
Abstract
Objective
To explore the association between in-hospital haemoglobin decline and long-term mortality and major adverse cardiovascular and cerebrovascular events (MACCE) among ST-segment elevation myocardial infarction (STEMI) patients treated with primary percutaneous coronary intervention (PCI).
Methods
This retrospective analysis included adult patients who underwent primary PCI for STEMI. Haemoglobin levels were recorded at admission and 48–72 h later. Patients were divided into two groups based on the extent of haemoglobin decline: low (<3 g/dl or no decline) and high (≥3 g/dl). The primary endpoint was all-cause mortality at long-term follow-up. The secondary endpoint was MACCE.
Results
Patients were divided into two groups: low group (n = 665) and high group (n = 111). The mortality rate was significantly higher in the high group (72 of 111 patients; 65%) than in the low group (185 of 655 patients; 28%). Propensity score matching confirmed this association, with higher mortality (41 of 79 patients [52%] versus 25 of 79 patients [32%]) and MACCE rates (56 of 79 patients [71%] versus 41 of 79 patients [52%]) in the high group compared with the low group, respectively.
Conclusion
There was a significant association between in-hospital haemoglobin decline, even without visible bleeding, and increased long-term mortality and MACCE in STEMI patients undergoing primary PCI.
Keywords
Introduction
Cardiovascular diseases are among the leading causes of death worldwide, with ST-segment elevation myocardial infarction (STEMI) representing a critical condition necessitating immediate medical intervention.1,2 Primary percutaneous coronary intervention (PCI), the primary treatment for STEMI, aims to quickly restore cardiac blood flow and minimize myocardial damage.3,4 However, a significant yet often overlooked complication for STEMI patients undergoing primary PCI is the decline in haemoglobin levels, affecting both short- and long-term health outcomes.5,6 Haemoglobin, crucial for oxygen transport in the blood, commonly decreases during the hospitalization of STEMI patients.7,8 This decline is multifactorial, arising from blood loss due to medical procedures and tests, which is often worsened by anticoagulant medications and other issues such as gastrointestinal bleeding, dilution from intravenous fluids and decreased erythropoietin production in the context of renal dysfunction.9–12 Additionally, hidden bleeding from intensive antithrombotic treatments and conditions such as inflammation and stress polycythaemia contribute significantly to this reduction.13,14
Although the immediate consequences of decreased haemoglobin are recognized in clinical settings, the long-term effects, particularly for STEMI patients who have undergone primary PCI, are less well-understood. This current study aimed to address this knowledge gap by investigating the association between in-hospital haemoglobin decline and long-term mortality in STEMI patients who have undergone primary PCI.
Patients and methods
Study design and population
This single-centre, retrospective cohort study included consecutive adult patients who were diagnosed with STEMI based on clinical findings, electrocardiographic changes and biomarker levels according to the current universal definition of myocardial infarction at the Department of Cardiology, Izmir Katip Çelebi University, Atatürk Training and Research Hospital, Izmir, Turkey between May 2009 and March 2018. 15 The inclusion criteria were as follows: (i) ≥18 years of age; (ii) patients with in-hospital haemoglobin values; (iii) patients who did not experience a fatal event in the first 24 h. The exclusion criteria were as follows: (i) patients with blood disorders, such as chronic anaemia; (ii) patients who had blood transfusions in the 3 months prior to the study; (iii) patients who had undergone surgery in the 3 months prior to the study; (iv) patients on treatments such as chemotherapy or radiation therapy; (v) patients with serious conditions such as active cancer that could independently influence the study’s results.
Patient stratification in this study was based on the extent of haemoglobin decline. A low group was defined as no haemoglobin decrease (patients with zero or a negative difference between baseline and haemoglobin values at 48–72 h) or <3 g/dl haemoglobin decrease. A high group was defined as a haemoglobin decrease ≥3 g/dl. The Bleeding Academic Research Consortium definition for bleeding was used. 16
The study followed the principles of the Declaration of Helsinki and was approved by the Medical Ethics Committee of Izmir Katip Çelebi University, Atatürk Training, and Research Hospital (no. 2023-0551). Due to the study’s retrospective nature, the need for informed consent was waived by the Medical Ethics Committee. All patient details were de-identified. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 17
Outcomes
Information regarding mortality and major adverse cardiovascular and cerebrovascular events (MACCE) was obtained from a national electronic database, an institutional electronic database and phone calls with patients/relatives. The primary endpoint was all-cause long-term mortality. The secondary endpoint was long-term MACCE at a median follow-up of 6.9 years. MACCE was a composite of all-cause mortality, myocardial reinfarction (defined as STEMI or non-ST-segment elevation myocardial infarction), target vessel revascularization (defined as any repeat revascularization in the epicardial vessel [main branch or side branches]) and cerebrovascular events (including the occurrence of new neurological deficits such as stroke or transient ischaemic attack confirmed through radiological imaging). The composite endpoint was assessed by time to the first event. Clinical follow-up information was obtained by review of clinic visits or by telephone. Clinical visits were conducted face-to-face or by telephone at 3-month intervals in the first year after STEMI and at 6-month intervals thereafter. Mortality or MACCE data for patients lost to follow-up were confirmed using the National Death Records and National Social Security Institution.
Statistical analyses
In terms of a power analysis, considering total mortality rates, the study needed to recruit 21 participants for the high group and 116 participants for the low group, to have 80% power with a 5% type 1 error level. The power of the study increased to 95% with the selection of 138 low-risk and 25 high-risk patients with 5% type 1 error level.
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 26.0 (IBM Corp., Armonk, NY, USA) and R statistical package (R ggstream 0.1.0; R Foundation for Statistical Computing, Vienna, Austria). Continuous variables are presented as mean ± SD and categorical variables are shown as the number of patients (%). Either the Student’s t-test or the Mann–Whitney U-test was used to compare values between the two groups, as appropriate. χ2-test was used to compare categorical variables. Univariate and multivariate Cox regression analyses were performed to identify predictors of long-term mortality. A propensity score matching was performed to create a matched dataset (low group versus high group). The following covariates were considered for balance between groups: age, stroke history, thrombus aspiration device use, intra-aortic balloon pump use, vasopressor use, Killip class, haemoglobin at admission and estimated glomerular filtration rate (eGFR). Matching based on propensity score yielded 79 patients in each group. The cumulative incidence of the primary and secondary endpoints was estimated using the Kaplan–Meier method. Two-sided P-values <0.05 were considered statistically significant.
Results
The study evaluated 766 patients with STEMI stratified into two groups based on the extent of in-hospital haemoglobin decline: the low group (n = 655) and the high group (n = 111). Table 1 presents the baseline characteristics of the study population. The mean ± SD age was significantly higher in the high group (64.6 ± 12.1 years) compared with the low group (58.8 ± 12.4 years; P < 0.001). Sex distribution was similar between the groups, with males representing 82% (538 of 655 patients) and 83% (92 of 111 patients) of the low and high groups, respectively. There were no significant differences in the prevalence of diabetes mellitus, hypertension, previous coronary artery disease (CAD), hyperlipidaemia or smoking between the two groups. However, previous stroke (P = 0.021) and chronic obstructive pulmonary disease (P = 0.037) were significantly more prevalent in the high group. Multivessel disease was significantly more common in the high group (64%) compared with the low group (49%; P = 0.003). The use of inotropic agents (P < 0.001), Killip class >2 (P < 0.001), intra-aortic balloon pump (P < 0.001) and thrombus aspiration device usage (P = 0.001) were significantly higher in the high group than in the low group. Final Thrombolysis In Myocardial Infarction flow rates were significantly lower in the high group (90 of 111 patients; 81%) compared with the low group (592 of 655 patients; 90%) (P = 0.011). No significant differences were found in medical treatments at admission, including aspirin, clopidogrel, oral anticoagulants, beta blockers, angiotensin-converting enzyme inhibitors/angiotensin receptor blockers and statins between the two groups. Left ventricular ejection fraction percentages were similar between the two groups.
Demographic and clinical characteristics of patients (n = 766) who experienced ST-segment elevation myocardial infarction and underwent primary percutaneous coronary intervention who were enrolled in a study investigating the association between in-hospital haemoglobin decline and long-term mortality.

Data presented as mean ± SD or n of patients (%).
Student’s t-test or the Mann–Whitney U-test were used to compare continuous data; and χ2-test was used to compare categorical data; NS, no significant between-group difference (P ≥ 0.05).
A total of 69 patients died in the hospital, so the number of patients alive at discharge was 697. The evaluation was made based on this number of patients.
CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease; LVEF, left ventricular ejection fraction; IABP, intra-aortic balloon pump; GpIIb/IIIa inhibitors, glycoprotein IIb/IIIa inhibitors; TIMI-3 flow, Thrombolysis in Myocardial Infarction flow grade 3; LMCA, left main coronary artery; LAD, left anterior descending artery; CX, circumflex artery; RCA, right coronary artery; P2Y12 inhibitors, purinergic receptor P2Y, G-protein coupled, 12 protein inhibitors; OAC, oral anticoagulants; ACE/ARB: angiotensin-converting enzyme inhibitor/angiotensin receptor blockers.
White blood cell count and blood glucose levels were similar between the two groups (Table 2). The mean ± SD total cholesterol level was significantly lower in the high group compared with the low group (169.2 ± 40.8 mg/dl versus 183.8 ± 48.3 mg/dl, respectively; P = 0.005). The mean ± SD eGFR was significantly lower in the high group compared with the low group (81.5 ± 28.2 ml/min/1.73 m2 versus 92.4 ± 24.3 ml/min/1.73 m2, respectively; P < 0.001). The mean ± SD haemoglobin levels at admission were significantly lower in the low group compared with the high group (13.9 ± 1.9 g/dl versus 15.1 ± 1.6 g/dl, respectively; P < 0.001).
Baseline laboratory findings of patients (n = 766) who experienced ST-segment elevation myocardial infarction and underwent primary percutaneous coronary intervention who were enrolled in a study investigating the association between in-hospital haemoglobin decline and long-term mortality.

Data presented as mean ± SD.
aStudent’s t-test or the Mann–Whitney U-test were used to compare continuous data; NS, no significant between-group difference (P ≥ 0.05).
WBC, white blood cell count; eGFR, estimated glomerular filtration rate.
There was overt bleeding in 94 of 766 patients. Among patients with overt bleeding, 260 of 766 patients (34%) had BARC type 2 bleeding, while 121 of 766 patients (16%) had BARC type 3 or 5 bleeding. There were instances of intracranial bleeding (two patients), gastrointestinal bleeding (five patients), coronary artery bypass graft surgery-related bleeding within 48 h after PCI (five patients), urinary system bleeding (one patient) and retroperitoneal bleeding (two patients).
The long-term mortality rate was significantly higher in the high group (72 of 111 patients; 65%) than in the low group (185 of 655 patients; 28%; P < 0.001) (Table 3). Kaplan–Meier mortality curves for the two groups before matching are shown in Figure 1. The high group had a significantly higher MACCE rate compared with the low group (87 of 111 patients [78%] versus 349 of 655 patients [53%], respectively; P < 0.001 (Figure 2 and Table 3). Both mortality and MACCE rates were higher in the high group in patients with overt bleeding before matching (Figures 3 and 4). Matching based on propensity scores yielded 79 patients in each group (Tables 3–5) and the analyses showed that the mortality and MACCE rates remained significantly higher in the high group compared with the low group (P = 0.010 and P = 0.014, respectively) (Table 3, Figures 5 and 6). Kaplan–Meier event curves for MACCE and mortality in patients with overt bleeding after matching are shown in Figures 7 and 8.
Long-term outcomes in patients (n = 766) who experienced ST-segment elevation myocardial infarction and underwent primary percutaneous coronary intervention who were enrolled in a study investigating the association between in-hospital haemoglobin decline and long-term mortality.
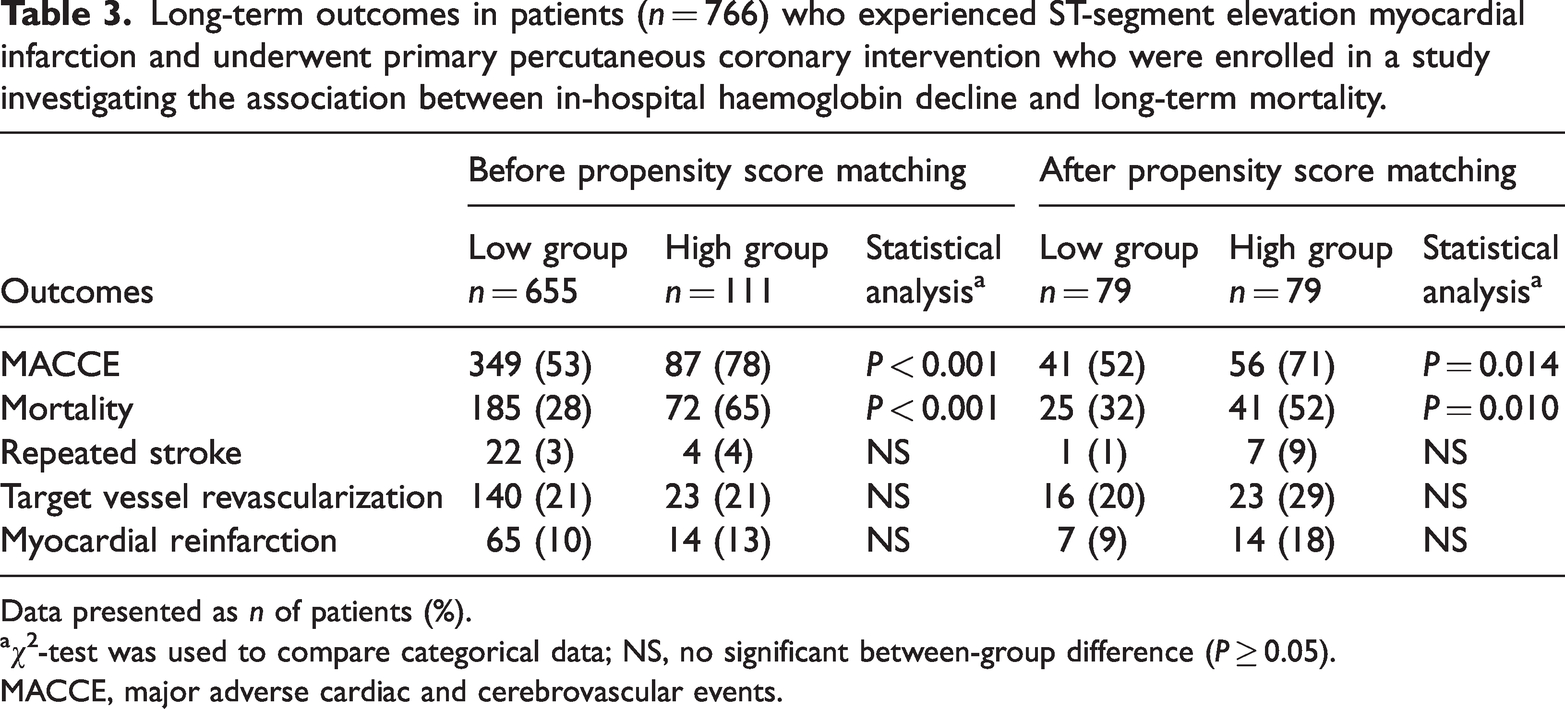
Data presented as n of patients (%).
χ2-test was used to compare categorical data; NS, no significant between-group difference (P ≥ 0.05).
MACCE, major adverse cardiac and cerebrovascular events.
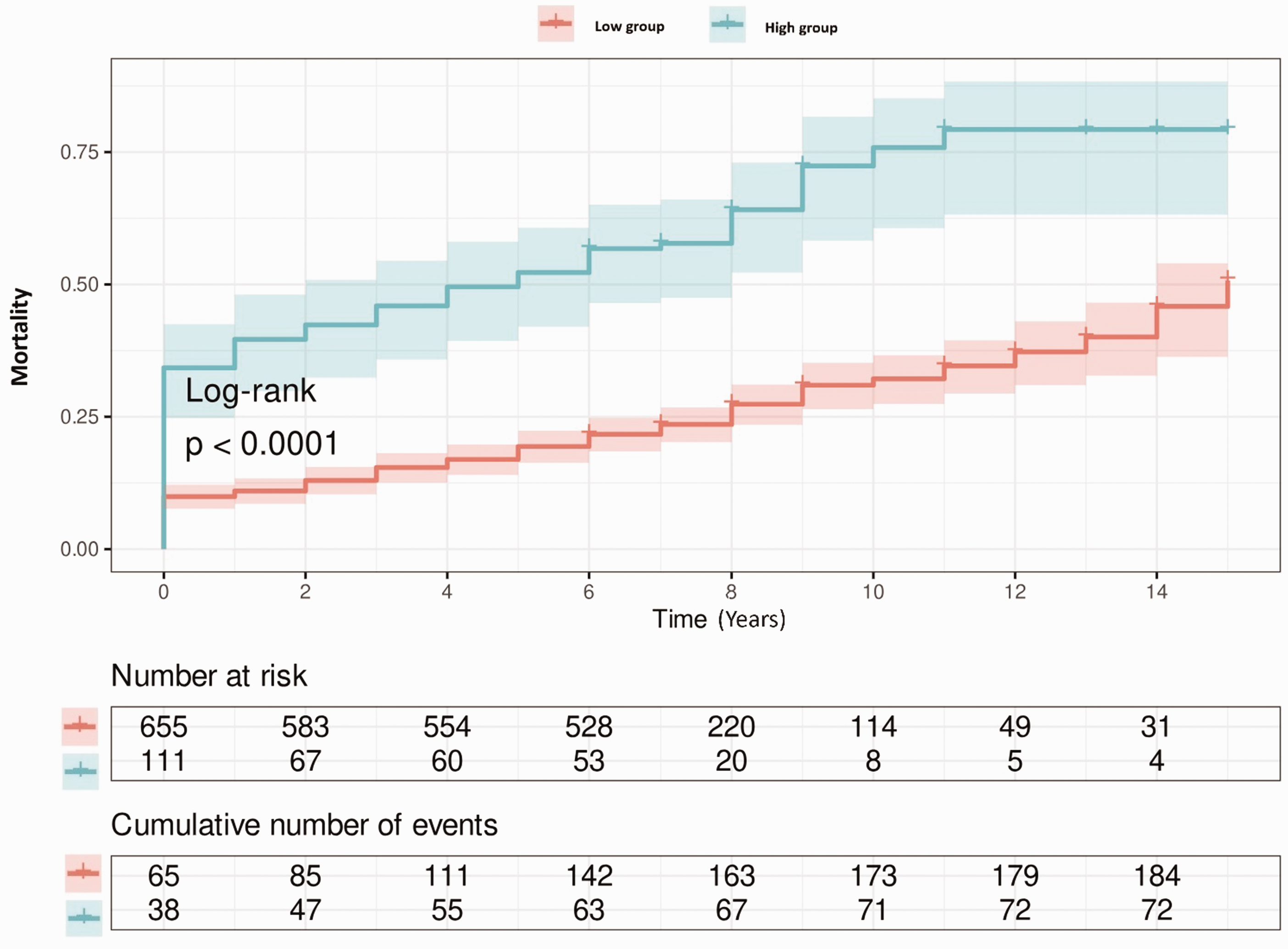
Mortality before propensity score matching in the entire cohort of patients (n = 766) who experienced ST-segment elevation myocardial infarction and underwent primary percutaneous coronary intervention who were enrolled in a study investigating the association between in-hospital haemoglobin decline and long-term mortality. Patients were stratified according to the extent of haemoglobin decline into low and high groups. The colour version of this figure is available at: http://imr.sagepub.com.

Major cardiovascular and cerebrovascular events (MACCE) before propensity score matching in the entire cohort of patients (n = 766) who experienced ST-segment elevation myocardial infarction and underwent primary percutaneous coronary intervention who were enrolled in a study investigating the association between in-hospital haemoglobin decline and long-term mortality. Patients were stratified according to the extent of haemoglobin decline into low and high groups. The colour version of this figure is available at: http://imr.sagepub.com.

Mortality before propensity score matching in patients (n = 94) with overt bleeding who experienced ST-segment elevation myocardial infarction and underwent primary percutaneous coronary intervention who were enrolled in a study investigating the association between in-hospital haemoglobin decline and long-term mortality. Patients were stratified according to the extent of haemoglobin decline into low and high groups. The colour version of this figure is available at: http://imr.sagepub.com.

Major cardiovascular and cerebrovascular events (MACCE) before propensity score matching in patients (n = 94) with overt bleeding who experienced ST-segment elevation myocardial infarction and underwent primary percutaneous coronary intervention who were enrolled in a study investigating the association between in-hospital haemoglobin decline and long-term mortality. Patients were stratified according to the extent of haemoglobin decline into low and high groups. The colour version of this figure is available at: http://imr.sagepub.com.
Demographic and clinical characteristics of propensity score matched patients (n = 158) who experienced ST-segment elevation myocardial infarction and underwent primary percutaneous coronary intervention who were enrolled in a study investigating the association between in-hospital haemoglobin decline and long-term mortality.
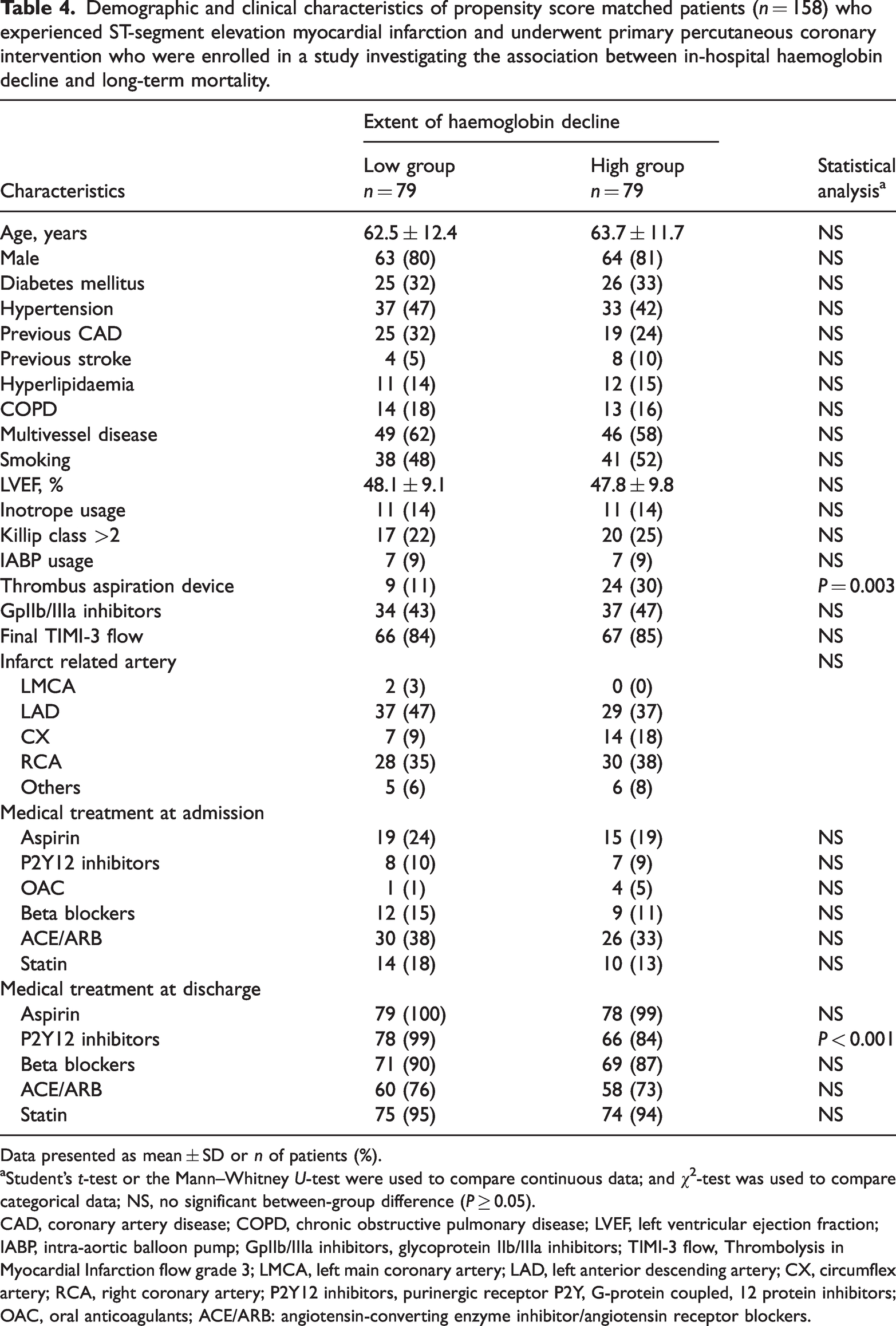
Data presented as mean ± SD or n of patients (%).
Student’s t-test or the Mann–Whitney U-test were used to compare continuous data; and χ2-test was used to compare categorical data; NS, no significant between-group difference (P ≥ 0.05).
CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease; LVEF, left ventricular ejection fraction; IABP, intra-aortic balloon pump; GpIIb/IIIa inhibitors, glycoprotein IIb/IIIa inhibitors; TIMI-3 flow, Thrombolysis in Myocardial Infarction flow grade 3; LMCA, left main coronary artery; LAD, left anterior descending artery; CX, circumflex artery; RCA, right coronary artery; P2Y12 inhibitors, purinergic receptor P2Y, G-protein coupled, 12 protein inhibitors; OAC, oral anticoagulants; ACE/ARB: angiotensin-converting enzyme inhibitor/angiotensin receptor blockers.
Baseline laboratory findings of propensity score matched patients (n = 158) who experienced ST-segment elevation myocardial infarction and underwent primary percutaneous coronary intervention who were enrolled in a study investigating the association between in-hospital haemoglobin decline and long-term mortality.
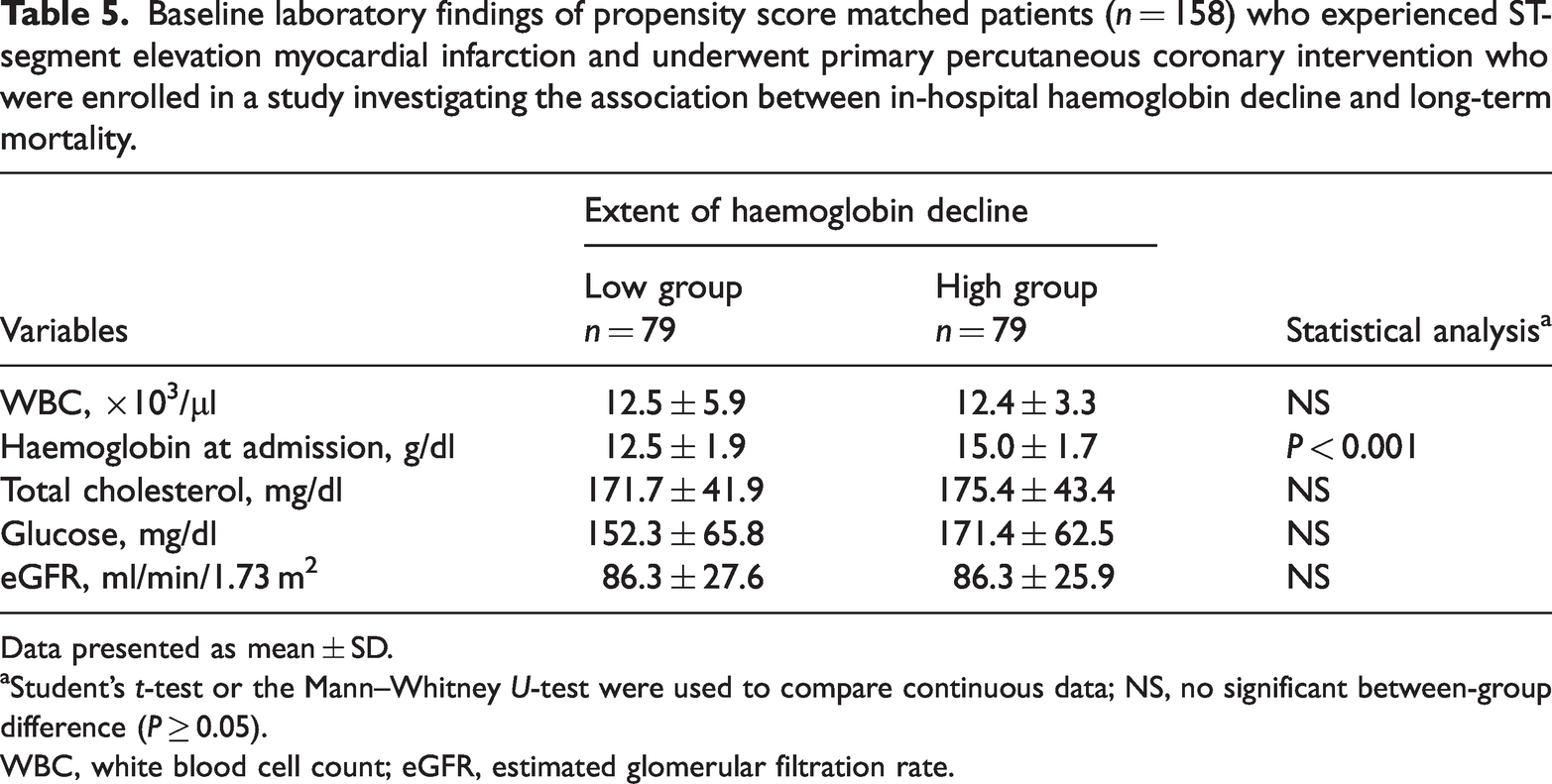
Data presented as mean ± SD.
Student’s t-test or the Mann–Whitney U-test were used to compare continuous data; NS, no significant between-group difference (P ≥ 0.05).
WBC, white blood cell count; eGFR, estimated glomerular filtration rate.

Mortality after propensity score matching in patients (n = 158) who experienced ST-segment elevation myocardial infarction and underwent primary percutaneous coronary intervention who were enrolled in a study investigating the association between in-hospital haemoglobin decline and long-term mortality. Patients were stratified according to the extent of haemoglobin decline into low and high groups. The colour version of this figure is available at: http://imr.sagepub.com.

Major cardiovascular and cerebrovascular events (MACCE) after propensity score matching in patients (n = 158) who experienced ST-segment elevation myocardial infarction and underwent primary percutaneous coronary intervention who were enrolled in a study investigating the association between in-hospital haemoglobin decline and long-term mortality. Patients were stratified according to the extent of haemoglobin decline into low and high groups. The colour version of this figure is available at: http://imr.sagepub.com.

Mortality after propensity score matching in patients (n = 37) with overt bleeding who experienced ST-segment elevation myocardial infarction and underwent primary percutaneous coronary intervention who were enrolled in a study investigating the association between in-hospital haemoglobin decline and long-term mortality. Patients were stratified according to the extent of haemoglobin decline into low and high groups. The colour version of this figure is available at: http://imr.sagepub.com.
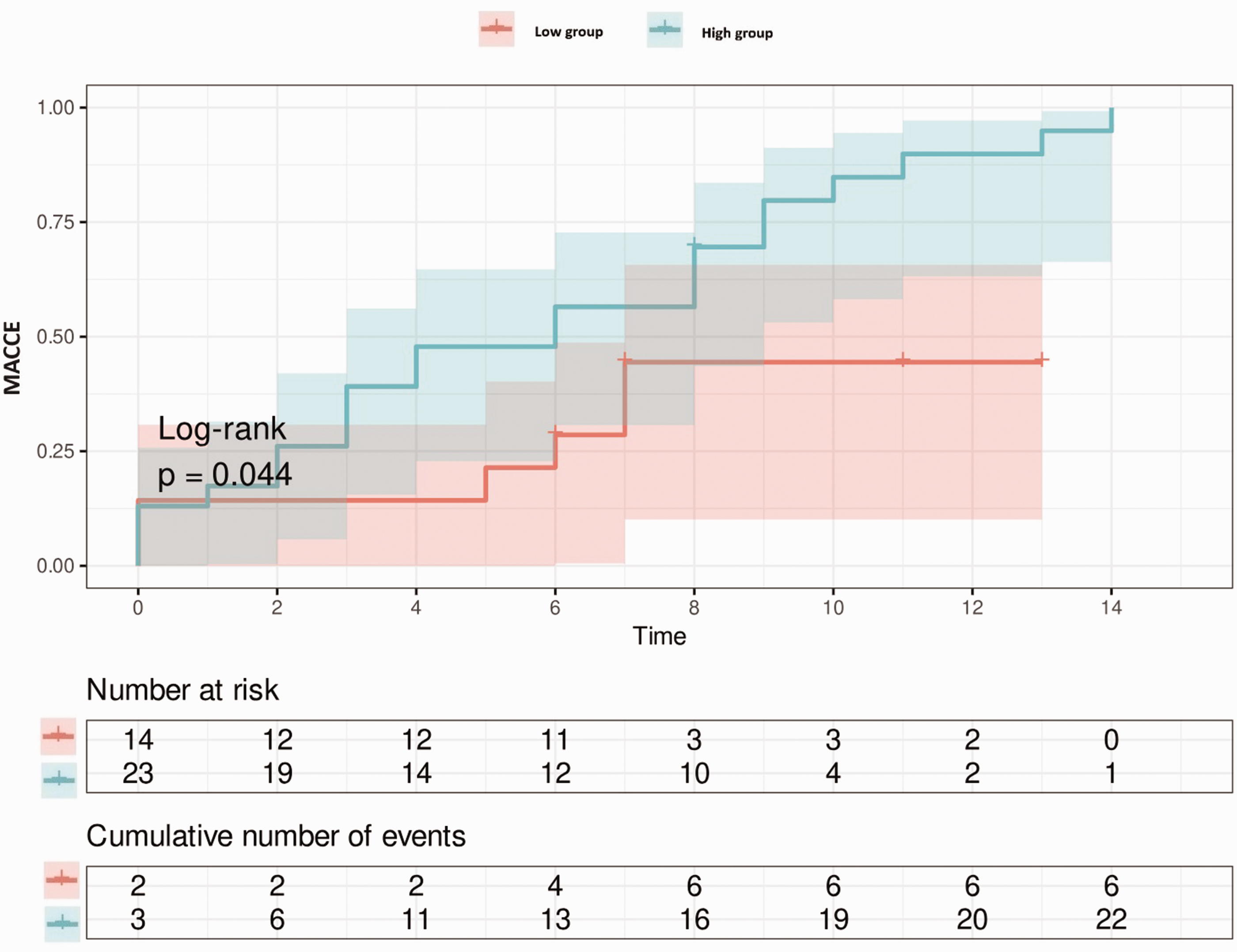
Major cardiovascular and cerebrovascular events (MACCE) after propensity score matching in patients (n = 37) with overt bleeding who experienced ST-segment elevation myocardial infarction and underwent primary percutaneous coronary intervention who were enrolled in a study investigating the association between in-hospital haemoglobin decline and long-term mortality. Patients were stratified according to the extent of haemoglobin decline into low and high groups. The colour version of this figure is available at: http://imr.sagepub.com.
Discussion
The current retrospective study demonstrated that a decrease in haemoglobin levels of 3 g/dL or more during hospitalization, even without visible bleeding, was independently linked to a higher risk of MACCE, with this association predominantly driven by increased mortality in STEMI patients undergoing primary PCI.
Haemoglobin, as the primary oxygen-carrying molecule in the bloodstream, plays a crucial role in ensuring adequate tissue oxygenation. This becomes particularly pivotal in the context of STEMI, an acute and critical cardiac event. In such cases, optimizing myocardial oxygenation is paramount for preserving heart function and facilitating recovery. 18 Herein, the role of PCI, especially in the context of STEMI, is of immense significance due to its well-established effectiveness in restoring blood flow and mitigating cardiac injury. 18
The current study also established a positive correlation between the degree of haemoglobin decline and the increased risk of long-term mortality. These findings support similar conclusions from previous studies.19,20 Another study demonstrated that an in-hospital haemoglobin decline of >3 g/dl was independently linked to an increased risk of all-cause mortality at 180 days in non-overt bleeding acute myocardial infarction patients admitted to the intensive care unit, irrespective of baseline haemoglobin levels and invasive treatment. 21
The decline in haemoglobin levels can have several implications for adverse clinical outcomes. One key mechanism is the reduction in haemoglobin concentration, which directly impacts the blood’s ability to carry oxygen. This decrease in oxygen-carrying capacity can potentially worsen myocardial ischaemia, a condition characterized by reduced blood flow to the heart muscle.22,23 Furthermore, after a STEMI event, an inflammatory response occurs. A previous study highlighted this inflammatory response and its role in compounding the challenges associated with declining haemoglobin levels. 13 The combination of decreased haemoglobin and the inflammatory response can have detrimental effects on myocardial health. Additionally, following an acute myocardial infarction, there might be changes in blood viscosity. These changes can impede the efficient delivery of oxygen to the myocardium, further exacerbating the impact of declining haemoglobin levels on clinical outcomes. Ensuring adequate oxygen supply to the heart muscle is crucial for its proper functioning and overall cardiovascular health. 14
The aetiology of declining haemoglobin levels during hospitalization is multifaceted, stemming from various factors. These encompass procedural complications such as post-PCI bleeding events;11,24 and challenges like haemodilution or acute kidney injuries associated with peri-procedural haemoglobin reductions. 25 The heterogeneity in the underlying causes underscores the importance of adopting a comprehensive approach to patient care. Furthermore, previous research underscores the need to identify predictors of significant bleeding events in the context of acute coronary syndromes.26,27
The outcomes of this current study demonstrate that haemoglobin decline subsequent to primary PCI in STEMI patients is linked to long-term mortality, corroborating the findings of analogous investigations. 28 These findings underscore the substantial impact of haemoglobin decline on long-term patient outcomes, mirroring the results of previous research. 29 Furthermore, there is evidence from other studies indicating that haemoglobin decline is associated with a heightened risk of 1-year mortality, even in the absence of in-hospital bleeding events. 12 This comprehensive perspective accentuates the potential critical role of managing haemoglobin levels in the broader context of cardiovascular disease management.
This current study had several limitations. First, it was a single-centre study, which limits the direct generalizability of the results to all STEMI populations. Secondly, the retrospective design might have left some variables uncontrolled, potentially influencing the outcomes. Thirdly, this study had a relatively small sample size. All of these limitations should be considered when interpreting the findings.
In conclusion, in patients with STEMI who were underwent primary PCI, a high in-hospital haemoglobin decline was associated with an increased risk of both MACCE and mortality at long-term follow-up.
Footnotes
Author contributions
All authors contributed to the study’s conception and design. Material preparation, data collection and analysis were performed by T.K., H.S.I., F.E., G.A. and A.C. The primary draft of the manuscript was written by F.E., T.K. and U.K. Writing, review and editing of the final version of the manuscript were carried out by T.K., F.E., H.S.I., A.C. and U.K. M.K. and T.K. added critical points to the study. All authors read and approved the final manuscript.
Availability of data and materials
The data supporting this study’s findings are available from the corresponding author upon reasonable request.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.