
Abstract
Most data on the burden of diabetes and prediabetes are from countries where local infrastructure can support reliable estimates of the burden of non-communicable diseases. Countries in the Middle East and Africa, together with Russia, have a total population of almost 2 billion, but have been relatively overlooked by authors in this field. We reviewed the prevalence and drivers of prediabetes and diabetes across this large region. A large, and variable, burden of dysglycaemia exists, especially in Middle Eastern and North African countries, associated with high levels of obesity and sedentariness, with a generally lower prevalence in most other parts of Africa. The design and size of studies are highly variable, and more research to quantify the scale of the problem is needed. Local barriers to care relating to issues concerned with gender, consanguinity, lack of understanding of diabetes, lack of understanding of obesity as a health issue, and limited resource at a national level for tracking and intervention for diabetes and other non-communicable diseases. Lifestyle interventions with proven local cost-effectiveness, enhanced access to pharmacologic intervention, and societal interventions to promote better diet and more activity will be an important element in strategies to combat these adverse trends.
Introduction
The adverse impact of type 2 diabetes on longevity, and its powerful adverse impact on the quality of life of both patients and their families are now well established. 1 The incidence and prevalence of the disease have been mapped systematically in many regions, but little is known, however, concerning the current status of the prevalence of type 2 diabetes and its underlying risk factors in large areas of the world.
Here, we focus on a large area – Africa, the Middle East and Russia – with a population of about 1.8 billion, 2 which has been largely overlooked in the clinical literature, compared with developed nations. We have summarised available data on the prevalence and management of type 2 diabetes and its predecessor, prediabetes (non-diabetic hyperglycaemia), risk factors for type 2 diabetes and complications of diabetes within these regions. In this way, we provide a snapshot of the extent and quality of existing data, consider some of the important factors that drive the progression of non-communicable diseases (NCDs) in the region and how diabetes and prediabetes may be managed there in future.
Search strategy
A PubMed search was conducted for names of countries in the region of interest (with the tag ‘[ti]’), together with ‘diabetes’, ‘prediabetes’, ‘impaired glucose tolerance’ and ‘impaired fasting glucose’. Co-authors also provided articles from their own countries, in some cases.
Burden of dysglycaemia
Prevalence of prediabetes and diabetes
Data on the prevalence of prediabetes and diabetes in these countries are summarised in Table 1.3–36
Prevalence of prediabetes and diabetes in the Middle East, Africa and Russia.
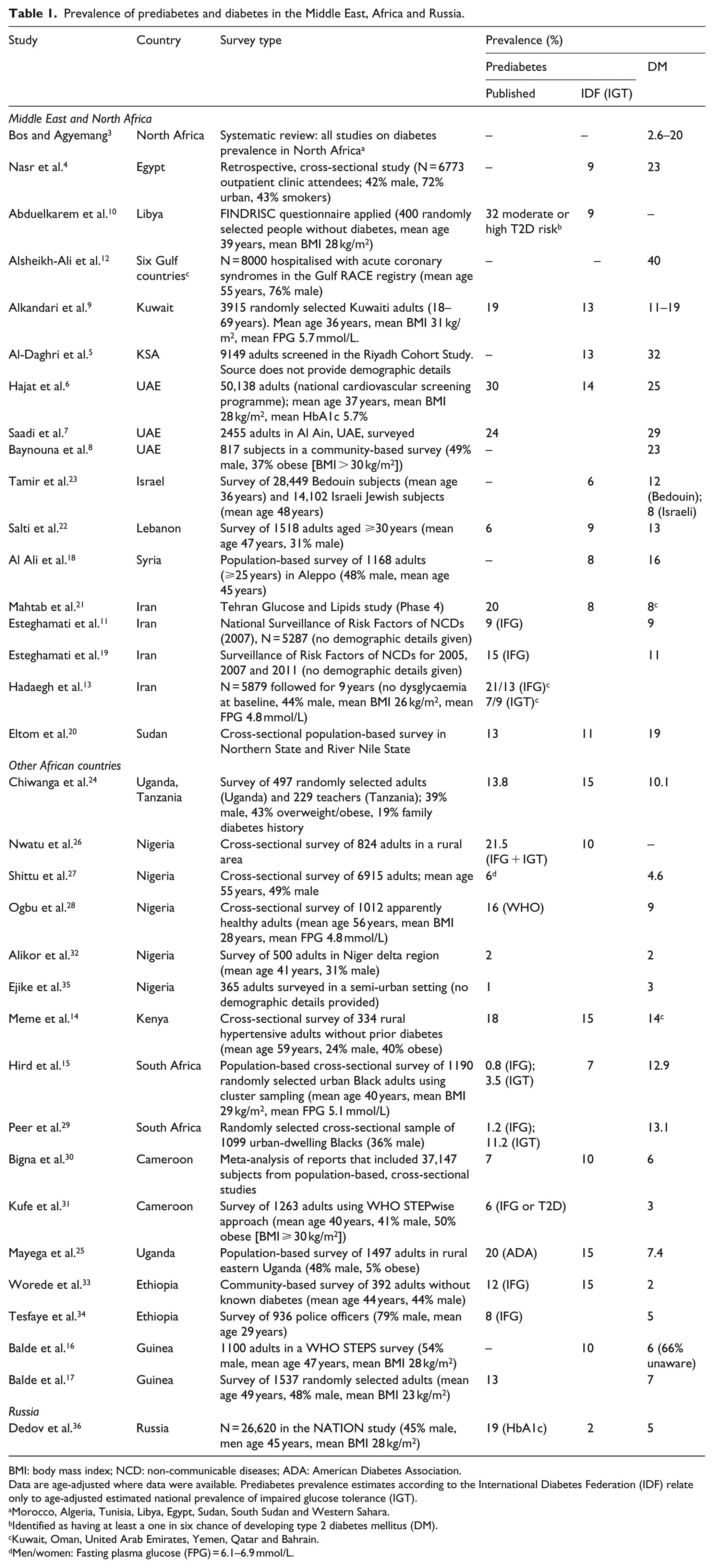
BMI: body mass index; NCD: non-communicable diseases; ADA: American Diabetes Association.
Data are age-adjusted where data were available. Prediabetes prevalence estimates according to the International Diabetes Federation (IDF) relate only to age-adjusted estimated national prevalence of impaired glucose tolerance (IGT).
Morocco, Algeria, Tunisia, Libya, Egypt, Sudan, South Sudan and Western Sahara.
Identified as having at least a one in six chance of developing type 2 diabetes mellitus (DM).
Kuwait, Oman, United Arab Emirates, Yemen, Qatar and Bahrain.
Men/women: Fasting plasma glucose (FPG) = 6.1–6.9 mmol/L.
The true prevalence of dysglycaemia has not been adequately determined across this region. First, the availability of data on prediabetes from peer-reviewed publications in Table 1 is patchy, at best, with data unavailable for a number of countries. These reports vary greatly in design and size, with only a minority representing a national survey. Few (or no) data are available on the study populations presented in most cases (we have sought to include basic data on the populations in the tables of studies in this article); available data vary widely between studies in terms of age, gender balance and use of special populations (e.g. police officers or hospitalised patients). Assessment of the prevalence of prediabetes, where presented, is hampered further by the varying use of fasting plasma glucose (FPG), HbA1c or post-load glucose to define this condition.
Nevertheless, worryingly high prevalence values of forms of prediabetes were identified in countries in the Middle East and North Africa. The prevalence of forms of prediabetes in other African countries was variable, but generally low in other African countries, except for Uganda (where 20% had American Diabetes Association [ADA]-defined prediabetes 25 ). The International Diabetes Federation (IDF) has estimated the global prevalence of prediabetes based only on the age-adjusted national prevalence of impaired glucose tolerance (IGT), 37 presented for the countries included in Table 1. In general, these are lower than published values for Middle Eastern and North African countries, but are substantial for other countries in Africa. The low IGT prevalence of 2% in Russia is also surprising, given the recent finding of a 19% prevalence of HbA1c-derived prediabetes in a large cohort there. 36
The prevalence of diabetes is high in many Middle Eastern/North African countries, approaching or exceeding 20% in some cases. The prevalence of diabetes in sub-Saharan Africa was generally low. The more developed economy of South Africa has a reported diabetes prevalence of around 13% among urban-dwelling Black, subjects which is the highest in sub-Saharan Africa.15,29
A substantial proportion of diabetes was previously undiagnosed in some of these reports. According to the IDF, the proportion of undiagnosed diabetes in the Middle East and North Africa ranged from 17% (Jordan) to 75% (Tunisia). 37 Elsewhere in Africa, the highest proportion of previously undiagnosed diabetes was 92% (Togo); otherwise, 36 out of 37 African countries listed had a proportion of undiagnosed diabetes of at least half. About half of diabetes was undiagnosed in Russia (54%). 36
Overweight and obesity
Obesity, especially abdominal obesity, is closely associated with increased risk of type 2 diabetes, including in Middle Eastern populations. 38 A systematic review from 2009 found a prevalence of obesity of 25% in this region. 39 The studies in Table 2 suggest a substantially higher obesity prevalence in most countries there, although subject to similar limitations of design, size and heterogeneity as described for evaluations of dysglycaemia, above.4-6,8,18,19,25,26,29,31,33,40-50 The UAE appears to bear a particularly heavy burden of obesity (41%) and overweight (34%). 6 One cross-sectional, international epidemiological survey 49 in Table 2 showed a clear trend for higher rates of obesity in countries within North Africa or the Middle East (~40%–50%), versus sub-Saharan Africa (~20%–30%), except for South Africa (~40%), perhaps highlighting the adverse influence of higher levels of development on adiposity.
Prevalence of cardiometabolic risk factors in countries of interest.
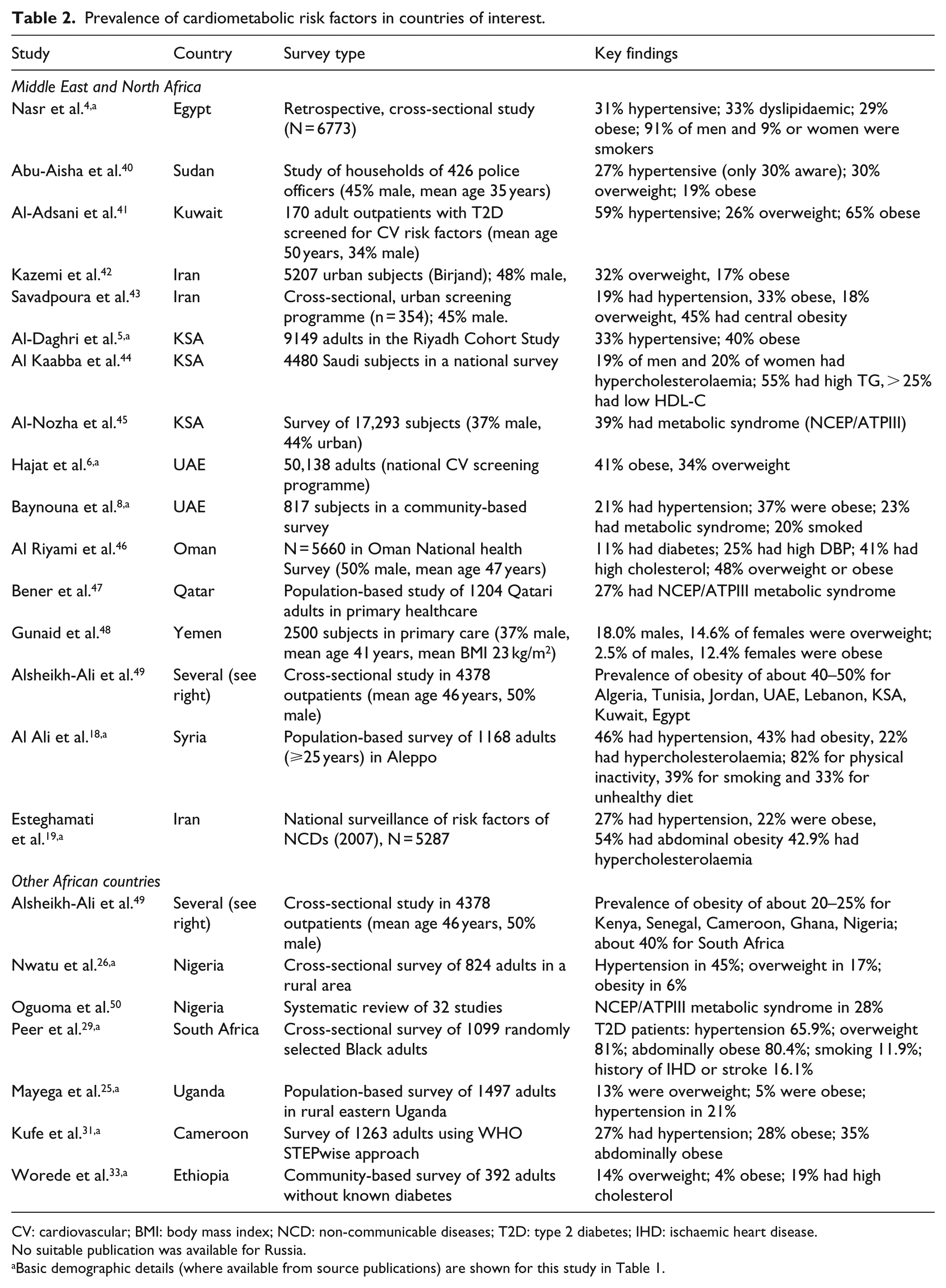
CV: cardiovascular; BMI: body mass index; NCD: non-communicable diseases; T2D: type 2 diabetes; IHD: ischaemic heart disease.
No suitable publication was available for Russia.
Basic demographic details (where available from source publications) are shown for this study in Table 1.
A study in Iran found that body mass index (BMI) cut-offs of 25 kg/m2 for men and 27 kg/m2 for women predicted increased risk of cardiovascular disease; 51 elsewhere, higher BMI cut-off that the standard 25 kg/m2 usually used to define overweight has been proposed for predicting 52 and Oman, 53 supporting a different interaction between genetic environment and cardiometabolic risk there. Optimal waist circumference cut-offs for diagnosing abdominal obesity were also higher for women (especially) in Egypt, compared with standard definitions. 54
Other cardiovascular risk factors
It is important also to consider the prevalence of classical cardiovascular risk factors in this population: these have also been associated with increased risk of type 2 diabetes and most people who develop type 2 diabetes die ultimately of cardiovascular disease. 55 Table 2 also shows a high prevalence of hypertension and dyslipidaemia among patients with type 2 diabetes. Of concern, 9% of adolescent Kuwaiti girls already had the metabolic syndrome (US definition). 56 Although increased uptake of evidence-based therapies promoted some improvements in cardiometabolic risk factors in Middle Eastern subjects with type 2 diabetes, dyslipidaemia and hypertension persisted in about 60%. 57 A high burden of cardiovascular disease in Russia (where there is no established system for tracking cardiovascular risk factors) has been attributed to excess alcohol, smoking, hypertension, sedentariness and poor diet. 58
Factors that may account for variations in prediabetes and diabetes prevalence in the region
Epidemiological transition
Many countries in Africa and the Middle East have relatively young populations. For example, the median age in Oman is only 26 years, 59 yet 75% of the disease burden in the country was already attributable to non-communicable diseases (NCDs) in 2008, and the number of elderly people is expected to increase sixfold over the coming 25 years. 60 This and other demographic shifts in the developing world, such as an increasing trend to urbanisation and improved management of infectious diseases (especially in Africa), are driving an epidemiological public health transition to a preponderance of NCDs.2,60 Table 3 shows that the burden of death from key NCDs is generally as high as that in developed countries.61,62 High rates of smoking and obesity may help to explain this in Middle Eastern countries and in Russia, but apparently not in sub-Saharan African countries, according to these data.
Data from the World Health Organization on the prevalence of key risk factors for non-communicable diseases (NCDs), national policies in place to combat NCDs and burden of mortality from NCDs.
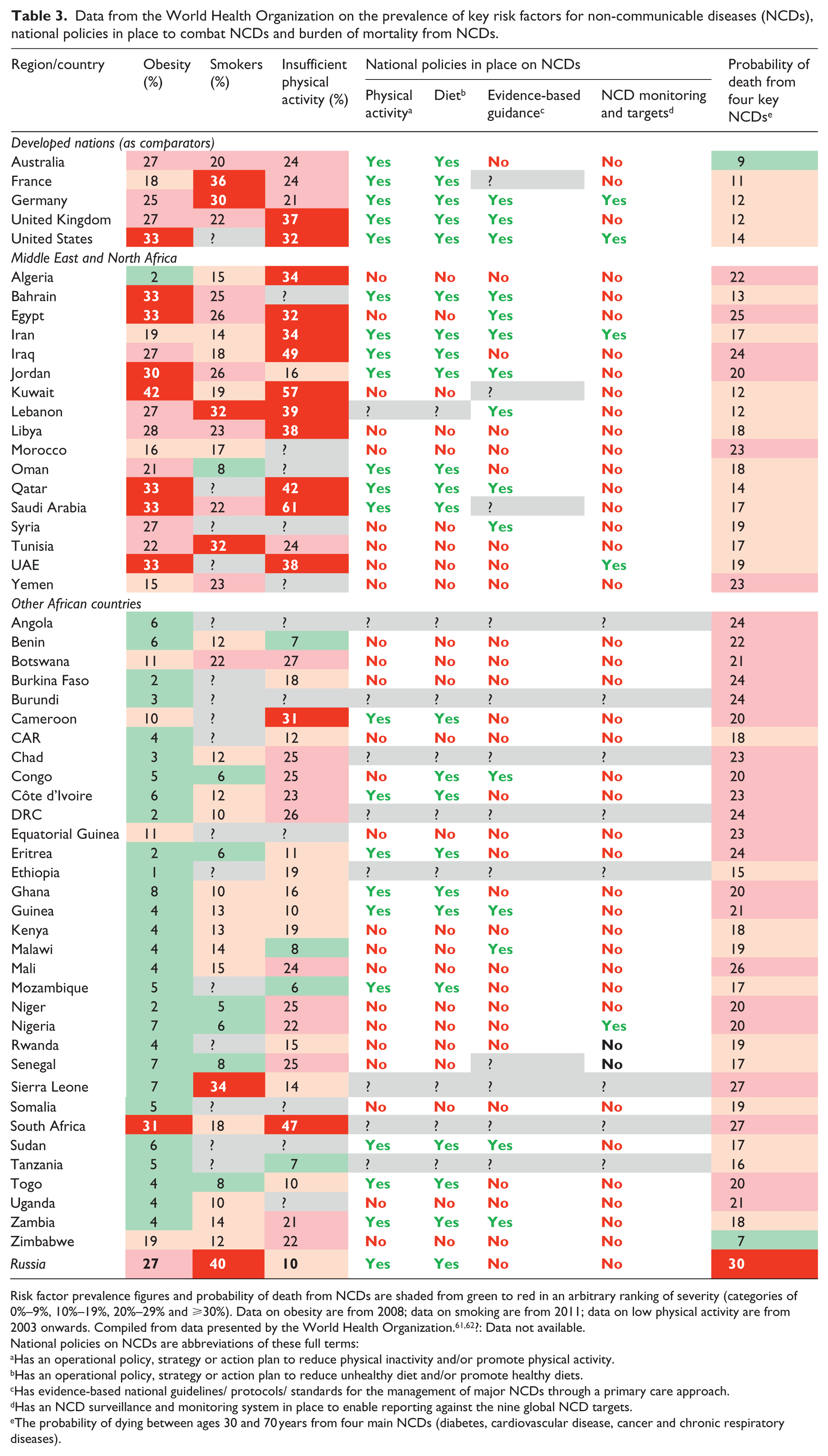
Risk factor prevalence figures and probability of death from NCDs are shaded from green to red in an arbitrary ranking of severity (categories of 0%–9%, 10%–19%, 20%–29% and ⩾30%). Data on obesity are from 2008; data on smoking are from 2011; data on low physical activity are from 2003 onwards. Compiled from data presented by the World Health Organization.61,62?: Data not available.
National policies on NCDs are abbreviations of these full terms:
Has an operational policy, strategy or action plan to reduce physical inactivity and/or promote physical activity.
Has an operational policy, strategy or action plan to reduce unhealthy diet and/or promote healthy diets.
Has evidence-based national guidelines/ protocols/ standards for the management of major NCDs through a primary care approach.
Has an NCD surveillance and monitoring system in place to enable reporting against the nine global NCD targets.
The probability of dying between ages 30 and 70 years from four main NCDs (diabetes, cardiovascular disease, cancer and chronic respiratory diseases).
Other sociodemographic and lifestyle factors
Physical activity and sedentariness are important drivers of increased diabetes prevalence in high-income countries, while an increasing trend to urbanisation is a key factor in middle-income countries. 63 Increasing gross domestic product also drives increasing prevalence in middle-income countries, 63 perhaps providing a bridge between these two mechanisms as a proportion of the population can access a sedentary lifestyle and high-energy foodstuffs. Consumption of unhealthy foods is also more prevalent in the Middle East and Russia than in lower income regions, such as sub-Saharan Africa, as shown by an analysis of surveys covering 89% of the world’s population. 64 Importantly, this study points out that while consumption of healthy foods has increased in higher income countries, consumption of unhealthy foods has increase more.
Other reports have also associated increasing urbanisation with a rising diabetes prevalence. 65 For the countries listed in Table 1 (where data are available), five out of seven in the Middle East and North Africa had 78% or more of their populations living in an urban setting in 2014; elsewhere in Africa, seven out of eight countries have <50% of their populations living in cities (excluding the more developed nation of South Africa, at 64%). 66 Urbanisation may explain some of the differences in dysglycaemia prevalence between our regions of interest, and it is noteworthy that poorer countries are forecast to continue a rapid process of urbanisation. 66
Urbanisation may expose people at risk of diabetes to air pollution. Living within 64 m of a major highway was associated with increase of 0.28 mmol/L in plasma glucose in the US Framingham Offspring study. 67 This association was apparently mediated by exposure to fine particulate carbon and oxides of nitrogen from automobile exhausts. 68 These pollutants also promote a number of other NCDs, especially in middle income countries. 69 Noise pollution has been associated with increased mortality risk among people who already have diabetes. 70
Diabetes risk tends to increase as socioeconomic status falls in Africa, as it does in high-income countries. 71 In addition, climate change has been proposed as both a cause and a consequence of obesity, with these phenomena linked in complex ways.72,73 Efforts to move away carbon-dense economies and a shift away from a diet based on animal products would tend to ameliorate both problems. Access to education is reduced in lower income countries, but the relationship between socioeconomic status, education and diabetes risk is complex. Amalgamation of data from 410 populations in 91 countries suggested that more education reduces the risk of diabetes in higher income countries, but the opposite is true in lower income countries, where access to motorised transport and refined foods among people on the lowest incomes may be limited. 74
Prospects for diabetes prevention and improved health outcomes
Identifying subjects at risk of diabetes
Screening for prediabetes is generally absent in developing countries, which hampers the ability of clinicians to intervene to prevent diabetes. Most of these countries do not have dedicated programmes for surveillance of NCDs, or evidence-based public health initiatives to reduce their burden (Table 3), according to the World Health Organization (WHO).61,62 In addition, there is no well-organised system for detecting gestational diabetes in Russia. 75 There is evidence that migrant populations may be at higher risk of diabetes, for example, South Asian people working in the UAE, who may not be included in such initiatives. 76 The increasing prevalence of dysglycaemia in children cannot be ignored: in the UAE, for example, 5.4% of 11–17 year olds had oral glucose tolerance test (OGTT)-diagnosed prediabetes and 0.8% had type 2 diabetes in 2015. 77
Increasing the awareness of prediabetes in primary care is key to diabetes prevention. Some individual countries are adopting initiatives aimed at single NCD, for example, in Dubai, UAE, primary healthcare centres are screening for prediabetes and diabetes according to ADA recommendations. However, in the experience of the authors, many primary care physicians in their countries do not refer or treat individuals with dysglycaemia until their conversion to clinical diabetes. Primary, secondary and tertiary care need to be integrated to provide continuity for individuals who are at risk of diabetes. Guidelines are being developed in Russia aimed at general practitioners, which aim to increase identification of people at risk of diabetes, using criteria such as age > 40 years, family diabetes history and abdominal obesity.
Local barriers to improved health outcomes
Urgent need for effective lifestyle interventions
Guidelines with international influence, for example, from the ADA 78 or UK National Institute for Health and Care Excellence (NICE), 79 have addressed the management of prediabetes (see Box 1 for details). These focus mainly on lifestyle information, but recommend the use of metformin for selected individuals. NICE provides a separate guideline for population- and community-level interventions. 80 National diabetes prevention initiatives are underway in developed countries such as the United Kingdom 81 and the United States. 82 These are based largely on the intensive lifestyle interventions shown to be effective in randomised trials and can be translated into pragmatic, community-based interventions. 83
Key details of guidelines for the management of prediabetes from the American Diabetes Association and National Institute for Heath and Care Excellence.
American Diabetes Association (ADA) 78
At least annual monitoring of glycaemic status.
Intensive lifestyle intervention, modelled on the Diabetes Prevention Program (DPP).
Weight loss target of 7%, as used in the DPP.
Consider Internet-based social networks, mobile applications or other technological aids, which can be useful in maintaining the lifestyle intervention.
Metformin may be considered, especially for more obese subjects (BMI > 25 kg/m2), age < 60 years, or prior gestational diabetes, that is, the patient groups in which this agent was most effective in the DPP.
UK National Institute for Health and Care Excellence (NICE) 79
Intensive lifestyle interventions delivered in groups of 10–15 at-risk individuals.
Use lifestyle programmes delivered by experienced healthcare practitioners.
Using an approach that builds on the needs and preferences of the patient.
Activity recommendations (at least 150 min of moderate intensity exercise per week), weight loss target (5–10% of initial weight in 1 year) and dietary recommendations are broadly similar to those of the ADA.
Metformin is recommended for patients who do not respond to or are unable to comply with lifestyle intervention, especially where BMI is >35 kg/m2.
This approach provides an opportunity to address local cultural sensitivities and other potential barriers to care, some of which are discussed below. There is no reason to believe that successful implementation of lifestyle interventions will be less effective in preventing the onset of diabetes in sedentary people with obesity in Africa, Russia and the Middle East as it has been proven to be in Western nations. Many published reports support the adaptation for community use of the lifestyle interventions from randomised diabetes prevention trials, such as the Diabetes Prevention Program (DPP). 84 However, lifestyle interventions need to be shown to be effective and cost-effective in local settings, and evidence for this is lacking in countries within the region of interest. Communications technology may provide a way forward, as the use of mobile telecommunications is highly prevalent in developing nations today. A recent systematic review found that ‘e-health’ and ‘m-health’ interventions, where mobile telecommunications are used to provide information, reminders and prompts for specific health behaviours, have shown promise for improving diet and activity levels in developing countries, where healthcare resources are limited. 85
Data from the WHO suggest that high proportions of Middle Eastern/North African subjects, especially women, undertake insufficient physical activity. 62 It is not uncommon for physicians there to initiate lifestyle modification to prevent conversion to diabetes, but there are multiple barriers to achieving successful lifestyle change; in particular, infrastructure for patients to apply, engage with and maintain lifestyle modification is lacking.
Countries in the Middle East, Africa and Russia lack the centralised resources to deliver the community-delivered lifestyle interventions used in the DPP, which included a 16-week curriculum covering diet, exercise and behaviour modification, taught on a one-to-one basis. 84 The cost of lifestyle modification was seen as a major barrier for effective implementation, limiting the support provided by governments and healthcare authorities. Also, for example, most schools in Egypt do not have courtyards for physical exercise, and physical activity is not embedded within local cultural values. In addition, the ‘obesogenic environment’ has been identified as a driver of sedentariness, especially in higher income regions, where most journeys are made by car and physical barriers such as major roads hinder any effort to walk between locations. Recent research has highlighted higher levels of obesity where facilities for physical activity are limited. 86 Ease of access to fast food outlets also has some effect here, and this may be exacerbated by the high level of advertising for these products, especially to children; further study of such relationships is required in these countries. 87
An improved diet is an indispensable component of lifestyle interventions to reduce the future risk of type 2 diabetes, and the Mediterranean diet can reduce the risk of type 2 diabetes, gestational diabetes or cardiovascular disease in at-risk subjects.88,89 However, dietary habits varied considerably among people with or without diabetes in a survey in six Mediterranean countries 90 and people in these countries tend to ‘westernised’ these diets, for example, by addition of meat and omission of fruit, 91 which may increase the risk of type 2 diabetes. 92 Interestingly, rates of obesity in these countries was lower than the typically 80% prevalence seen in populations in Western countries with diabetes. 79
Access to pharmacological intervention
Where physicians intervene to reduce the risk of diabetes, they are likely to prescribe metformin, with or without an attempt at lifestyle intervention. Metformin does not have an indication for diabetes prevention in most countries (it has an indication but no reimbursement in Russia), but is included in guidelines for diabetes prevention (see Box 1). Clinical trials are required to evaluate the effectiveness of metformin in local populations. Its indication elsewhere for use primarily in younger subjects with higher BMI (or when lifestyle intervention has failed) could be implemented in these countries until such evidence is available. Metformin abuse for weight loss is promoted widely across the Internet and is likely widespread, including in Middle Eastern countries, although the prevalence of this behaviour is currently unknown.
Consanguinity
Having a first degree relative with type 2 diabetes is an important diabetes risk factor, and the practice of consanguineous marriage has been associated with an increased risk of type 2 diabetes in an Arab population. 93 There is a high rate of consanguinity in Arab countries, of about 30% in North African countries (except for an extremely high prevalence of about 80% in Nubian communities, where marrying outside the family is discouraged) and exceeding 50% in the Gulf region. 94
Gender-specific issues
The overall rate of sedentariness of 61% in Saudi Arabia (Table 3) contains rates of 53% for men and 69% for women. 62 Cultural roles and expectations of women in Middle Eastern countries tend to promote physical inactivity. Sensitivities around been seen exercising in public, and lack of suitable segregated facilities for women, have been identified as a significant barrier to increased physical activity for women. 95 Initiatives are underway in several countries to promote physical activity for women, some with government support. 96
Obesity is seen as a ‘healthy’ and socially acceptable in female populations in the Middle East. In Sudan, obesity is associated with beauty. Furthermore, some young women in Sudan use steroids to gain weight and refuse to take metformin because it is associated with weight loss.
Smoking rates are broadly similar in Middle Eastern countries versus Western countries (Table 3). 61 A 10-fold higher prevalence of smoking among Egyptian men versus women 4 and higher smoking rates for men versus women elsewhere in the Middle East 39 have been described, highlighting an important cultural difference between men and women there, although smoking rates are increasing among Middle Eastern women, particularly younger women. 92
Other cultural barriers
Younger generations are more likely to adhere to lifestyle modification, but this population is less at risk of developing diabetes compared with older generations. Thus, the individuals with the highest risk of developing diabetes are those who are the least likely to adhere.
Misconceptions about diabetes and its treatment are common. A stigma associated with diabetes in the Middle East contributes to this problem, and patients often resent being ‘labelled’ with a diagnosis and either do not comply with or refuse treatment. Patients there tend to equate health with absence of visible disease, with limited attention paid to ‘invisible’ conditions, such as prediabetes or early diabetes; religious convictions and fatalism over the course of life may be strong modifiers of attitudes to NCDs and their treatment. 97 Complementary/alternative therapy is common in the Middle East, highlighting the need for education on diabetes.98,99
Discussion
A high prevalence of prediabetes and type 2 diabetes is already established in the nations of the Middle East and in the Arabic-speaking nations of North Africa, where its prevalence has been described as ‘alarming’ or ‘dramatic’. In addition, diabetes is an established cause of morbidity and mortality, along with other NCDs in Russia. Complications of established diabetes are prevalent in these countries. In two tertiary centres in Sudan, 68% of subjects had neuropathy, 73% had retinopathy, 40% had hypertension and 60% had hypercholesterolaemia; glycaemia was well controlled in only 16%. 100 A systematic review of studies from throughout Africa found prevalence of up to 42% for retinopathy, 22% for albuminuria, 46% for nephropathy and 60% for neuropathy. 3 Patients with newly diagnosed diabetes in Alexandria, Egypt, already had evidence of diabetes complications, for example, neuropathy (3%), and nephropathy, retinopathy and peripheral artery disease (10% for each); the prevalence of these complications was 29%–48% for patients with known diabetes. 101 Complications (nephropathy and peripheral neuropathy) were also prevalent in the UAE for people with type 2 diabetes (44% and 37%, respectively) and prediabetes (29% and 13%, respectively); 73% of type 2 diabetes patients had retinopathy here (not investigated in prediabetes). 7
Importantly, complications of diabetes are already evident is some people with prediabetes. Recent data from the Whitehall II cohort showed that the risk of a major adverse cardiovascular event or death was increased in people with prediabetes (WHO or ADA definitions) versus normoglycaemia by 12%–17% after adjustment for confounders. 102 Other studies have shown that prediabetes increased the risk of adverse cardiovascular outcomes or death.103,104
Conversely, moving from prediabetes to normoglycaemia reduces the risk of subsequent cardiovascular disease. 105 Impairments of microvascular function and/or damage to the retina have also been observed in people with prediabetes.106–109 We lack assessments of the prevalence of complications typical of diabetes in people with prediabetes within the countries of interest to this review, but it is reasonable to assume that the adverse effects of prediabetes on the vasculature and nerves would also occur in these populations.
In general, a high prevalence of obesity, fuelled by sedentary habits and high-energy diets underlies the problem of dysglycaemia in these countries. However, prediabetes and type 2 diabetes are emerging as a problem even in sub-Saharan Africa, where an epidemiological transition and relentless urbanisation are replacing infectious diseases with NCDs and the countries’ major health threat. Improved lifestyles, and pharmacologic intervention where appropriate, will be an important element in strategies to combat these adverse trends.
Call to action
The people of Africa, the Middle East and Russia should be at the forefront of interventions to reduce the burden of NCDs, but a Westernised approach will be insufficient: it is crucially important that these strategies address the distinct cultural and other barriers to diabetes prevention and management that prevail in these nations. 110 A call to action is needed, aimed at governments, international healthcare institutions, local diabetes societies and leading physicians to undertake multiple medical and societal interventions in these countries. These would be the subject of another review, but will certainly include education on improved lifestyles, awareness campaigns on diabetes prevention (including changing the food environment for children and young adults in school or university), legislation on food labelling and reduced availability of sugary foods/drinks.111,112 Pharmacologic therapy for diabetes prevention needs to be more widely accessible, supported by licenced indications and reimbursement, for those who cannot or will not undertake an intensive lifestyle intervention. Figure 1 summarises the types of approach that will be needed.
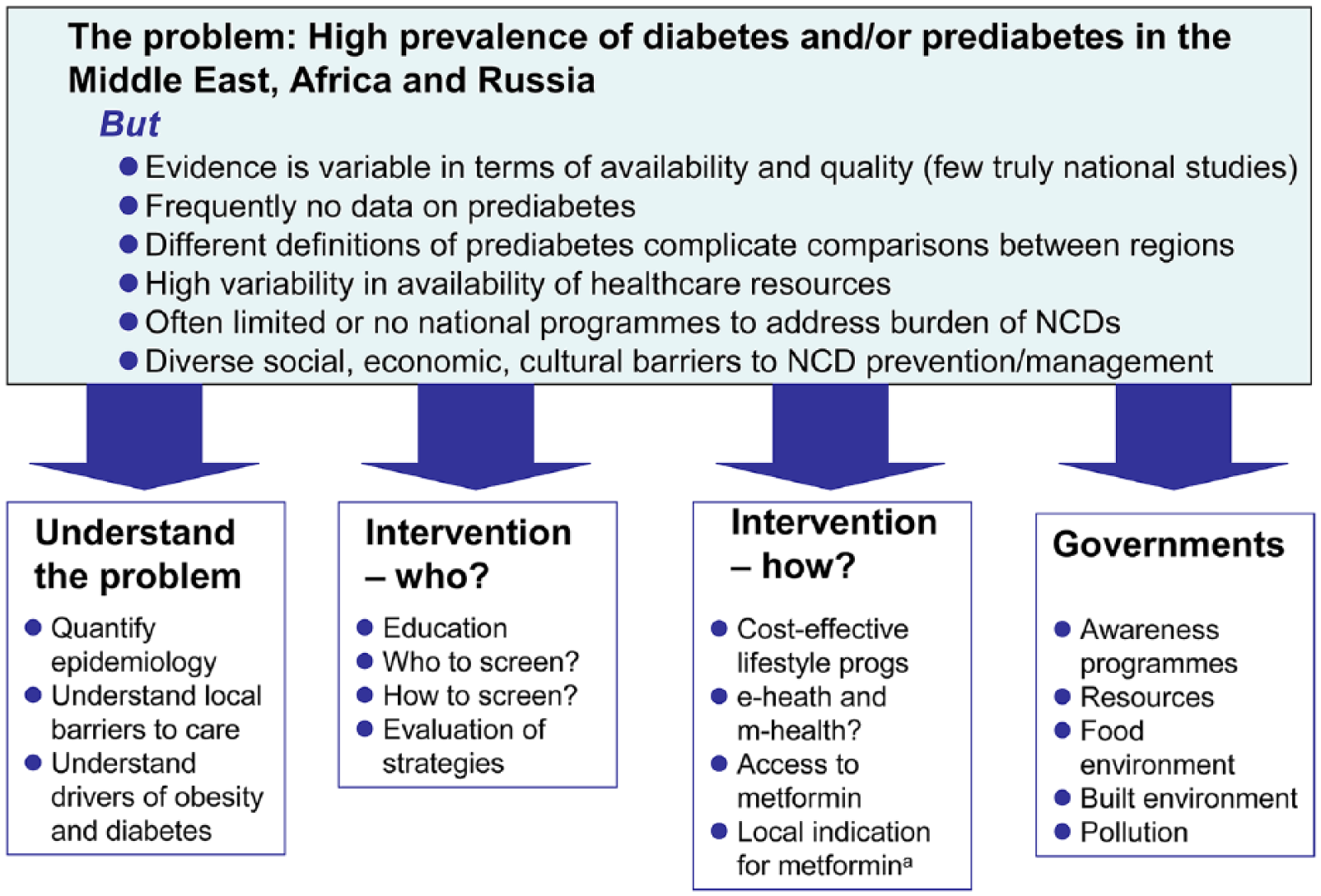
Summary of new approaches needed to address the burden of diabetes and prediabetes in the Middle East, Africa and Russia.
There is also a pressing need for more research. The size of the challenge of diabetes and prediabetes needs to be defined quantitatively and systematically, given the disparate nature of the evidence base in these countries. Further information is needed on the key drivers of obesity and other NCDs at a regional and national level, supported by more national programmes for tracking and intervening to reduce their impact on public health. Finally, we need to know how to conduct successful lifestyle interventions in low- and middle-income countries. The progress made with m-health programmes, described above, may provide a promising avenue for this.
Footnotes
Acknowledgements
A medical writer (Dr Mike Gwilt, GT Communications, funded by Merck) provided editorial assistance in the development of the manuscript. The authors retained full control over the content of the manuscript. Dr Salim Mihson Alruba, a leading diabetes physician in Iraq, contributed importantly to the ideas behind this article, but sadly passed away before its preparation. The authors acknowledge this contribution, and our thoughts and prayers are with his family.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This review arose from a meeting funded by Merck (all coauthors thus acted as honorary consultants to Merck). S.M. and U.H. are employees of Merck.