
Abstract
Background:
The risk of sudden sensorineural hearing loss associated with metformin use in patients with diabetes mellitus has not been fully examined.
Study design:
It is a retrospective matched-cohort study.
Subjects and methods:
We examined the medical records of patients with diabetes mellitus over 18 years old in Taiwan’s National Health Insurance Research Database for the period between 1 January 2000 and 31 December 2013, to establish matched cohorts (14,109 with and 42,327 without metformin use) at a ratio of 1:3 by sex, age and index year.
Results:
We used a Cox regression hazard model to identify risk factors of sudden sensorineural hearing loss during 14 years of follow-up, and the results indicate that a significantly lower percentage of diabetes mellitus patients with metformin use (p = 0.033) developed sudden sensorineural hearing loss compared with those without metformin use (0.21%, 29/14,109 vs 0.32%, 136/42,327). After adjustment for age and other variables [adjusted hazard ratio: 0.630 (95% confidence interval: 0.422–0.941, p = 0.024)], this study also demonstrated that metformin use appeared to reduce the risk of developing sudden sensorineural hearing loss.
Conclusion:
This study demonstrated an association between metformin use and lower incidence of sudden sensorineural hearing loss among patients with diabetes mellitus.
Introduction
Sudden sensorineural hearing loss (SSNHL) is a type of hearing loss that can lead to permanent hearing disability. The incidence of SSNHL has been increasing globally, affecting an estimated 5 to 27 of every 100,000 people per year. 1 The risk factors of SSNHL include hypertension (HTN), diabetes mellitus (DM) and cerebrovascular and cardiovascular disease. 2 DM has been suggested as a risk factor for SSNHL development; it would thus be valuable to ascertain whether a medication used in DM treatment has a simultaneous protective effect against SSNHL. 3
Metformin has been reported to play a protective role against cerebral or cardiovascular disease and reduce the risk of stroke in patients with DM.4,5 The pathway of this effect is mediated by activation of AMP-activated protein kinase (AMPK), which reduces vascular inflammation and protects the endothelium through nitric oxide synthase. 6 Metformin has also been demonstrated in vitro to protect against hair cell death through gentamicin-induced and cisplatin-induced ototoxicity.7,8
Although the aetiologies of SSNHL remain unclear, the mechanisms are postulated to associate with inflammation, oxidative stress and blood flow disturbance in the inner ear. 3 To evaluate if metformin use is associated with a reduced incidence of SSNHL, we conducted this retrospective cohort study by analysing data from a nationwide medical database.
Materials and methods
This study employed a retrospective matched-cohort design. We acquired data from the National Health Insurance Research Database (NHIRD, an outpatient and hospitalization longitudinal health insurance database in Taiwan). Patients with type 2 DM according to ICD-9-CM code 250 and all its subcodes who were registered in the NHIRD between 1 January 2000 and 31 December 2013 were selected. Eligible patients must have received a diagnosis of DM at least 3 times in the same year according to outpatient clinic records or as their primary inpatient diagnosis. The two study cohorts consisted of selected patients who were over 18 years old during the study period (2000–2013) and had been prescribed with or without metformin for DM treatment. Patients were diagnosed with SSNHL according to ICD-9-CM code 388.2 (sudden deafness). We excluded all patients with a prior SSNHL diagnosis and those who had been prescribed metformin for DM treatment before 2000. Patients with a diagnosis of chronic kidney disease (ICD-9-CM codes 580–589) at any time during the study period were also excluded, because metformin is not indicated in patients with impaired renal function.
We considered variables believed to affect SSNHL risk (age, sex, catastrophic illness and medical comorbidities) as potential confounding factors. The comorbidities are HTN (ICD-9-CM codes 401–405), stroke (ICD-9-CM codes 430–438), hyperlipidaemia (ICD-9-CM code 272), rheumatic arthritis (ICD-9-CM code), ischaemic heart disease (IHD; ICD-9-CM codes 410–414), depression (ICD-9-CM codes 296.2, 296.3, 296.82, 300.4 and 311) and insomnia (ICD-9-CM code 780.52).
The Institutional Review Board of Tri-Service General Hospital approved this study (TSGHIRB No. 2-104-05-126) and waived the requirement of written informed consent to access the NHIRD.
Data analysis
All data analyses were performed using IBM SPSS for Windows, version 22.0 (IBM Corp., Armonk, NY, USA). The chi-square test and Fisher’s exact test were used to compare the difference of categorical variables, and Student’s t test was used to compare the difference of continuous variables between with metformin use group and without metformin use group in diabetic patients. Multivariate Cox proportional hazard regression was used to determine the risk of SSNHL, and the results are presented as a hazard ratio (HR) with 95% confidence interval (CI). The difference in risk of SSNHL for patients with or without metformin use was estimated using the Kaplan–Meier method with a log-rank test. A two-tailed p value <0.05 was considered statistically significant.
Results
Based on the data used in this study, between 1 January 2000 and 31 December 2013, 14,109 DM patients with metformin use were included and a matched 42,327 patients without metformin use were selected as the control group (Supplementary Figure 1). At the end of the follow-up period (Supplementary Table 1), 29 patients with metformin use (0.21%, 29/14,109) and 136 without metformin use (0.32%, 136/42,327) had developed SSNHL, indicating a significantly lower incidence of SSNHL among those with metformin use (p = 0.033). The average follow-up period was 12.3 ± 9.48 years, and the average period for developing SSNHL was 5.98 ± 3.99 years. Significantly lower percentages of IHD (12.94% vs 13.70%; p = 0.021) and depression (0.48% vs 0.65%; p = 0.026) were found in the patients with DM and metformin use, compared with the control group.
The cumulative incidence curve of SSNHL for the cohort with metformin use was significantly lower than for the control cohort, following adjustment for age and other variables (Figure 1; log-rank test, p = 0.028).
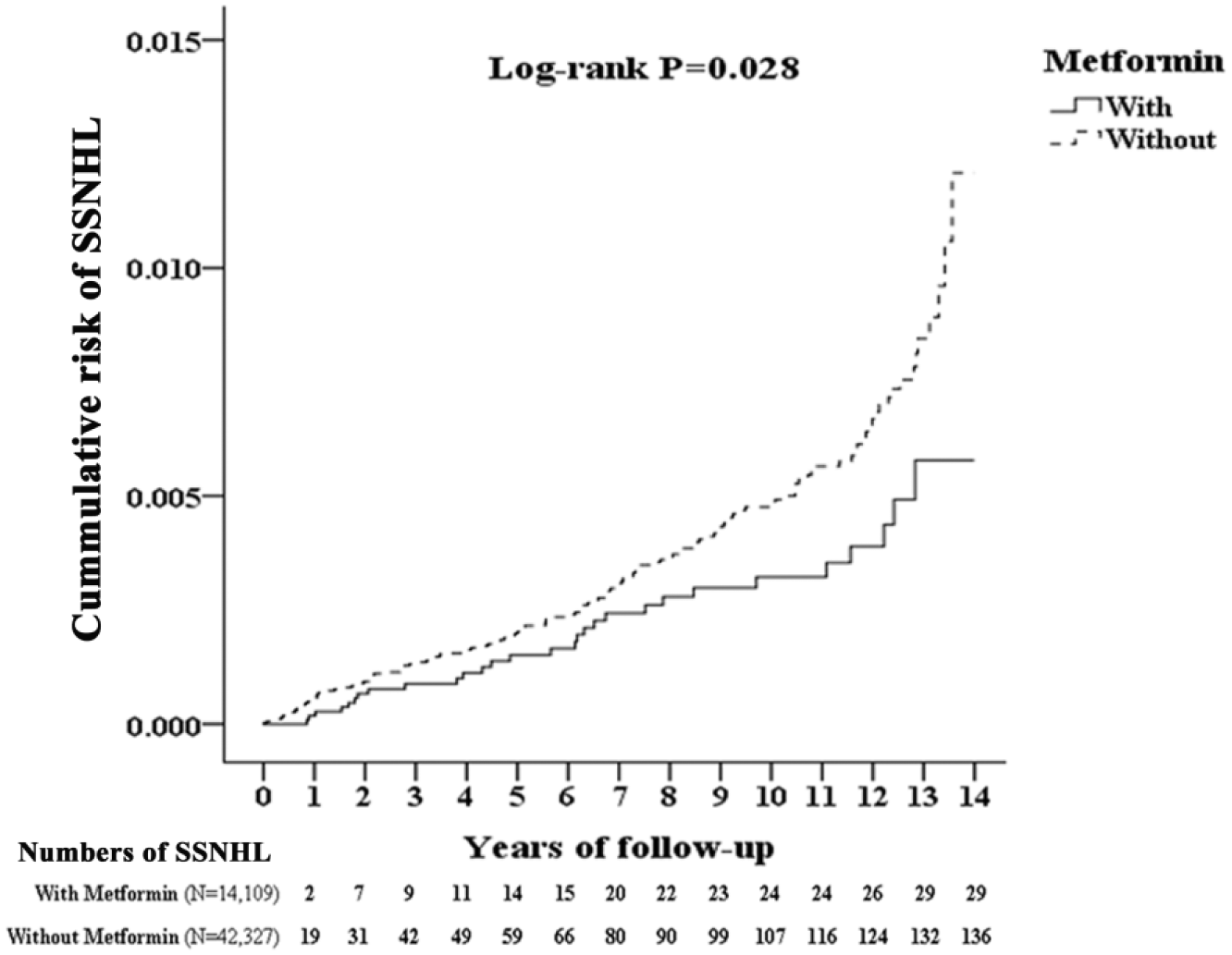
Kaplan–Meier curves for cumulative risk of SSNHL in diabetic patients with or without metformin use. The incidence rate of SSNHL was 17.12 per 100,000 patient–years for diabetic patients with metformin use and 26.70 per 100,000 patient–years for diabetic patients without metformin use [adjusted hazard ratio (95% confidence interval): 0.630 (0.422–0.941)].
After adjustment for age, sex and comorbidities in the Cox proportional hazard regression, metformin use was still significantly associated with a decreased SSNHL risk, with an adjusted HR of 0.630 (95% CI: 0.422–0.941; p = 0.024; Supplementary Table 2). Patients with catastrophic illness, stroke or IHD and older patients had a significantly higher SSNHL risk.
We further investigated the association of factors reducing SSNHL risk with metformin use in a subsequent stratified variable analysis (Supplementary Table 3). A significantly lower adjusted HR was observed among male patients with metformin use (HR: 0.540; p = 0.041) and in patients aged 18 to 44 (HR: 0.453; p = 0.022) and 45 to 64 (HR: 0.592; p = 0.047).
Discussion
This was the first large-scale retrospective matched-cohort study to explore the association between SSNHL and metformin use in patients with DM. This study demonstrated an association between metformin use and lower incidence of SSNHL among patients with DM. The data indicated initial evidence for future more neatly planned research between SSNHL and metformin.
Lin et al. 3 indicated that DM was significantly associated with an increased risk of developing SSNHL, with an adjusted HR of 1.592 and an incidence rate 1.54-fold higher in the DM than in the non-DM group. Moreover, in large-scale studies, metabolic syndromes including DM have been proven to be associated with elevated SSNHL risk. 9 This cautions us to be alert to the increased risk and incidence of SSNHL in patients with DM.
At the end of follow-up in our study, HTN (26.95%) was the most common comorbidity in patients with DM, followed by IHD (13.51%) and stroke (13.29%). Metformin use has been proven to have a protective effect in decreasing stroke and cardiovascular disease (CVD) risk in patients with DM.4,5 Our data showed a significantly lower percentage of IHD in the DM patients with metformin use. Moreover, stroke and CVD are reportedly associated with elevated SSNHL risk, 2 which is also consistent with our study data. Much research has indicated that metformin use appears to control these risk factors and reduces SSNHL incidence in patients with DM.
The mechanism between metformin use and its SSNHL-risk-reducing effect has not been identified. In vitro studies have suggested that metformin is a potential agent against ototoxicity that reduces the number of reactive oxygen species produced by gentamicin and cisplatin.7,8 Metformin use was safe and resulted in a superior hearing threshold in a radiation-induced hearing-loss animal model. 10 The function of metformin is mediated by the activation of AMPK to protect the vascular endothelium. 6 Föller et al. 11 indicated that the AMPK pathway may participate in signalling cascades that protect the inner ear from damage following acoustic overstimulation. These findings further support the potential effect of metformin use in decreasing SSNHL risk in patients with DM.
Our study had several limitations. First, data on the severity of DM (such as HbA1C monitoring) were not available. Second, the precise dose and duration of metformin use were not available. Third, the database did not provide audiometric results assessing the degree of hearing loss and indicating the prognosis in the population with DM. Finally, a population-based study cannot clarify the actual mechanism of the association between metformin use and SSNHL in patients with DM.
Conclusion
An increased risk of SSNHL in patients with DM has been discovered in large-scale population-based studies, indicating the necessity of early detection and treatment for SSNHL in such patients. However, the optimum solution would be to decrease the risk of SSNHL during the course of diabetes. Our study revealed that metformin use in patients with DM appeared to associate with a lower risk of developing SSNHL.
Supplemental Material
supplementary_Fig1 – Supplemental material for Metformin decreases the risk of sudden sensorineural hearing loss in patients with diabetes mellitus: A 14-year follow-up study
Supplemental material, supplementary_Fig1 for Metformin decreases the risk of sudden sensorineural hearing loss in patients with diabetes mellitus: A 14-year follow-up study by Hsin-Chien Chen, Chi-Hsiang Chung, Chieh-Hua Lu and Wu-Chien Chien in Diabetes & Vascular Disease Research
Supplemental Material
supplementary_Table_1_(3) – Supplemental material for Metformin decreases the risk of sudden sensorineural hearing loss in patients with diabetes mellitus: A 14-year follow-up study
Supplemental material, supplementary_Table_1_(3) for Metformin decreases the risk of sudden sensorineural hearing loss in patients with diabetes mellitus: A 14-year follow-up study by Hsin-Chien Chen, Chi-Hsiang Chung, Chieh-Hua Lu and Wu-Chien Chien in Diabetes & Vascular Disease Research
Supplemental Material
supplementary_Table_2_(3) – Supplemental material for Metformin decreases the risk of sudden sensorineural hearing loss in patients with diabetes mellitus: A 14-year follow-up study
Supplemental material, supplementary_Table_2_(3) for Metformin decreases the risk of sudden sensorineural hearing loss in patients with diabetes mellitus: A 14-year follow-up study by Hsin-Chien Chen, Chi-Hsiang Chung, Chieh-Hua Lu and Wu-Chien Chien in Diabetes & Vascular Disease Research
Supplemental Material
supplementary_Table_3_(1) – Supplemental material for Metformin decreases the risk of sudden sensorineural hearing loss in patients with diabetes mellitus: A 14-year follow-up study
Supplemental material, supplementary_Table_3_(1) for Metformin decreases the risk of sudden sensorineural hearing loss in patients with diabetes mellitus: A 14-year follow-up study by Hsin-Chien Chen, Chi-Hsiang Chung, Chieh-Hua Lu and Wu-Chien Chien in Diabetes & Vascular Disease Research
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received financial support for the research, authorship and/or publication of this article: This study was supported in part by grants from the Ministry of Science and Technology of Taiwan (MOST 107-2314-B-016-029 to H-CC), Tri-Service General Hospital (TSGH-C107-028 and TSGH-C108-037 to H-CC, and TSGH-C107-004 to W-CC) and Ministry of National Defense Medical Affairs Bureau, Taiwan, ROC (MAB-106-003 and MAB-107-003 to H-CC). The grantors had no role in the study design, data collection and analysis, decision to publish or preparation of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.