
Abstract
Background:
Forefoot gangrene in patients with diabetes is a severe form of foot ulcers with risk of progress and major amputation. No large cohort studies have examined clinical characteristics and outcome of forefoot gangrene in patients with diabetes. The aim was to examine clinical characteristics and outcome of forefoot gangrene in patients with diabetes admitted to a diabetic foot centre.
Methods:
Patients with diabetes and foot ulcer consecutively presenting were included if they had forefoot gangrene (Wagner grade 4) at initial visit or developed forefoot gangrene during follow-up at diabetic foot centre. Patients were prospectively followed up until final outcome, either healing or death. The median follow-up period until healing was 41 (3–234) weeks.
Results:
Four hundred and seventy-six patients were included. The median age was 73 (35–95) years and 63% were males. Of the patients, 82% had cardiovascular disease and 16% had diabetic nephropathy. Vascular intervention was performed in 64%. Fifty-one patients (17% of surviving patients) healed after auto-amputation, 150 after minor amputation (48% of surviving patients), 103 had major amputation (33% of surviving patients) and 162 patients deceased unhealed. Ten patients were lost at follow-up. The median time to healing for all surviving patients was 41 (3–234) weeks; for auto-amputated, 48 (10–228) weeks; for minor amputated, 48 (6–234) weeks; and for major amputation, 32 (3–116) weeks.
Conclusion:
Healing without major amputation is possible in a large proportion of patients with diabetes and forefoot gangrene, despite these patients being elderly and with extensive co-morbidity.
Keywords
Introduction
Diabetes mellitus is a fast-growing health challenge; it is estimated that worldwide 700 million adults will have diabetes by 2045. 1 Diabetic foot ulcers (DFUs) are a major complication of diabetes mellitus with a risk for amputation.2,3 The incidence of vascular lower limb amputation at or proximal to the trans-metatarsal level has been shown to be eight times higher in diabetic individuals than nondiabetic individuals ⩾45 years of age. 4
Forefoot gangrene in patients with diabetes is a severe form of DFU. 5 The reasons for the development of gangrene have been disputed, but reduced peripheral circulation, inflammation and infection have been suggested.6,7 In general, the most significant predictors of outcome of DFU are peripheral arterial disease (PAD), infection and co-morbidities.2,6,8–10 The possible outcomes of forefoot gangrene include healing after auto-amputation, healing after minor amputation with a loss of varying part of the forefoot, major amputation or death without healing.2,6,10
Many studies have examined patients with diabetes and forefoot gangrene,11–14 but they only included small number of patients. There are no large cohort studies that have examined the clinical patient characteristics and, consequently, the outcome for forefoot gangrene. This study aimed to examine the clinical characteristics, outcome and factors related to the outcome of forefoot gangrene in patients with diabetes who were consecutively admitted to a diabetic foot centre.
Materials and methods
Study design
In this cohort study, a retrospective evaluation was done of patients with diabetes and forefoot gangrene at first visit or who developed forefoot gangrene during follow-up. Patients were followed up at diabetic foot centre prospectively until the outcome.
Setting
The study was conducted at a multidisciplinary diabetic foot centre located in a university hospital, with a primary catchment area of approximately 600,000 people. The management was based on a pre-set standardised protocol,6,15 which registered demographic information, concomitant diseases, diabetes treatment, ulcer-specific data (Wagner grade, infection, local treatments, vascular and orthopaedic surgery) and outcome. Physical examination was performed at the time of inclusion, and it was regularly repeated during the study by the same multidisciplinary team. The core team consisted of a diabetologist, orthopaedic surgeon, an orthotist, a podiatrist and a registered nurse educated in diabetes. A vascular surgeon was integrated into the team on a regular basis. Out-patient treatment was carried out in collaboration with primary healthcare and home nursing services. The participants were consecutively included between 1 January 2000 and 31 December 2012, then followed up and treated by the team at the hospital until healing was achieved or death occurred unhealed. The study was approved by the Regional Ethical Review Board in Southern Sweden (No. 120/2007). No signed consent was required. Patients were informed of the study and that they could decline participation at any time.
Patient population
All the patients referred to the diabetic foot centre (n = 5010) presenting with DFUs (n = 7214) were consecutively assessed, treated and followed until final outcome. The following inclusion criteria were applied: ⩾18 years of age, diabetes and gangrene (Wagner grade 4) 16 at first visit or if developed during the treatment time, located on the forefoot (digits or metatarsal heads). In this study, 476 patients with gangrene on the toes and/or forefoot were followed (Figure 1). Each participant is represented with one foot having the worst DFU outcome.
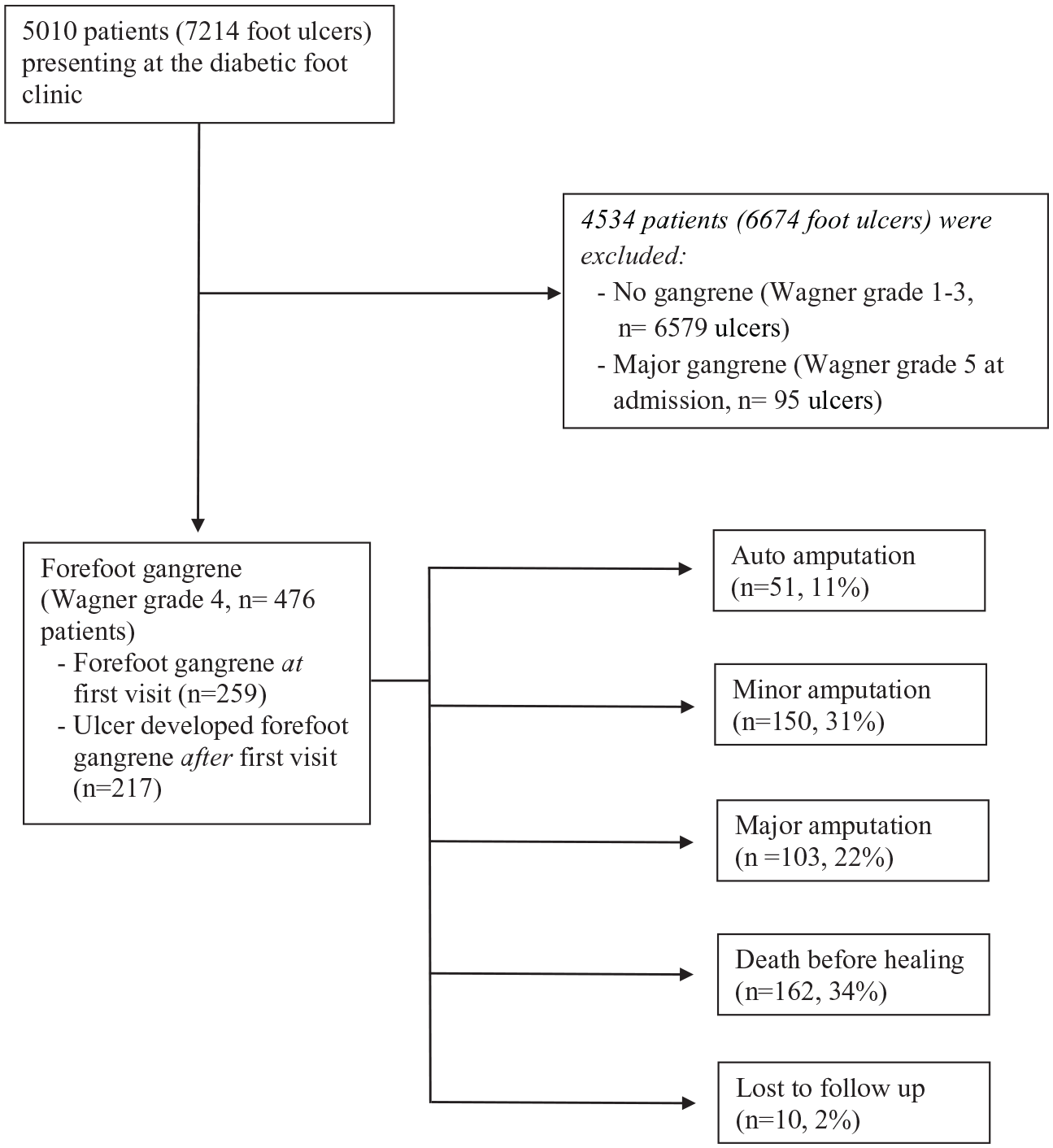
Flow chart and outcome.
Forefoot was defined as the distal part of the foot that is composed of the metatarsal bones, the phalanges and associated soft tissue structures. 17 Gangrene was defined as a continuous necrosis of the skin and underlying structures (muscle, tendon, joint or bone), indicating irreversible damage and fulfilling Fontaine grade 4, that would be unlikely to heal without loss of some part of the extremity (Wagner grade 4).16,18 Healing was defined as intact skin with complete epithelialisation without any exudation of a previous foot ulcer site. 17
Treatment procedure
Entry data were collected on patient characteristics, co-morbidities, previous management, ulcer characteristics and laboratory findings. Diabetic kidney disease was defined as the need for ongoing dialysis or renal transplantation or persistent urine albumin ⩾300 mg/L. 19 Glycated haemoglobin (HbA1c) was measured using Mono-S or later as IFCC (International Federation of Clinical Chemistry and Laboratory Medicine) values. The HbA1c values measured as Mono-S were converted to IFCC using the following formula: IFCC = 10.45 × Mono-S − 10.62 20 (Supplementary Information).
The participants were treated as outpatients, but in the case of vascular surgery, deep infection associated with septic condition, foot surgery, amputations or exacerbation of inter-current disease, they were treated as in-patients under the supervision of the multidisciplinary diabetic foot team.2,6,15,21,22 Topical treatments were prescribed in a written form by the team, and dressing changes were performed under the supervision of a registered nurse in primary healthcare centres or home nursing services. Individually adjusted off-loading equipment was offered to all the participants.
Systolic toe and ankle pressure were measured using strain gauge and Doppler techniques (Supplementary Information).
Angiography was performed at the discretion of the vascular surgeon according to a written programme that was jointly agreed upon in advance. 2 The exclusion criteria for angiography were: medical condition not allowing angiography, gangrene Wagner grade 5, life expectancy less than 6 months, lack of walking ability before occurrence of gangrene or informed consent for angioplasty refused. 2
Revascularisation was performed at the discretion of the vascular surgeon in 306 participants, via either endovascular intervention (n = 246) or reconstructive surgery (n = 60). The remaining 170 participants had no vascular surgery: 116 participants due to their medical condition (not feasible; general health condition did not permit surgery or acute amputation due to deep infection), 43 participants had no severe PAD and 11 participants did not give consent for revascularisation. Furthermore, vascular surgery prior to referral had been performed on 14 participants ipsilaterally, 9 participants with percutaneous transluminal angioplasty (PTA) and 5 with reconstruction; and on 21 participants contralaterally, 16 participants with PTA and 5 with reconstruction. Local surgical debridement was performed when required. Dry and inactive necrosis or toe gangrene with or without an underlying osteomyelitis was left to mummify if pain, progression of gangrene and infection would allow. 22 Acute incision and drainage was performed in case of a deep abscess or necrotising tendonitis/fasciitis. The decision to amputate was made at the discretion of the orthopaedic surgeon based on the following criteria: progressive gangrene, septic condition and rest pain not improved by or not available for revascularisation. In most of the cases, there were multiple indications for amputation. 23 A non-healing ulcer was not necessarily considered to be an indication for amputation. The level of amputation was chosen based on clinical assessment at the most distal level where healing could be anticipated; the minimal requirements for this were intact skin and no local signs of infection or severe ischaemia. 23 Participants were followed up until healing was achieved or till the patient’s death.
Statistical analysis
Descriptive statistics are given as median and range. The Chi-square test and Mann–Whitney U-test were used to compare the variables in relation to the outcome and to compare the duration of healing time between the participants who healed after auto-amputation and those who had healed after a minor amputation. The simultaneous influence of possible risk factors on a binary outcome (either minor or auto-amputation versus major amputation or deceased unhealed) was investigated using backward logistic regression analysis. Statistical significance was defined as a p-value <0.05. Statistical analysis was performed using SPSS Version 20 (SPSS, Chicago, IL, USA).
Results
A total of 476 participants were included in the study. The median age was 73 (range, 35–95) years and 62% of the participants were male. The demographic data of the participants are presented in Table 1. Median toe pressure was 35 (0–180) mmHg and median ankle pressure was 80 (0–197) mmHg; 36% of the participants had more than one ulcer on the same foot and 68% had rest pain (Table 2).
General characteristics of patients at inclusion in relation to outcome.

pı: auto-amputation versus minor amputation; p²: major amputation versus minor amputation; NS: not significant; HbA1c: glycated haemoglobin in millimoles per mole (mmol/mol).
Values are number (%) or median (range).
Local characteristics on the foot.

pı: auto-amputation versus minor amputation; p²: major amputation versus minor amputation; NS: not significant.
Values are n (%) or median (range). Toe and ankle pressure are measured in millimetres of mercury (mmHg).
There was no difference in the outcome between the participants presenting with gangrene at inclusion compared to those who developed gangrene during follow-up (data not shown). The participants who developed gangrene after the first visit to the clinic were more often male, more often had a single ulcer (p = 0.000), infection in the foot (p = 0.001) and rest pain (p = 0.001) than the participants who presented with gangrene at the first visit. A separate analysis was made of the participants included from 1 January 2000 to 30 June 2006 versus 1 July 2006 to 31 December 2012 to reveal any effects from potential improved treatments, but no differences in outcome were detected.
Of the 476 participants, 51 (17% of the surviving participants, 11% of all participants) were healed after auto-amputation, 150 were healed after a minor amputation (49% of surviving participants, 31% of all participants), 103 had a major amputation (34% of surviving participants, 22% of all participants) and 162 died unhealed (34% of all participants). Ten participants were lost to follow-up (2% of all participants) (Figure 1).
Factors related to outcome with regard to final amputation level
The participants who healed after auto-amputation had more often undergone vascular surgery than those who healed after a minor amputation. A majority of the auto-amputated participants had diabetes type 2 (92%); they were less often treated with insulin at inclusion, less often had diabetic kidney disease and less often had rest pain in comparison to the other groups. The participants who healed after a minor amputation more often had a deep foot infection than the participants who healed after auto-amputation. Most of the participants who had major amputation were male; moreover, they more often had cardiovascular disease, multiple ulcers and rest pain than participants who healed after minor amputation or auto-amputation. The participants who died unhealed were older, had more cardiovascular disease and diabetic kidney disease and had undergone vascular surgery less often than surviving participants (Table 1).
A multiple regression analysis was performed to identify the participant or ulcer-related factors, including age, gender, ankle pressure, performance of vascular intervention, presence of peripheral oedema, rest pain, retinopathy, diabetic kidney disease, cardiovascular disease and multiple ulcers by comparing healing after auto-amputation or minor amputation versus major amputation or died unhealed. The following factors were found to affect the outcome: older age, presence of diabetic kidney disease, cardiovascular disease and more than one ulcer in the same foot (Table 3).
Factors related to outcome of forefoot gangrene (major amputation or death unhealed).

OR: odds ratio; CI: confidence interval.
Time to wound healing in relation to outcome
The median time to healing for all the surviving participants was 41 (3–234) weeks; for auto-amputated participants it was 48 (10–228) weeks and for minor amputated participants it was 48 (6–234) weeks. There was no statistically significant difference between the two groups (p = 0.382). For the participants with major amputation, the time to healing was 29 (3–116) weeks.
Discussion
In this study of 476 consecutively presenting individuals with diabetes and a forefoot gangrene, 42% of all the participants healed after either auto-amputation of toes or minor surgical amputation, 22% had major surgical amputations and 34% died unhealed. In the surviving participants who continued follow-up until the final outcome, healing below the ankle was achieved in 66% of the participants. To the best of our knowledge, this outcome has not previously been reported in a large cohort study of consecutively presenting individuals with diabetes and a forefoot gangrene.
In this study, 17% of the surviving participants with forefoot gangrene healed with an auto-amputation when managed by a multidisciplinary foot team in collaboration with primary healthcare centres and home nursing services. An auto-amputation is considered less traumatic to patients than a surgical amputation, as it enables patients to avoid a hospital stay and provides less tissue loss. Minor auto-amputation or minor surgical amputation preserves the ankle joint and limb length, thus maintaining a significant part of limb function. Well-healed DFUs after minor amputation allows for better function over time, provided the patient has sufficient arterial blood flow to the foot and successful offloading and rehabilitation. 24
It has been argued that a long healing time for auto-amputation will lead to increased suffering and pain. 21 However, in this study, the healing time was not significantly shorter for the participants who underwent minor surgical amputation.
There is some controversy concerning the benefit of a primary minor amputation versus primary major amputation below the knee.23,25,26 In this study, 52% of all the participants and 64% of the surviving patients healed below the ankle either with auto-amputation or a minor surgical amputation. In studies with DFUs of mixed cohorts, the reported healing rates for minor amputation levels range from 2.4% to 34%.27–29 These variations can be explained by differences in patient selection, definitions and length of follow-up. There is no randomised controlled study regarding amputation level selection in DFUs and particularly in the presence of gangrene. The basic consideration is to choose the lowest amputation level where healing is deemed possible.
The median healing time from inclusion was longer in our study in comparison to other studies.2,27–30 This may be explained by the type of foot ulcer in the included patients; they all had ischemic gangrene, Wagner grade 4 and no superficial non-ischemic ulcers. Healing time is often not uniformly defined in studies examining DFUs. It is essential to mention that there was no specific time set for follow-up. The reported healing time is determined from the day the patient is first seen at our clinic until the day the ulcer is healed; the healing time is not based on the length of time from amputation to healing. Furthermore, assessing healing time in studies that included patients with DFUs and comparing results in this regard to other studies are often difficult and complex. 31
Interestingly, the participants who had auto-amputation less often had insulin treatment in comparison to those who healed after a minor amputation. One possible explanation for this is that the lower need for insulin treatment indicates better glycaemic control in this group of participants; consequently, this may imply a lower risk for foot infection. The latter is a known major indication for surgical amputation. 32 This explanation is supported by the observation that the median HbA1c value was lower in the participants with auto-amputation in comparison to those with minor amputation. Moreover, deep infection was seen in 61% of the participants with auto-amputation in comparison to 77% in those with minor amputation.
Despite the health and economic burden caused by lower limb amputations, both minor and major, major surgical amputation results in higher costs per patient and annual expenditures, including post-operative care. 33 Healing after minor amputation was not associated with a negative impact on health-related quality of life in patients with DFUs in comparison with healing after conservative treatment. 25 Furthermore, it has been shown that patients with diabetes who undergo major amputation are older with a high incidence of co-morbidity. Major amputation in these patients implies a significant impact on their functional capacity and considerable risk for mortality.34,35
In this study, multiple regression analysis showed that older age, presence of co-morbidity (cardiovascular and diabetic kidney disease) and having more than one ulcer in the same foot were related to a lower probability of an ulcer healing below the ankle. The presence of foot ulcers in patients with diabetes has been associated with underlying multi-organ disease.2,19,36 Patients with PAD and diabetes have also been shown to more frequently have chronic renal disease and a history of myocardial infarction in comparison to those without diabetes. 37 Kidney disease is known to be associated with worse outcome in patients with diabetic foot problems.38–40 Approximately 50% of diabetic patients with PAD have been shown to simultaneously have coronary artery disease and/or cerebrovascular disease. 41 In fact, coexistence of PAD and coronary artery disease in patients with DFUs might be more common. Londahl et al. 42 have reported that signs of cardiac muscle dysfunction were present in 76% of diabetic patients with a chronic foot ulcer without a previous history of heart disease. Furthermore, coronary artery disease has been shown to be the leading cause of death in patients with diabetes and PAD. 43
Uccioli et al. 44 found that age predicts major amputation in patients with diabetes undergoing endovascular angioplasty. Similarly, previously, we showed that older age predicts non-primary healing in patients with diabetes and an ischemic foot ulcer. 2
This study was limited to a cohort of consecutive patients presenting at a multidisciplinary foot clinic at a university hospital, followed to healing or death. One of its strengths is that over 350 amputations were included, and all but 10 were followed until healing or death. Because the patients included in this study had Wagner grade 4 with gangrene in the forefoot, and no exceptions were made with regard to age, co-morbidity or expected survival, it is unlikely, yet still possible that the foot team was unaware whether patients with diabetes and forefoot gangrene from the same catchment area were treated in primary healthcare centres or other units. Definitions of outcome in patients with diabetes and foot ulcers can be very complex, which is an issue that has been previously analysed. 45 The purpose of this study was to compare amputation below and above the ankle as an outcome; therefore, we divided outcomes into four groups: minor auto-amputation, minor surgical amputation, major amputation or death unhealed. Primary healing was not considered to be an outcome because all the patients had gangrene. Another limitation of the study is that no power calculation was done for estimation of sample size selected for the study, with exception to include 500 participants with forefoot gangrene based on experience from previous studies in this cohort study. The study recruitment was stopped due to the introduction of new treatment technologies with regard to medical or surgical treatment. It is worth mentioning that some risk factors that may affect outcome, such as foot infection, 32 were not included in our logistic regression analysis due to the limitation of data availability.
Conclusion
This study has shown that healing without major amputation is possible in patients with diabetes and forefoot gangrene, and it supports the use of minor amputation in these patients to avoid major amputation. However, using minor amputation to achieve healing below the ankle results in longer healing times and the risk of repeated surgical interventions in a vulnerable patient group. Old age, co-morbidity and presence of multiple ulcers negatively affected the outcome.
Supplemental Material
sj-pdf-1-smo-10.1177_20503121211029180 – Supplemental material for Healing below the ankle is possible in patients with diabetes mellitus and a forefoot gangrene
Supplemental material, sj-pdf-1-smo-10.1177_20503121211029180 for Healing below the ankle is possible in patients with diabetes mellitus and a forefoot gangrene by Targ Elgzyri, Jan Apelqvist, Eero Lindholm, Hedvig Örneholm and Magdalena Annersten Gershater in SAGE Open Medicine
Footnotes
Acknowledgements
The authors express their gratitude to M.-B. Johansson, I. Dupros, G. Larsson, Å. Asmundsson, L. K. Bengtsson, M. Cederberg and M. Jonsson for their help by providing data for the database.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
The study was evaluated and approved by the Regional Ethical Review Board in Lund, Sweden (study approval: 120/2007)
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Informed consent was not sought for this study because the study was conducted through evaluation of patients’ medical records. The Regional Ethical Review Board in Lund, Sweden, approved the study (120/2007) with the condition that an advertisement in the local daily newspaper would be published stating patients not wishing to be included in the analysis could contact the clinic and his or her data would be excluded. The requirement for signed consent was waived off by the Regional Ethical Review Board. This was published on 18 June 2007.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.