stress hyperglycemia was associated with higher mortality, higher incidence of no reflow phenomenon. Cardiogenic shock and contrast induced nephropathy were significantly higher in patients with stress hyperglycemia.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.