
Abstract
Admission hyperglycaemia is very common in acute ischaemic stroke (IS) patients and is associated with worse outcome in non-lacunar infarction, but its association with lacunar infarction remains controversial. We investigated the association between hyperglycaemia and clinical outcome in patients with acute lacunar stroke in a hospitalised Chinese population. Consecutive patients with acute IS were enrolled and classified into lacunar and non-lacunar stroke groups based on clinical criteria according to the Oxfordshire Community Stroke Project (OCSP) and findings on brain computed tomography (CT) or magnetic resonance imaging (MRI) scan. Hyperglycaemia was defined as blood glucose > 6.1 mmol/L. Univariate and multivariate analyses were used to examine the association between hyperglycaemia and outcomes in diabetic and non-diabetic groups. The main outcome measure was a poor outcome [defined as modified Rankin Scale (mRS) score ≥ 3] at 12 months after stroke. Of the 2020 acute ISs, 689 (34.1%) were acute lacunar strokes, of which 159 (23%) were diabetic and the other 530 (77%) were non-diabetic. In non-lacunar stroke, admission hyperglycaemia was independently associated with increased risk of poor outcome at 1 year (odds ratio (OR) = 1.782; 95% confidence interval (CI) = 1.340–2.370, p = 0.0005). In lacunar stroke, hyperglycaemia was not associated with functional outcome (OR = 1.337; 95% CI = 0.939–1.093, p = 0.086) irrespective of the diabetic status.
Introduction
Admission hyperglycaemia is very common in acute ischaemic stroke (IS) patients with a reported prevalence over 40%,1–4 irrespective of the time between stroke onset and glucose assessment or the conditions under which blood glucose levels are assessed, for example, random sampling versus fasting sampling (definition of hyperglycaemia used in these studies was blood glucose values of greater than 6.1–8 mmol/L). Many clinical trials have concluded that hyperglycaemia predicts a larger infarct size, poor clinical outcome and a higher risk of mortality independent of age, diabetic status, stroke severity or stroke type.2,5–9
However, a systematic review and meta-analysis 10 suggest that the administration of intravenous insulin to patients within the first hours of IS in an attempt to maintain serum glucose within a specific normal range is not beneficial in terms of patient functional outcome, death at 30 days or 90 days or improvement in final neurological deficit. However, it is therefore still unknown whether and to what degree hyperglycaemia should be treated.
The relationship between hyperglycaemia and stroke outcome seems to differ between diabetic and non-diabetic patients. One report shows a threefold higher 30-day mortality only in non-diabetic hyperglycaemic IS patients. 2 Two studies11,12 have shown no relationship between high blood glucose levels and short-term mortality in IS patients with diabetes mellitus (DM). In addition, the association between hyperglycaemia and IS seems to differ between lacunar and non-lacunar subtypes. Lacunar infarcts are small subcortical infarcts that result from occlusion of a single penetrating artery. 13 Admission hyperglycaemia has been clearly demonstrated as a risk factor for non-lacunar infarction, especially in patients treated with thrombolysis. 14 However, the relationship between hyperglycaemia and lacunar infarction remains controversial. Weir et al. 5 suggested the detrimental effect of hyperglycaemia on lacunar stroke, while trials by Bruno et al.15,16 and Uyttenboogaart et al. 17 indicated that hyperglycaemia might be protective in lacunar stroke.
The aim of this study was to investigate the impact of hyperglycaemia on the prognosis of lacunar strokes at 1 year after stroke onset in a Chinese hospital-based study.
Subjects and methods
We included first-ever IS patients admitted consecutively to neurological wards of the West China Hospital, Sichuan University within 24 h of symptom onset between 1 September 2002 and 30 August 2010. The diagnosis of IS was based on clinical presentation and computed tomography (CT) or magnetic resonance imaging (MRI) scan. Patients with transient ischaemic attack or prior functional dependency [modified Rankin Scale (mRS) ≥ 3] were excluded. IS cases were classified into lacunar infarction and non-lacunar infarction subgroups according to the Trial of ORG 10172 in Acute Stroke Treatment (TOAST) classification criteria. 18 Lacunar infarction was defined as an infraction presenting the following features: pure motor stroke, pure sensory stroke, sensorimotor stroke, ataxic hemiparesis and dysarthria-clumsy hand syndrome in conjunction with a CT or MRI that could account for neurological deficits. Lacunes were defined as well-delineated areas of 2–15 mm of signal change with the same characteristics as cerebrospinal fluid on T1- and T2-weighted MRI. Lesions with these signal or hypodensity characteristics smaller than 2 mm were considered as perivascular space dilatations. Patients exhibiting clinical signs that could not be explained by the lacunar infarction were excluded from this study. This research project was approved by the Scientific Research Department of West China Hospital.
Baseline information was collected from patients upon admission, including age, sex, initial stroke severity, risk factors (hypertension, DM, hyperlipidaemia, current smoking, alcohol assumption), admission blood serum glucose (blood glucose > 6.1 mmol/L was defined as hyperglycaemia 3 ) and neuroimaging findings. The patients with hypertension were identified either from a previous diagnosis, current antihypertensive treatment or blood pressure > 140/90 mmHg on at least two measurements at different time points. Diabetes was defined by a previous diagnosis of diabetes or the use of antidiabetic agents by patients. Hypercholesterolaemia was defined by a previous diagnosis, lipid-lowering therapy or blood cholesterol > 5.72 mmol/L. 19 The patients who smoked tobacco products at least 6 months at the time of their events were defined as current smokers. The patients who drank almost every day, the average amount of daily drinking being more than 30 g, for more than 1 year were defined as current drinkers. 20 Severity of stroke was assessed using the National Institutes of Health Stroke Scale (NIHSS). The NIHSS score was graded as follows: mild (0–6), medium (7–15) and severe (≥16). 21 We used the mRS to assess the functional outcome of these patients at 1 year after stroke onset by telephone interview or letter. Unfavourable outcome in terms of dependency or death was defined using the mRS score ≥ 3. 22 Cause of death was determined via questionnaires taken by telephone interview or letter. A detailed study design and methods have been previously published. 23
Continuous data are presented as the mean ± standard deviation (SD) or median and interquartile range (IQR) (25th to 75th percentile) in the case of non-normal distributions. Discrete data are given as counts and percentages. For univariate analyses, Mann–Whitney U or chi-squared tests were used, where appropriate.
Variables such as age, gender, stroke severity (NIHSS), hypertension, hyperlipidaemia, diabetes, alcohol and smoking are possible confounders of the predictors. Variables that were identified as significant in the univariate analyses (p < 0.05) were entered into logistic regression analyses to determine the association between hyperglycaemia and patient outcomes.
SPSS version 18.0 was used for statistical analyses. Statistical significance was defined as a (two-sided) p value < 0.05.
Results
Of the 2020 cases of IS, 689 (34%) cases were classified as having lacunar infarction. Table 1 summarises the baseline characteristics of the patients.
Baseline characteristics at admission.
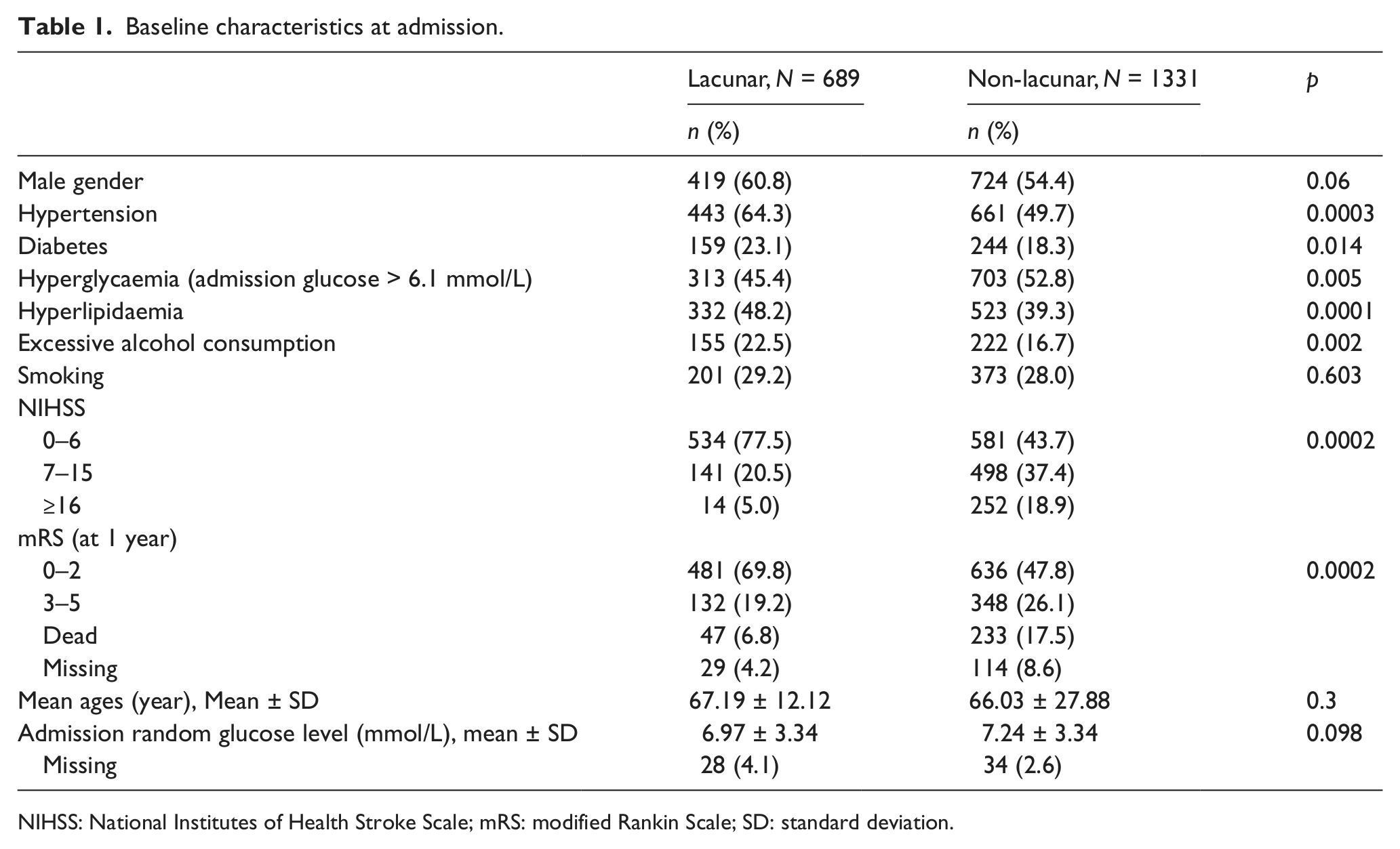
NIHSS: National Institutes of Health Stroke Scale; mRS: modified Rankin Scale; SD: standard deviation.
There were 28 (4.1%) missing glucose values in the lacunar group and 34 (2.6%) in the non-lacunar group. At 1 year, 29 (4.2%) and 114 (8.6%) mRS scores were missing in the lacunar and non-lacunar group, respectively.
In lacunar strokes, a total of 313 patients (47.4%) had blood glucose > 6.1 mmol/L on admission; 159 (23.1%) patients had a prior diagnosis of diabetes. We classified lacunar patients into diabetic and non-diabetic groups based on the prior diagnosis of diabetic status.
The univariate analysis showed that hyperglycaemia did not predict poor outcome in lacunar stroke (odds ratio (OR) = 1.337; 95% confidence interval (CI) = 0.939–1.093) (Table 2), while in non-lacunar stroke, both univariate and multivariate analyses (Tables 2 and 4) showed that hyperglycaemia, defined as blood glucose > 6.1 mmol/L, independently increased the chance of an unfavourable outcome (OR = 1.782; 95% CI = 1.340–2.370, p = 0.0005).
Univariate analysis of lacunar and non-lacunar patients.
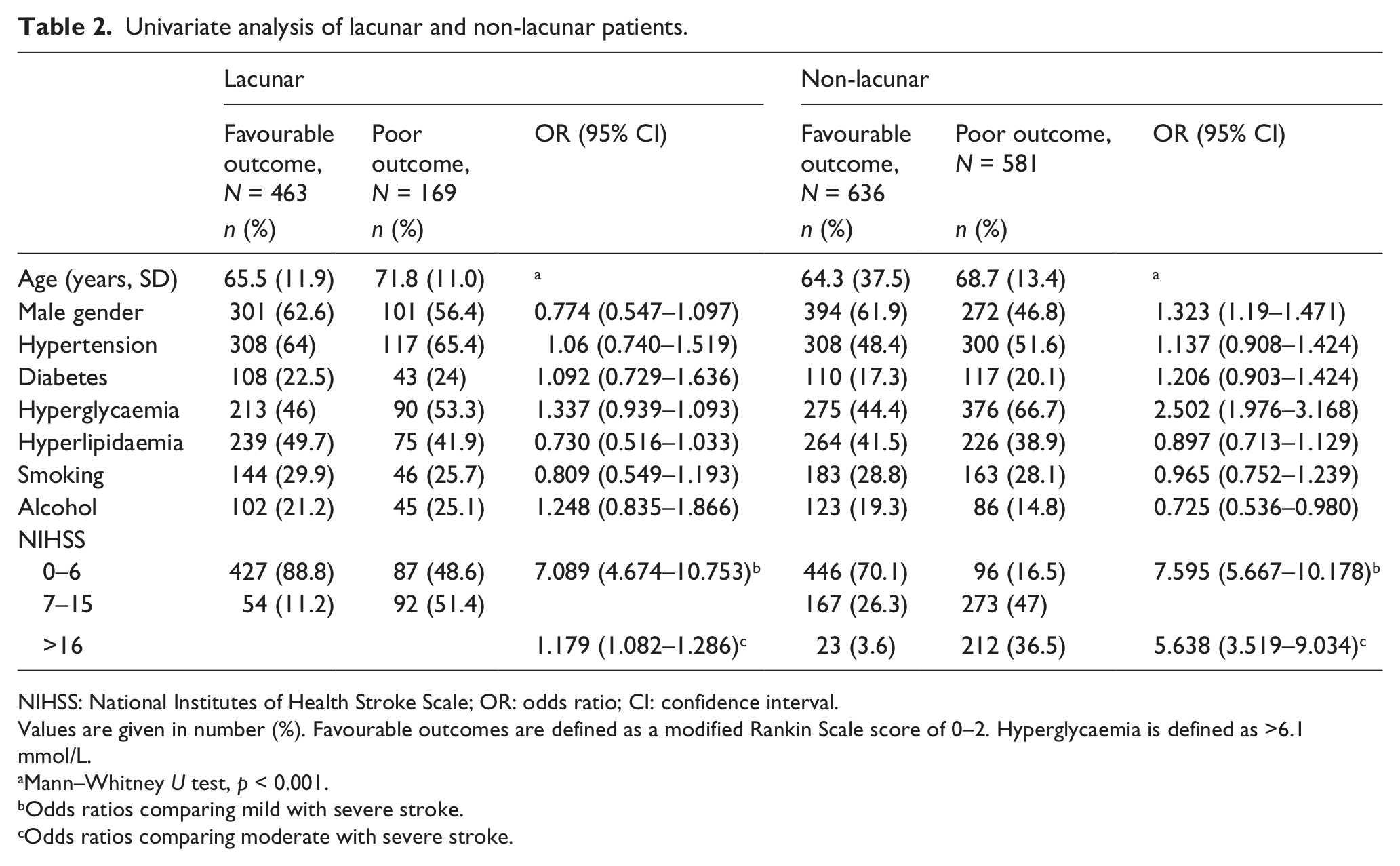
NIHSS: National Institutes of Health Stroke Scale; OR: odds ratio; CI: confidence interval.
Values are given in number (%). Favourable outcomes are defined as a modified Rankin Scale score of 0–2. Hyperglycaemia is defined as >6.1 mmol/L.
Mann–Whitney U test, p < 0.001.
Odds ratios comparing mild with severe stroke.
Odds ratios comparing moderate with severe stroke.
We further investigated the relationship between diabetic and non-diabetic lacunar stroke and clinical outcome. The results of the subgroup analysis of lacunar stroke are presented in Table 3. In a univariate analysis, the association of hyperglycaemia was significant only in those patients without a prior diagnosis of DM (p = 0.033), but in the diabetic subgroup, there was no statistically significant association (p = 0.618). Hyperglycaemia was not associated with outcome in non-diabetic patients with lacunar stroke (p = 0.925), after adjusting for age and severity of stroke in multivariate analysis (Table 4).
Univariate analysis of variables associated with functional outcome at 1 year in lacunar stroke (mRS ≥ 3).
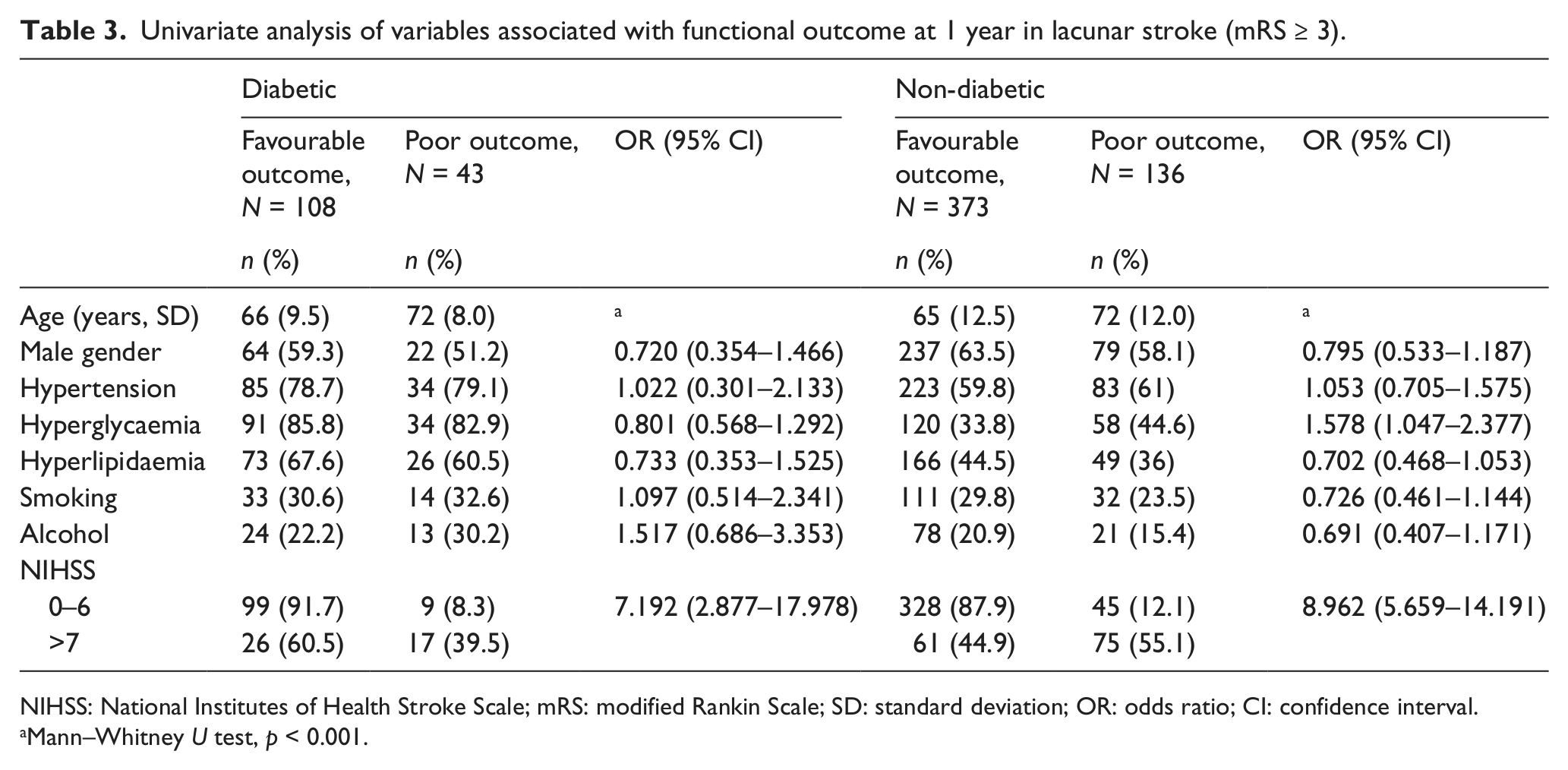
NIHSS: National Institutes of Health Stroke Scale; mRS: modified Rankin Scale; SD: standard deviation; OR: odds ratio; CI: confidence interval.
Mann–Whitney U test, p < 0.001.
Multivariate analysis of non-lacunar and non-diabetic lacunar patients’ poor outcome at 1 year (mRS ≥ 3).
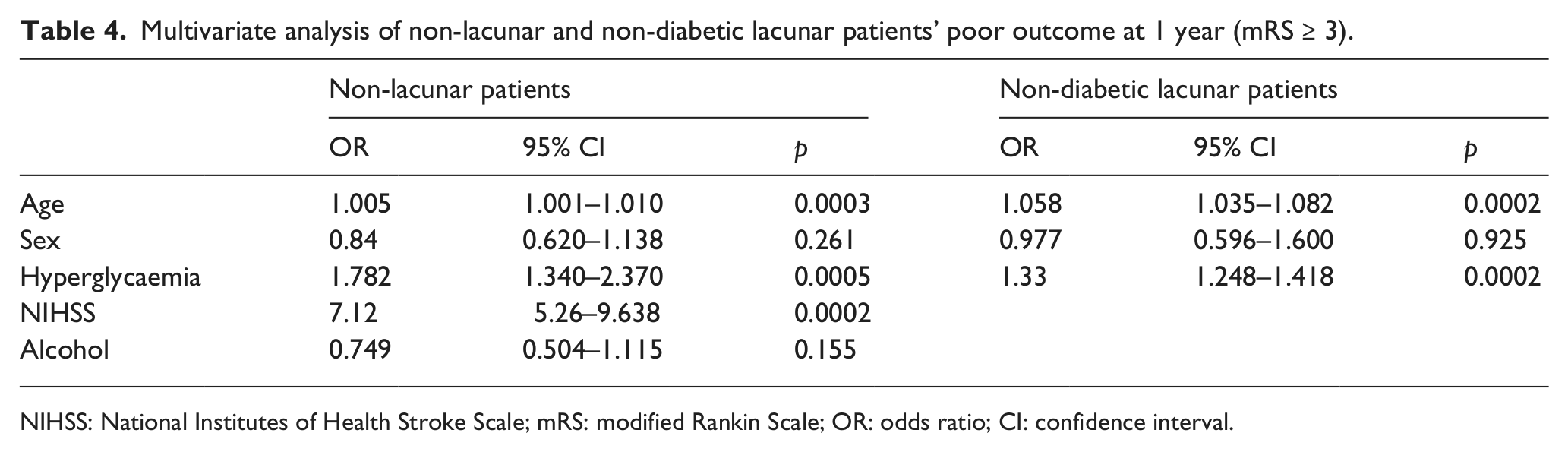
NIHSS: National Institutes of Health Stroke Scale; mRS: modified Rankin Scale; OR: odds ratio; CI: confidence interval.
Discussion
To our knowledge, this study is the largest hospital-based study to evaluate the relevance of hyperglycaemia and lacunar stroke. Our data suggest that after acute lacunar stroke, admission hyperglycaemia has no relationship with adverse clinical outcomes with the poor outcome. In lacunar patients, we performed further analysis for patients with or without diabetes. In non-diabetic patients, admission hyperglycaemia was associated with poor outcome in a univariate analysis but was not confirmed after adjusting for age and severity of stroke using logistic regression analysis. The results were consistent with Bellolio et al.’s study 24 but different from two other studies.15,17 However, each of these studies had fewer patients than our study and neither was statistically powered to detect the effects of hyperglycaemia. One explanation is that most patients presented with relatively mild stroke events [median NIHSS score, 4 (IQR = 1–6)], with a high functional recovery (69.8%) and limited mortality. In addition, our results with regards to non-lacunar stroke are consistent with previous investigations in IS, which demonstrate that admission hyperglycaemia is independently associated with the poor outcome. Our definition of post-stroke hyperglycaemia differs from prior studies; however, we have attempted to maintain consistency with the systematic review, 10 though the use of any cut-off threshold to define hyperglycaemia is arbitrary. In this study, a single measure of blood glucose was used at the time of admission. This is a relatively crude measure and likely to underestimate true incidence of hyperglycaemia. Nevertheless, at least 60% of the previous studies that demonstrated a relation between stroke outcome and glucose level relied on a single glucose measurement. 2 Several mechanisms have been proposed to account for hyperglycaemia after stroke. Hyperglycaemia might be due to a stress response, a measure of unrecognised insulin resistance or DM. Various studies have shown that a substantial proportion of IS patients without a previous history of diabetes appear to have insulin resistance or DM at follow-up.1,25,26 Admission plasma glucose > 6.1 mmol/L predicted the presence of previously unrecognised DM at 12 weeks with a high predictive value.1,26 Lack of HbA1c test and oral glucose tolerance test (OGTT) to define pre-existing glycaemic status is a limitation of this study.
The mechanism of the effects of hyperglycaemia on lacunar stroke is not yet known. Experiments have also found that the effect of ischaemia was not different between normoglycaemic and hyperglycaemic animals with end-artery infarcts,27,28 suggesting that it was related to ischaemia and reperfusion rather than to hyperglycaemia. However, in subcortical strokes, the magnetic resonance spectroscopy also provided evidence of metabolically compromised area. 29
This study is a single-centre study conducted in China, so the results can only suggest a correlation among people of Asian descent and cannot be generalised to the general population. Among our patients, 34% with IS are in the lacunar group, which is higher than in other studies.30,31 This high proportion may be due to a higher lacunar infarction rate among Asian people or it may indicate that the clinical distinction between lacunar and non-lacunar infarction was less accurate than in other studies. 32 Most of the lacunar stroke infarcts are asymptomatic, and our study included only acute lacunar strokes with symptoms. Lacunar infarcts are small subcortical strokes that, in most cases, result from occlusion of a single penetrating artery, classically located in the basal ganglia, internal capsule, thalamus or brainstem, with a size ranging from 3 to 15 mm in diameter. 13 There are a variety of different classification methods to define IS subtypes, such as Oxfordshire Community Stroke Project (OCSP) 33 and TOAST 18 classification, and TOAST classification is the standard classification system for clinical definition of ISs. This proportion could be reduced in future studies by the more frequent use of advanced MRI such as diffusion-weighted imaging (DWI) and perfusion-weighted imaging (PWI) in an early stage, especially when the CT scan does not show a relevant infarct. 34
And beyond survival and functional impairment, cognitive impairment following stroke has been recognised as an important outcome in patients with stroke. Lacunar infarct is the most common stroke subtype that predisposes patients to vascular dementia.35,36 One study reported that hyperglycaemia was not associated with impaired cognition after 6–10 months in lacunar stroke, 37 though this study had limitations including small sample size and short follow-up duration.
In the absence of evidence supporting tight glycaemic control in stroke patients and because of the increased risk of hypoglycaemia, the American Heart Association, American Diabetes Association and European Stroke Organization all currently recommend initiating treatment in patients with a blood glucose level > 7.8–10 mmol/L.38–40 It is unclear whether hyperglycaemia should be treated actively in the acute phase of lacunar stroke. Our findings may have important implications for the treatment of hyperglycaemia in acute lacunar stroke and related clinical trials. From these results, we can conclude that it is important to define the stroke type and the diabetic status in patients because the aggressive treatment of hyperglycaemia may not be necessary in cases of lacunar infarction, especially for diabetic patients. Future studies investigating the association of hyperglycaemia and long-term cognitive outcome in patients with lacunar strokes are needed.
Footnotes
Conflict of interest
The authors report no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.