
Abstract
Although diabetes is rapidly increasing in Asia and has been shown to be associated with worse cardiac surgery outcomes, no research has been done to study the impact of diabetes on cardiac surgery outcomes in a Southeast Asian cohort. Hence, this study aims to delineate the predictors and impact of diabetes after cardiac surgery in a multi-ethnic Southeast Asian cohort. We analysed data from 2831 adult patients undergoing elective cardiac surgery, from 2008 to 2010 in Singapore. Diabetes was found to significantly increase the odds of intensive care unit readmission by 1.70 (95% confidence interval 1.171–2.480, p = 0.005), postoperative infection by 1.73 (95% confidence interval 1.003–2.976, p = 0.049), acute kidney injury by 1.36 (95% confidence interval 1.137–1.626, p = 0.001), postoperative hyperglycaemia by 6.00 (95% confidence interval 4.893–7.348, p < 0.001), and new need for dialysis by 1.71 (95% 1.086–5.360, p = 0.021). In conclusion, diabetes is associated with increased risk for renal dysfunction, hyperglycaemia, and infection after cardiac surgery, similar to the relative risks of diabetes patients observed in Western populations.
Keywords
Introduction
Diabetes mellitus is a major health problem worldwide today and is estimated to affect 8.4% of the world’s total population. 1 The majority of diabetes patients in the world live in Southeast Asia and the prevalence of the disease is increasing more rapidly in Asia than elsewhere.1,2 The prevalence of diabetes in patients undergoing cardiac surgery has been reported to be about 20% in Western cohorts 3 and is expected to be higher in Asian cohorts, given the higher prevalence of diabetes in Asian populations. 1 Furthermore, research has shown that diabetes is an important risk factor for coronary artery disease and is associated with poorer cardiac surgery outcomes in Western populations due to the poor quality of target vessels and comorbidities of diabetes.3,4
Yet, although diabetes has been shown to be associated with worse cardiac surgery outcomes and has a higher prevalence and ethnic association in Southeast Asia, no research has been done to study the impact of diabetes on cardiac surgery outcomes in the local Southeast Asian cohort. Hence, study aims to identify the predictors and impact of diabetes on perioperative cardiac surgery outcomes.
Methods
Study population
With SingHealth Centralised Institutional Review Board (CIRB) (IRB number 2008/137/D) approval and written informed consent from the patients before enrolment, a total of 3008 adult patients undergoing elective cardiac surgery were retrospectively included in this study. Of this, 117 patients were excluded from the study as they belonged to various ethnic groups apart from the three main ethnic groups in Singapore that were being studied: Chinese, Malay, and Indian. Of the remaining 2831 patients analysed, 46.7% (n = 1321) had diabetes. Patients with a known history of diabetes, preoperative random plasma glucose greater than 200 mg/dL or taking antidiabetic medications, or haemoglobin A1c (HbA1c) greater than 6.5% were analysed as diabetes patients.
Preoperative patient characteristics are shown in Table 1 with comparisons between patients with and without diabetes undergoing elective cardiac surgery. The average age was 59.4 ± 10.5 years and most patients were male (80.1%) and hypertensive (75.3%).
Preoperative patient characteristics of patients with and without diabetes undergoing cardiac surgery.
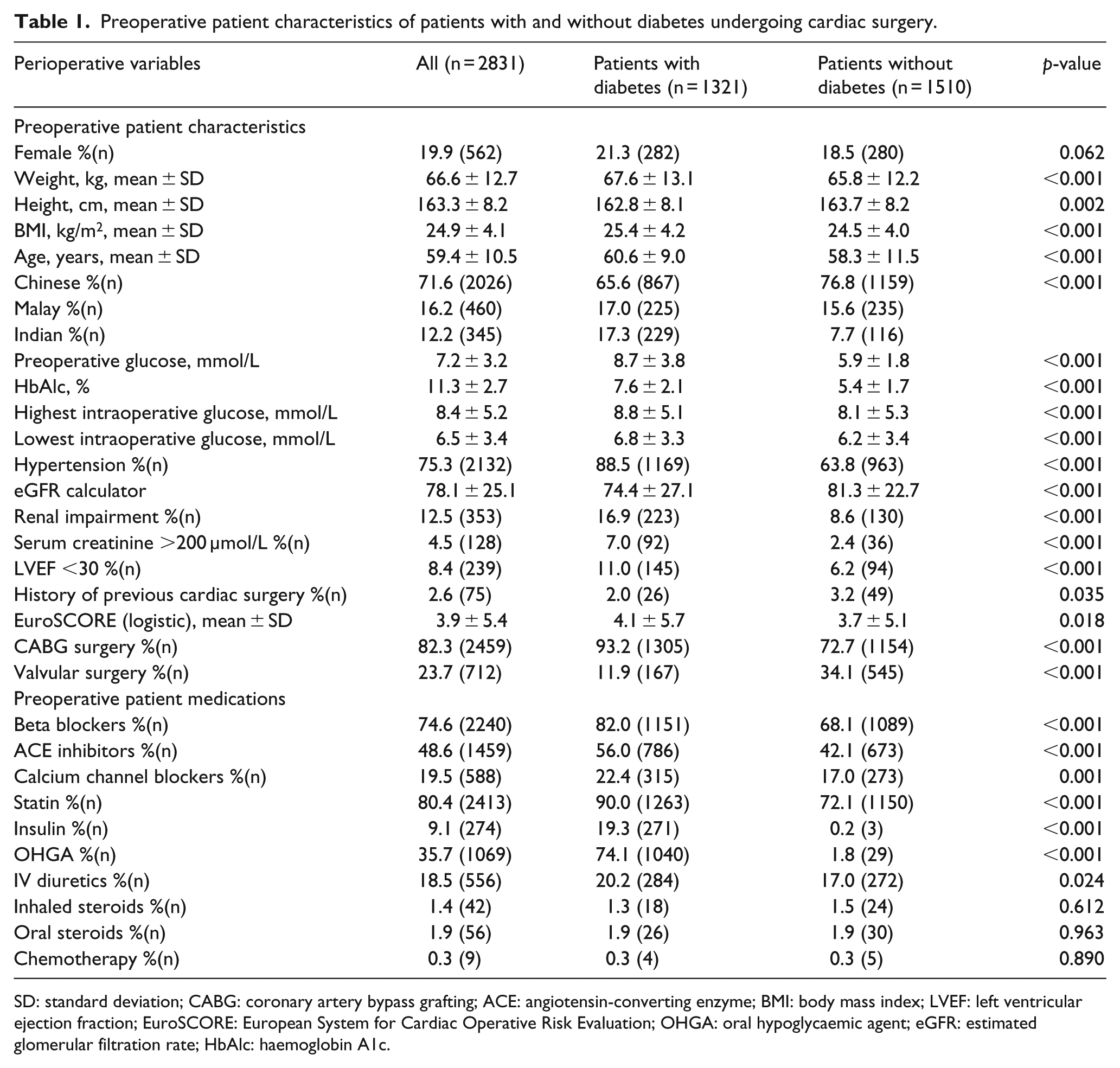
SD: standard deviation; CABG: coronary artery bypass grafting; ACE: angiotensin-converting enzyme; BMI: body mass index; LVEF: left ventricular ejection fraction; EuroSCORE: European System for Cardiac Operative Risk Evaluation; OHGA: oral hypoglycaemic agent; eGFR: estimated glomerular filtration rate; HbAlc: haemoglobin A1c.
Perioperative anaesthesia and surgical and perfusion management
Perioperative clinical practices and surgical management followed strict international standards. Anaesthesia was induced with intravenous induction agents (Propofol or Etomidate) and maintained with a balanced anaesthesia regime using low-dose fentanyl (10–20 μg kg−1) in addition to volatile agents (primarily Sevoflurane). Conventional cardiopulmonary bypass (CPB) circuits with heat exchangers, roller pumps, membrane oxygenators, arterial blood filters, venous reservoirs, and cardiotomy suction were utilised. Typically, 1300–1400 mL of primer was used in the CPB circuits. Perfusion targets include a hematocrit of >22%, mild-to-moderate hypothermia (32°C–35°C), nonpulsatile flow rate of 2.2–2.4 L min−1 m−2, mean arterial pressure of 50–70 mmHg, glucose levels of below 10 mmol/L, and activated clotting times of more than 400 s. Cold blood cardioplegia was used to achieve myocardial protection. Aprotinin was not utilised in any patients.
All patients were kept to a tight baseline blood glucose control within a range of 4–10 mmol/L, in accordance with hospital protocol and the ‘Society of Thoracic Surgeons Practice Guideline series: Blood Glucose Management During Adult Cardiac Surgery’. 5 In line with hospital protocol, glycaemic targets were strictly adhered to via insulin infusion and monitoring every 2–4 h or more frequently if required, up to the first 48 h.
Data collected
Data extracted from the patients were chosen a priori and include patient characteristics, risk factors, surgical data, and postoperative outcomes up to 30 days post-surgery including intensive care unit (ICU) mortality, readmission to ICU, length of stay in ICU, length of stay in high dependency unit (HDU), new onset cardiac arrhythmia, cardiac failure, cardiac tamponade, postoperative infections, and length of hospitalisation.
Perioperative outcomes were defined and categorised according to the ICD-10 coding (the 10th revision of the International Statistical Classification of Diseases and Related Health Problems) and noted from patient discharge summaries.
Postoperative hyperglycaemia was defined as a blood glucose level of more than 10 mmol/L (approximately 180 mg/dL) within the first 48 perioperative hours. 6 The remaining patients who were included were considered normoglycaemic for the purposes of this study.
Acute kidney injury (AKI) was determined based on the Acute Kidney Injury Network (AKIN) criteria and defined as an absolute increase in serum creatinine of ⩾26.4 mmol/L, and/or a ⩾50% increase in the serum creatinine to the peak postoperative from the preoperative serum creatinine. The estimated glomerular filtration rate (eGFR) was calculated via the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation, during the preoperative anaesthesia review, which has been previously validated in the local population. 7
Subsequently, we followed the reference cut-off for the eGFR in defining renal insufficiency:8,9 Stage 1 (representing normal kidney function with eGFR of ⩾90 mL/min/1.73 m2); Stage 2 (mild renal insufficiency with eGFR of ⩾60–89 mL/min/1.73 m2); Stage 3 (moderate renal insufficiency with eGFR of ⩾ 30–59 mL/min/1.73 m2); Stage 4 (severe renal insufficiency with eGFR of ⩾15–29 mL/min/1.73 m2); and Stage 5 (renal failure or end-stage renal disease [ESRD]) with eGFR of <15 mL/min/1.73 m2.
In accordance with the new American College of Cardiology/American Heart Association high blood pressure (BP) guidelines in the United States, 10 hypertension was defined as having at least stage 1 hypertension with systolic pressure between >130 mmHg and/or diastolic pressure >80 mmHg.
In accordance with the ‘Definitions of Terms of The Society of Thoracic Surgeons National Cardiac Surgery Database’, 11 an infection was considered present if (1) a wound was opened with excision of tissue (I&D), (2) there was a positive culture, or (3) the patient was treated with antibiotics. This included infections that were sternum-superficial (skin, subcutaneous tissue), sternum-deep (muscle, mediastinum, bone), leg (incision site), Intra-Aortic Balloon Pump (IABP) site, and septicaemia (requires positive blood cultures).
Statistical analysis
Continuous variables are expressed as mean ± standard deviation with categorical data as proportions (sample size). For continuous variables, comparisons between patients with and without diabetes were carried out using student’s t-test. Categorical variables were compared using χ2 analysis.
The association of the diabetes with adverse postoperative outcomes was then evaluated using logistic regression analysis. Significant patient characteristics, including diabetes and surgical risk factors, were added to the model, and non-significant covariates were removed from the multivariate analysis in a stepwise manner. All statistical analyses were performed using IBM SPSS v.22.0 (SPSS IBM, New York, USA); significance was judged at p = 0.05.
Results
Patient characteristics
Patients with diabetes undergoing cardiac surgery were significantly more obese [body mass index (BMI) 25.4 ± 4.2 vs 24.5 ± 4.0; p < 0.001], older (60.6 ± 9.0 years vs 58.3 ± 11.5 years; p < 0.001), hypertensive (88.5% vs 63.8%; p < 0.001), had renal impairment (16.9% vs 8.6%; p < 0.001), severely reduced left ventricular ejection fraction (11.0% vs 6.2%; p < 0.001) and a higher EuroSCORE (4.1 ± 5.7 vs 3.7 ± 5.1; p = 0.018) (Table 1). Expectedly, patients with diabetes also had higher preoperative glucose (8.7 vs 5.9 mmol/L, p < 0.001), HbA1c (7.6 vs 5.4%, p < 0.001), and peak intraoperative glucose level (8.8 vs 8.1 mmol/L, p < 0.001) (Table 1).
The overall prevalence of diabetes in our cohort was 46.7% (n = 1312 out of 2831) with prevalence varying among the different ethnic groups. Race was also significantly associated with diabetes (p < 0.001), with Indian and Malay ethnicity being associated with of the presence of diabetes, compared to Chinese ethnicity (Table 1).
Association of DM (Diabetes Mellitus) and outcomes
Compared to patients without diabetes, patients with diabetes tended to get postoperative hyperglycaemia (88.3% vs 56.0%; p < 0.001) and postoperative infection (2.8% vs 1.3%; p = 0.005) (Table 2).
Outcomes of patients with and without diabetes after cardiac surgery.
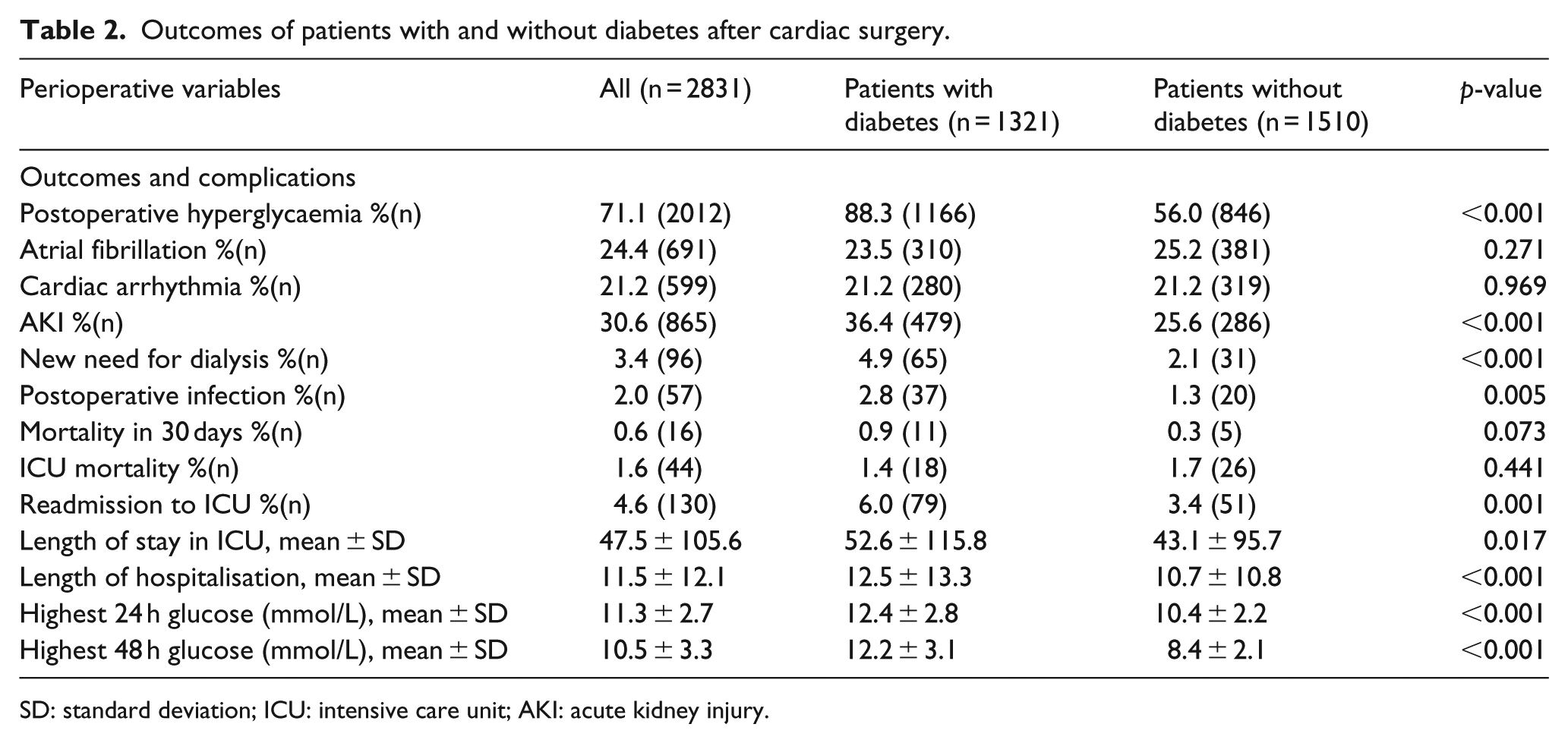
SD: standard deviation; ICU: intensive care unit; AKI: acute kidney injury.
Patients with diabetes also had poorer renal outcomes with diabetes being significantly associated with AKI (36.4% vs 25.6%; p < 0.001) and new need for dialysis (4.9% vs 2.1%; p < 0.001) (Table 2).
Diabetes patients also tended to have significantly higher rates of readmission to ICU (6.0% vs 3.4%; <0.001), longer stay in ICU (52.6 ± 115.8 days vs 43.1 ± 95.7 days; p = 0.017), and longer hospitalisation (12.5 ± 13.3 vs 10.7 ± 10.8; p < 0.001) (Table 2).
From multivariate analysis, diabetes mellitus was found to significantly increase the odds of ICU readmission by 1.70 (95% CI 1.171–2.480, p = 0.005), postoperative infection by 1.73 (95% CI 1.003–2.976, p = 0.049), AKI by 1.36 (95% CI 1.137–1.626, p = 0.001), postoperative hyperglycaemia by 6.00 (95% CI 4.893–7.348, p < 0.001), and the new need for dialysis by 1.71 (95% 1.086–5.360, p = 0.021) (Table 3).
Perioperative outcome variables significantly associated with diabetes mellitus after multivariable logistic regression analysis for each outcome.
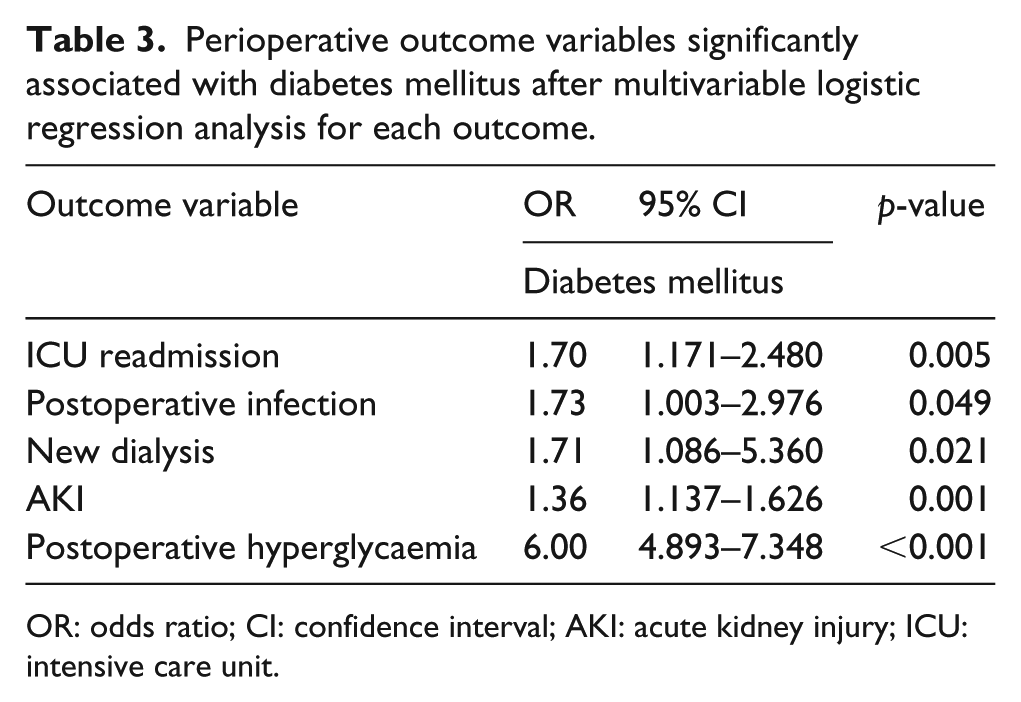
OR: odds ratio; CI: confidence interval; AKI: acute kidney injury; ICU: intensive care unit.
Subsequent subgroup analysis of patients with diabetes revealed that compared to those who were only on oral hypoglycaemic agents (OHGA), those who were on insulin regimes tended to be predisposed to poorer outcomes of postoperative hyperglycaemia (93.4% vs 87.0%, p < 0.001), AKI (49.0% vs 36.3%, p < 0.001), new need for dialysis (10.2% vs 3.7%, p < 0.001), ICU mortality (3.1% vs 0.9%, p = 0.006), and longer hospitalisation stay (15.3% vs 11.8%, p < 0.001) (Table 4).
Patient outcomes of diabetes patient treated with insulin versus those on OHGA only.
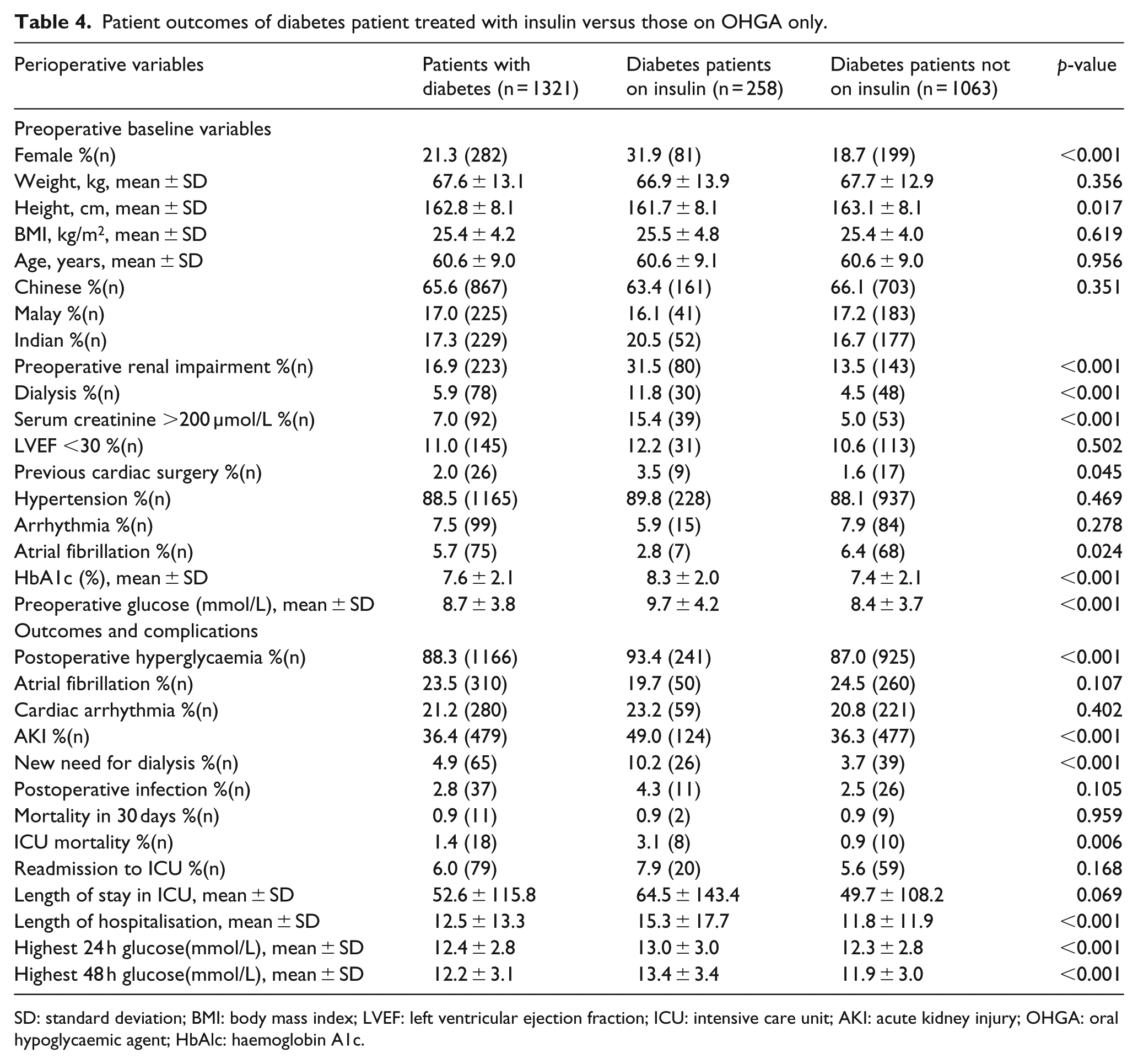
SD: standard deviation; BMI: body mass index; LVEF: left ventricular ejection fraction; ICU: intensive care unit; AKI: acute kidney injury; OHGA: oral hypoglycaemic agent; HbAlc: haemoglobin A1c.
Discussion
Overall prevalence of DM
The overall prevalence of DM in our Southeast Asian cohort undergoing cardiac surgery was 46.7%. This is significantly higher than that reported in Western populations (12%–38%), 12 supporting findings that Asia is the major site of a rapidly emerging diabetes epidemic. 13 This further validates the need of our study to determine whether diabetes is associated with poorer cardiac surgery outcomes among Southeast Asian patients.
Association of DM and poorer renal outcomes
Our findings show that diabetes patients were shown to be 1.36 times more likely than patients without diabetes to develop AKI. Previous studies have shown that diabetes patients are at increased risk of poorer renal outcomes, even after adjusting for numerous known risk factors, including chronic kidney disease. 14 Similar Western cohort studies have reported that surgical patients with diabetes were about 1.40 times more likely to have renal insufficiency and AKI after surgery as compared to those without diabetes,3,15 similar to our findings.
We also found that diabetes patients were over 1.71 times more likely to need new dialysis after surgery as compared to those without diabetes. The poorer renal outcomes (AKI, new need for dialysis) associated with diabetes are likely because patients with diabetes undergoing cardiac surgery have a greater inflammatory and oxidative stress response with significantly higher levels of cortisol, hsCRP, interleukin-6, and oxidative stress markers during the postoperative period, which is in turn associated with renal damage and poorer postoperative renal outcomes. 16
In a long-term prospective observational study of 4273 UK Prospective Diabetes Study (UKPDS), participants followed for a median of 18 years found similar results. 17 The study found that there were no differences in the rates of stroke or microvascular disease between the three ethnic groups in the study. This corroborates the findings in this study that the postoperative risk of developing complications among Asian diabetes patients is similar to that of Western diabetes patients, as compared to patients without diabetes.
Association of DM and postoperative infections and hyperglycaemia
We found patients with diabetes to be almost twice as likely to develop postoperative infections than those without diabetes.18,19 Similarly, other Western cohort studies have also found diabetes patients to be 2.03 more likely to develop postoperative infections, suggesting that patients with diabetes are twice as likely as those without diabetes to develop postoperative hyperglycaemia regardless of whether they are of Asian or Caucasian origin. Expectedly, the presence of diabetes is also strongly associated with the onset of postoperative hyperglycaemia (increasing its risk of onset by six times), which has been shown to lead to poorer outcomes in cardiac surgery patients. 20 Such post-surgical hyperglycaemia abolishes intrinsic myocardial protective mechanisms such as ischemic preconditioning 21 and causes both macrovascular and microvascular complications, as well as an increased risk of cardiovascular mortality. 22
Furthermore, this increased rate of postoperative hyperglycaemia in diabetes patients has been associated with deep sternal wound infections, further worsening prognosis and outcomes for diabetes patients undergoing cardiac surgery.6,23 This is because the hyperglycaemia among diabetes patients impairs their immune function and the inflammatory response which are critical for postoperative healing. 19
Association of DM and poorer hospitalisation outcomes
We also found diabetes patients to have a higher risk of being readmitted to the ICU compared to those without diabetes (OR 1.70, 95% CI 1.171–2.480, p = 0.005). Patients with diabetes also tended to have significantly longer ICU stay (52.6 vs 43.1, p = 0.017) and longer hospitalisation (12.5 vs 10.7, p < 0.001), likely due to the presence of complications and comorbidities associated with diabetes, increasing the cost of treatment and burden on healthcare.
Diabetes patients treated with insulin
Subsequent subgroup analysis of patients with diabetes revealed that compared to those who were only on oral hypoglycaemic agents (OHGAs), those who were on insulin tended to be predisposed to poorer outcomes of postoperative hyperglycaemia (93.4% vs 87.0%, p < 0.001), AKI (49.0% vs 36.3%, p < 0.001), new need for dialysis (10.2% vs 3.7%, p < 0.001), ICU mortality (3.1% vs 0.9%, p = 0.006), and longer hospitalisation stay (15.3% vs 11.8%, p < 0.001). Zarling et al. 24 also showed that patients on insulin therapy tended to be 1.89 times more likely to require Discharge to an Extended-Care Facility after surgery, corroborating our results that patients with diabetes who are on insulin therapy are more likely to have poorer outcome and more postoperative complications than their counterparts who have not been started on regular insulin regimes.
We postulate this is because requiring preoperative insulin treatment is a surrogate marker of poorer diabetes control and the presence of complications of diabetes. Patients with diabetes who were on insulin tended to have higher HbA1c (8.3% vs 7.4%, p < 0.001), higher preoperative glucose levels (9.7% vs 8.4%, p < 0.001), preoperative renal impairment (31.5% vs 13.5%, p < 0.001), serum creatinine >200 µmol/L (15.4% vs 5.0%, p < 0.001) and be on dialysis (11.8% vs 13.5%, p < 0.001) as compared to their counterparts with diabetes who were not on insulin. This is despite the fact that there was no significant difference between the subgroups in terms of baselines patient demographics such as weight, BMI, age, or ethnicity. Thus, it is clear that patients with diabetes who are on insulin therapy are likely to have more poorly controlled diabetes (and associated complications) and consequently worse outcomes after cardiac surgery than those not requiring insulin therapy (such as those only on OHGA).
Conclusion
In conclusion, diabetes is associated with increased risk for renal dysfunction, hyperglycaemia and infection after cardiac surgery as compared to patients without diabetes, to a similar extent to findings in Western populations. As such, patients with diabetes undergoing cardiac surgical interventions should receive special attention during the perioperative period to prevent the identified adverse effects, thereby improving postoperative outcomes of patients with diabetes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.