
Abstract
More than 1 in 10 US adolescents have prediabetes or diabetes, and elevated glycosylated haemoglobin (HbA1C) in youth is associated with increased risk of death before the age of 55 years. We conducted a prospective, cross-sectional study of 31,546 consecutive volunteer blood donors, 16–19 years of age, who donated blood during school blood drives between 1 September 2011 and 21 December 2012 in Texas. In the overall cohort, the prevalence of elevated HbA1C was 11.5%, including 11.0% in the prediabetes range (HbA1C 5.7%–6.4%) and 0.5% in the diabetes range (HbA1C ⩾ 6.5%). The prevalence of elevated HbA1C was higher in boys compared with girls (15.7% vs 7.9%, p < 0.001) and was especially high in racial/ethnic minorities (Blacks 32.7%, Asians 19.7%, Hispanics 13.1%) compared with Whites (8.0%, p < 0.001). There was a significant increase in total cholesterol and blood pressure across categories of increasing HbA1C in the overall cohort and stratified by sex and race/ethnicity. Blood donation programmes can serve as unique portals for health screening with potential for intervention in adolescents.
Introduction
The global epidemic of diabetes mellitus affects all age groups, 1 with approximately 215,000 children and adolescents in the United States diagnosed with diabetes based on data from the US Centers for Disease Control and Prevention (CDC). 2 The estimated prevalence of diagnosed diabetes in youth 15–19 years of age in the multicentre SEARCH for Diabetes in Youth Study was 0.4% in 2009, 3 representing a significant increase compared with similar data from 2001. 4 In addition, 11.8% of youth 16–19 years of age in the 2005–2006 National Health and Nutrition Examination Survey (NHANES) had prediabetes based on fasting plasma glucose (FPG) and/or oral glucose tolerance testing (OGTT). 5
An increasing number of blood centres provide basic clinical lab testing such as total cholesterol with results made available to donors, in addition to the mandated screening for haemoglobin/haematocrit and transfusion-transmissible infectious diseases. 6 The recent endorsement by the American Diabetes Association (ADA) 7 of glycosylated haemoglobin (HbA1C) for diabetes screening, eliminating the requirement for fasting blood collection, provides opportunity for screening in blood donors who are by protocol non-fasting. While the HbA1C criteria for diabetes and prediabetes classification are based on data derived from adult populations, with uncertain accuracy in children and adolescents,8,9 the potential public health value of HbA1C screening in adolescents is supported by recent data from the CDC showing that elevated HbA1C at baseline in adolescents and young adults was associated with a significantly higher risk of death before the age of 55 years. 10
Leveraging an existing programme of high school blood drives that represent over 20% of all blood donated in North Texas, we implemented a regional HbA1C screening programme in a large adolescent blood donor population. Preliminary data from this programme have been previously published in a brief research letter, 4 with this study comprising a markedly increased sample size and more detailed analyses of sociodemographic and clinical features associated with elevated HbA1C levels.
Methods
Study population
Blood samples were collected from consecutive adolescent donors 16–19 years of age during school blood drives conducted between 1 September 2011 and 21 December 2012 by Carter BloodCare, the largest independent blood programme in the state of Texas. Donors were provided instructions on secure retrieval of their HbA1C results from the blood centre’s website using unique identification codes. Demographic data collected for each donor were those routinely collected as part of the donation process: date of birth, sex, race/ethnicity (optional), school name and zip code. The study was approved by the University of Texas Southwestern Medical Center (UTSW) Institutional Review Board with waiver of informed consent.
Definitions
The cut-offs used for HbA1C stratification were those endorsed by ADA for diabetes, HbA1C ⩾ 6.5% (⩾48 mmol/mol), and prediabetes, HbA1C 5.7–6.4% (39–46 mmol/mol). 3 We used the US Department of Education 2009 Rural and Low-Income School Programme eligibility spreadsheet for the state of Texas to categorize rural versus urban and low- versus not low-income designation of high school donation sites. Race/ethnicity was defined by donor self-report, with pre-defined options including White, Black, Hispanic, Asian and Other/Mixed.
Assay methods and characteristics
Whole blood aliquots were collected in BD Vacutainer™ Blood Collection tri-potassium ethylenediaminetetraacetic acid (K3EDTA) tubes. After routine screening for infectious diseases, the residual sample was used for clinical testing. HbA1C was measured in a Clinical Laboratory Improvement Amendments (CLIA)-certified laboratory (Creative Testing Solutions, Bedford, TX, USA). An antibody-mediated latex agglutination inhibition assay (Beckman Coulter AU system; coefficient of variation ⩽4%) was used for all samples for non-Black donors, while samples from Black donors were measured using an ion exchange high-performance liquid chromatography assay (Bio-Rad D10; coefficient of variation ~1.2%). This was done because initial results in Black donors (1 September 2011–30 December 2011) showed artifactually high HbA1C values, with HbA1C ⩾ 5.7% in 53.4% (281/526) of Blacks using the Beckman Coulter assay. This prompted a quality assurance process with co-measurement of HbA1C on split samples using the Beckman Coulter assay and the Bio-Rad D10 assay in 111 random samples from Black, White, and Hispanic donors. Test results with the two assays were highly correlated in White and Hispanic donors, with intra-class correlation coefficients (ICCs) 0.819 and 0.565, respectively, but much less so among Black donors (ICC = 0.026). This is attributable to interference by haemoglobin variants S and C in Blacks, a known limitation of the Beckman Coulter assay, but not of the Bio-Rad assay. For this reason, all results from Black donors that had been obtained using the Beckman Coulter assay (1 September 2011–30 December 2011) were discarded (N = 526), and samples collected between 31 December 2011 and 21 December 2012 (N = 1967 Black donors) were analysed with the Bio-Rad assay. Both methods used for determining HbA1C are certified by the National Glycohaemoglobin Standardization Program (NGSP) and standardized to the Diabetes Control and Complications Trial (DCCT) reference assay.
Non-fasting total cholesterol was measured using the Beckman Coulter AU system, certified to meet the National Cholesterol Education Program’s (NCEP) performance criteria for accuracy. Blood pressure measurements were obtained using a Welch Allyn Spot Vital Signs LXi® automated blood pressure monitor.
Statistical analyses
Summary statistics are reported as mean ± standard deviation (SD) for continuous variables and number (%) for categorical variables. The Student’s t-test was used to compare continuous variables, and comparisons of individuals with HbA1C ⩾ 5.7% versus <5.7% were performed using the chi-squared test for categorical variables. For comparing HbA1C categories in rural versus urban schools and for low-income versus other schools, the Cochran–Mantel–Haenszel test was used, adjusting for ethnicity. Trend comparisons across categories of HbA1C were performed using the Cochran–Armitage test for categorical variables and a test for linear trend via linear regression for continuous variables. For all analyses, two-tailed p values <0.05 were considered statistically significant, and no corrections were made for multiple comparisons. All statistical analyses were performed using Statistical Analysis System (SAS) version 9.2 (SAS Institute Inc., Cary, NC, USA).
Results
Blood samples were collected from a total of 32,696 high-school blood donors, with data from the initial 1150 Black donors discarded due to limitations of the Beckman Coulter assay described in the Methods section, yielding a total analysis sample of 31,546 adolescent blood donors. Pilot overall summary results from the first 14,850 donors have been previously published. 4 The present cumulative cohort included 52.9% girls, with 16,536 (52.4%) White, 1967 (6.2%) Black, 8317 (26.4%) Hispanic, 699 (2.2%) Asian and 4027 (12.8%) participants of other/mixed or undeclared ethnicity. Cohort characteristics stratified by HbA1C category are presented in Table 1. In the overall cohort, HbA1C was above the diabetes threshold in 167 blood donors (0.53%; 95% confidence interval (CI): 0.46, 0.62), and in the prediabetes range in 3480 blood donors (11.0%; 95% CI: 10.69, 11.38).
Sociodemographic characteristics of the study population by HbA1C categories (percentages for each characteristic are across columns, and do not add up to 100% for race/ethnicity because of rounding).
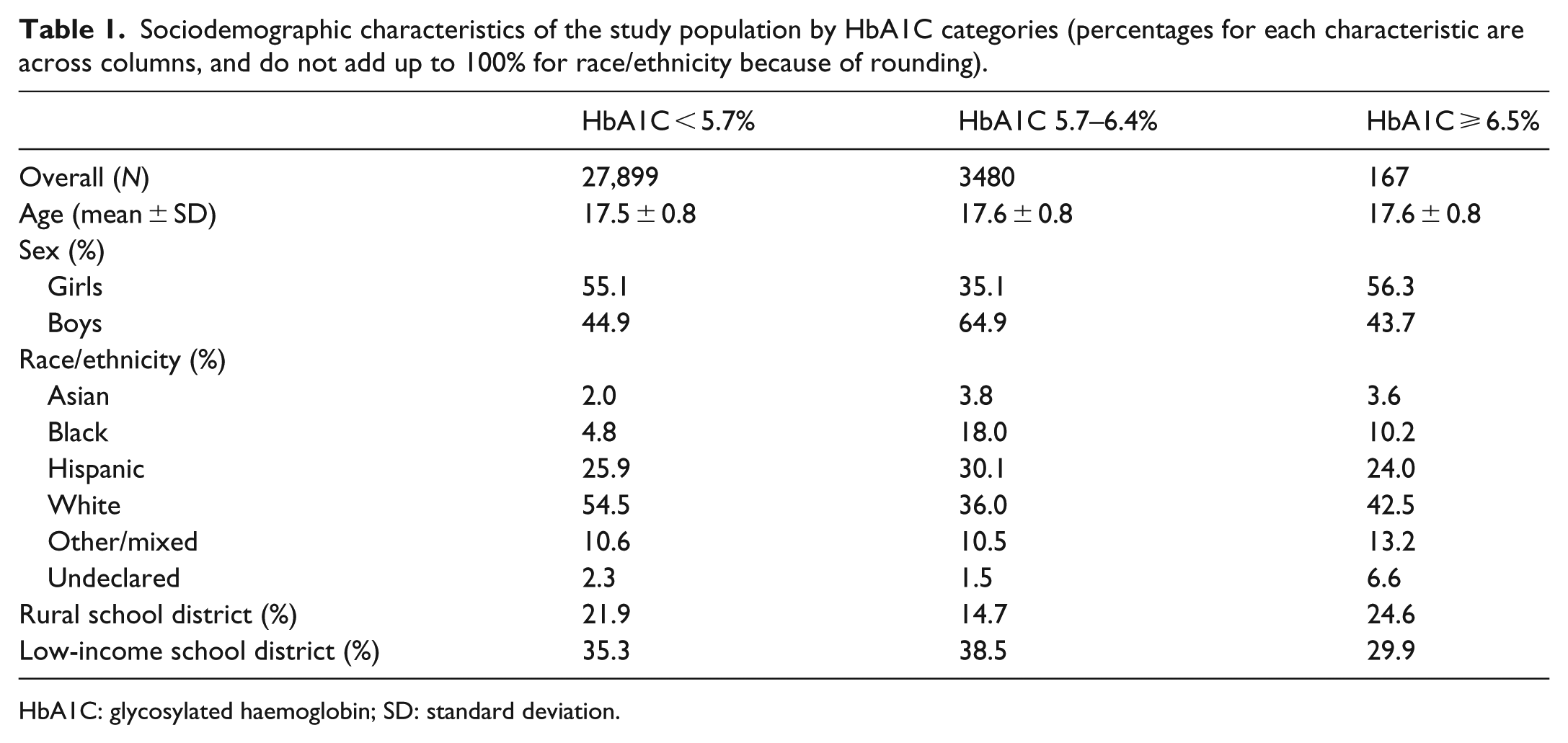
HbA1C: glycosylated haemoglobin; SD: standard deviation.
Subgroup analyses
The prevalence of HbA1C ⩾ 5.7% (prediabetes + diabetes range) within sex, race/ethnicity and sociodemographic strata is shown in Figure 1. HbA1C ⩾ 5.7% was more prevalent in boys compared with girls (15.7% vs 7.9%; p < 0.001) and in racial/ethnic minorities compared with Whites (p < 0.001 for each racial/ethnic group vs Whites). In analyses restricted to data collected after 31 December 2011 when HbA1C in Blacks became available, the racial/ethnic differences persisted. Boys were more likely to have a HbA1C ⩾ 5.7% than girls within race/ethnicity strata, and conversely, racial/ethnic differences were preserved within sex strata (Figure 2). There was a greater proportion of adolescents with HbA1C ⩾ 5.7% in urban versus rural school districts (12.4% vs 8.3%; p < 0.001), and in low-income versus not low-income school districts (12.4% vs 11.1%; p < 0.001), and these differences were preserved after adjustment for race/ethnicity (p < 0.001 and p = 0.003, respectively). Qualitatively similar trends were observed when evaluating the HbA1C threshold of ⩾6.5%, but small absolute numbers across strata preclude meaningful statistical analysis. Importantly, donors with HbA1C 5.7%–6.4% and HbA1C ⩾ 6.5% were widely distributed across the North Texas region of operation of the blood centre, with no geographic localization of particularly high prevalence of abnormal HbA1C (data not shown).
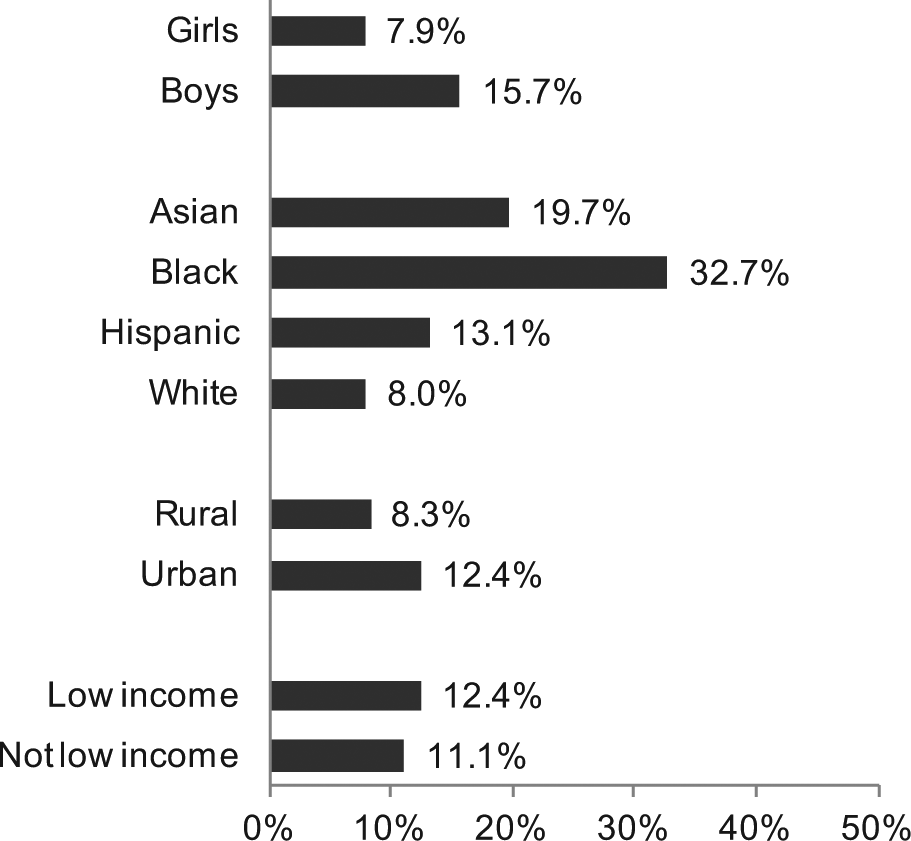
Prevalence of haemoglobin A1C ⩾ 5.7% (encompassing the prediabetic and the diabetic range) within sex, race/ethnicity and sociodemographic strata.
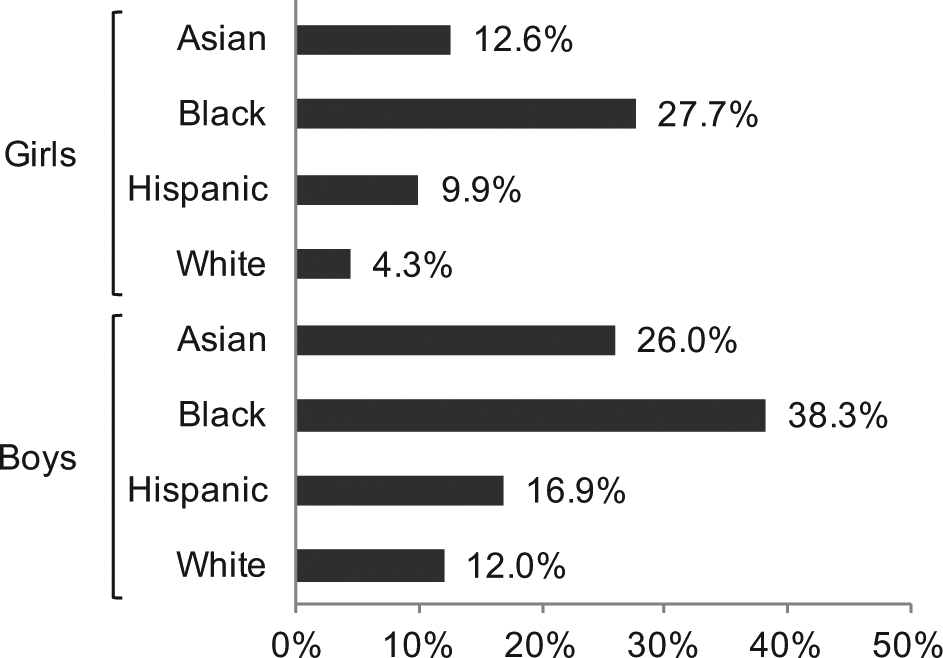
Prevalence of haemoglobin A1C ⩾ 5.7% (encompassing the prediabetic and the diabetic range) stratified by sex and racial/ethnic group.
HbA1C and cardiovascular risk factors
There was a significant increase in total cholesterol, systolic blood pressure and diastolic blood pressure across categories of increasing HbA1C in the overall cohort, in subgroups of boys and girls and in subgroups of Hispanic and White donors, with qualitatively similar trends observed in the smaller subgroups of Asian and Black donors (Table 2).
Selected cardiovascular risk factors stratified by HbA1C categories, in the overall cohort and in sex and racial/ethnic subgroups.
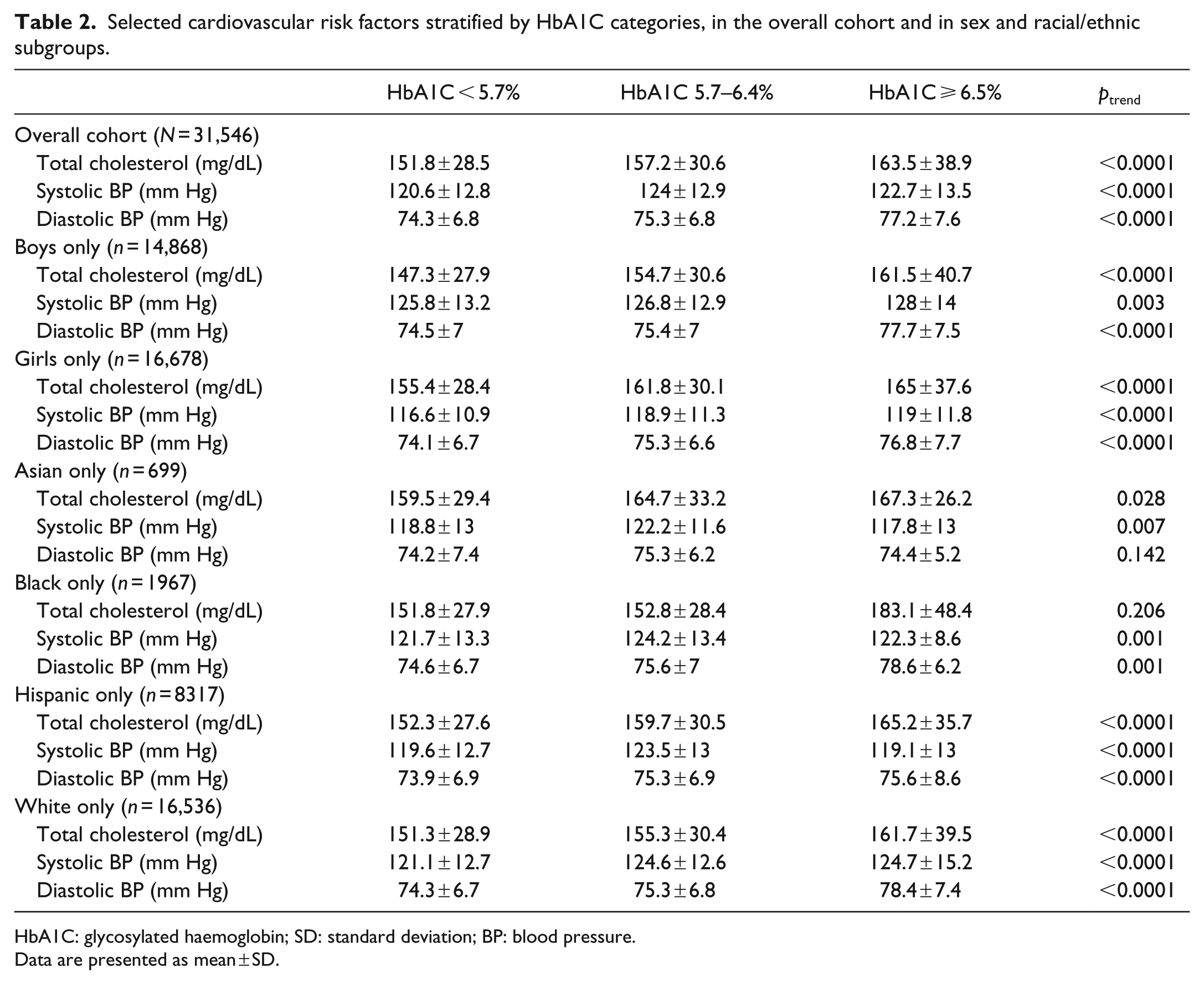
HbA1C: glycosylated haemoglobin; SD: standard deviation; BP: blood pressure.
Data are presented as mean ± SD.
Voluntary retrieval of HbA1C test results
Overall, test results were retrieved by only 7.3% of adolescent blood donors. Adolescents with HbA1C ⩾ 5.7% had lower rates of retrieval compared with those with HbA1C <5.7% (5.8% vs 7.4%; p < 0.001).
Discussion
There are several key findings from this study of a very large, multiethnic cohort of North Texas adolescent blood donors. The prevalence of HbA1C in the diabetes range was higher than the most recent prevalence estimate of diagnosed diabetes reported by the SEARCH for Diabetes in Youth Study for the index year 2009. 3 The prevalence of HbA1C in the prediabetes range was comparable with recent national estimates based on impaired fasting glucose and/or impaired glucose tolerance in NHANES. 5 Abnormal HbA1C was especially prevalent among boys and in racial/ethnic minorities and was associated with cardiovascular risk factors including higher blood pressure and total cholesterol.
Diabetes and prediabetes in adolescents
The prevalence of diabetes is increasing at an alarming pace in US adolescents and young adults, with recent increases reported in the prevalence of both type 1 and type 2 diabetes. 4 Undiagnosed and untreated diabetes in youth has potentially dire long-term health consequences, whereas early diagnosis and clinical intervention may reduce the burden of diabetes and the incidence of diabetes complications later in life. 11 There are no reliable estimates of the prevalence of undiagnosed diabetes in US youth. For diagnosed diabetes, the multicentre SEARCH for Diabetes in Youth study provided detailed estimates for the 2001 index year,12–15 and more recently for the 2009 index year, with a reported prevalence of 0.4% in youth 15–19 years of age. 3 The prevalence of HbA1C ⩾ 6.5% in this study was numerically higher, but differences in study design and population preclude a meaningful interpretation of this difference.
The estimated prevalence of prediabetes (defined as impaired fasting glucose and/or impaired glucose tolerance) in unadjusted analyses from a small subset of boys and non-pregnant girls drawn from the 2005–2006 NHANES sample was 16.1% in the 12- to 19-year-old age group and 11.8% in the 16- to 19-year-old age group. 5 The slightly lower prevalence of prediabetes as defined by HbA1C in 16- to 19-year-old students in this study could be in part attributable to differences in methodology, since FPG and OGTT were used in the NHANES report. 5 HbA1C has lower sensitivity in adolescents compared with adults for the detection of prediabetes (defined by OGTT), and thus, HbA1C may underestimate the prevalence of prediabetes in youth.8,9 On the other hand, FPG and OGTT, but not HbA1C, are dependent on subject compliance with test requirements (particularly fasting), and the prevalence of abnormal glucose metabolism may be overestimated by poor compliance, a relatively common issue in this age group. Finally, a ‘healthy blood donor’ bias may also contribute to the lower observed prevalence of prediabetes (and also of diabetes range HbA1C), as those with or at high risk of prediabetes/diabetes may be less likely to volunteer to donate blood or may be excluded from donation. 6 In spite of these differences, the observed prevalence of prediabetes is comparable with the results from NHANES, thus lending further support to the use of HbA1C as screening tool in adolescents.
Importantly, puberty is associated with a variable degree of physiologic insulin resistance that recedes after Tanner stage IV.16,17 This is the most likely reason why the estimated prevalence of prediabetes in NHANES was higher in the 12- to 15-year age group compared with the 16- to 19-year age group. 5 The transient insulin resistance of puberty is unlikely to play a role in this study restricted to adolescents 16–19 years of age.
Sex, race/ethnicity and rural versus urban setting
The observed higher prevalence of prediabetes in boys compared with girls is consistent with previous findings in this age group 5 and is likely part of a continuum with similar sex differences in the adult US population. 18 Similarly, the higher prevalence of abnormal HbA1C in racial/ethnic minorities, particularly among Black youth, mirrors the racial/ethnic disparities in diabetes risk and prevalence in the adult US population. It is particularly striking that almost one in three Black donors in this study had abnormal HbA1C values. This could reflect a very high prevalence of prediabetes among Black adolescents in North Texas, but could also be in part attributable to previously reported glucose-independent racial differences in HbA1C levels. 19 The lower observed prevalence of abnormal HbA1C in rural versus urban donor-sites is somewhat surprising given the higher prevalence of diabetes in rural adults, 20 the higher prevalence of obesity in rural children, 21 as well as the overall ‘rural health disadvantage’ described in the United States. 22 However, since the present cohort is not a probability-based population sample, we are unable to infer that prediabetes is less prevalent in rural versus urban North Texas adolescents in general.
The blood programme as a portal for community-based research and intervention
This study demonstrates the feasibility of using the community blood programme as a portal for public health screening. Leveraging this programme may represent a highly efficient means of performing large-scale research, clinical screening and referral for intervention, as ~40,000 individuals a day volunteer to donate blood in the United States. Moreover, for many blood collection programmes, up to 25% of donors are high-school students. Although there are notable drawbacks to health screening of blood donors (e.g. testing that requires fasting is not feasible), there are also compelling advantages. All donors, regardless of whether they are first time, infrequent or regular registrants, have blood drawn at each donation for serological markers of infectious disease. Additional tests can be included with trivial inconvenience to the donors. Furthermore, blood programmes rely on information management systems that reliably and confidentially maintain comprehensive donor demographic records and, where appropriate, permit retrieval of test results. For individuals with a history of regular donation, changes in health risks could be monitored over time, allowing for early referral to medical care when test results become abnormal. Although only a minority of donors retrieved test results in this study, campaigns to increase health education and risk awareness (e.g. ‘Know your numbers’ campaigns) could potentially increase the proportion of donors who retrieve their test results, which in turn could serve as an incentive for the adoption of risk reduction measures at the individual and community level.
Strengths and limitations
This study has several key strengths, including the large size of the study population, its racial/ethnic and socio-economic diversity, and focus on the vulnerable population of adolescents. There are also important limitations. First, there is ongoing controversy about the role of HbA1C in the diagnosis of diabetes and prediabetes in youth.8,9 The lower sensitivity of adult HbA1C thresholds for the detection of prediabetes and diabetes in youth likely led to an underestimation of the prevalence of these conditions. Second, HbA1C was measured in a single non-fasting blood sample, with no ability to perform repeat testing in a separate blood sample or to confirm the diagnosis using a fasting glucose measurement, as recommended by the ADA diagnostic criteria. Third, because of limitations with the original HbA1C assay used, the early participants in the Black subgroup were not collected contemporaneous with the other racial/ethnic groups. However, this is unlikely to explain the marked racial differences observed, since the time span differed by only 1–4 months, and affected only the first 28% of the overall Black subset. Fourth, data on weight, height, physical activity, medications, previous diagnosis or family history of diabetes, health insurance status and measures of health-care access were not available, as the dataset comprises only that information routinely collected at the point of blood donation. Importantly, although volunteer blood donors represent a large proportion of the eligible population, this cohort is not a probability-based population sample, and therefore, our results cannot be extrapolated to the general youth population. However, due to screening criteria for donor eligibility, volunteer donors typically comprise a ‘healthy subject bias’, 6 and therefore, our results may underestimate the prevalence of abnormal HbA1C in the general youth population.
Conclusion
Abnormal HbA1C values are common in adolescent volunteer blood donors. Blood donation programmes can be used as a valuable portal for public health screening and may provide the opportunity for targeted public health interventions, triaging of donors to medical care, and research programmes for community-based participatory interventions.
Footnotes
Acknowledgements
A portion of this manuscript was previously presented as a poster on 19 March 2014 at the American Heart Association (AHA) Epidemiology and Prevention/Nutrition, Physical Activity and Metabolism (EPI/NPAM) 2014 Scientific Sessions, San Francisco, CA, USA.
Declaration of conflicting interests
Stephen J Eason and Merlyn Sayers are employed by, but have no equity interests in, Carter BloodCare. James A de Lemos is a consultant for Janssen, Amgen and Novo Nordisk. Darren K McGuire is a consultant for Janssen, Boehringer Ingelheim, Regeneron, Novo Nordisk, Sanofi Aventis and Merck and has research support from Eli Lilly, Bristol-Myers Squibb, AstraZeneca, Eisai, Boehringer Ingelheim, Lexicon, Orexigen, Janssen, Merck, GlaxoSmithKline and Takeda. All other authors report no conflicts of interest. The sponsors had no role in the design and conduct of the study; collection, management, analysis and interpretation of the data; and preparation, review or approval of the manuscript.
Funding
M Odette Gore was supported by a cardiology fellowship training grant from the National Heart, Lung, and Blood Institute of the NIH [T32HL007360]. Carter BloodCare supported all sample collection and cholesterol testing. HbA1C testing was funded by the Carter BloodCare Foundation, the Lange Endowment Disbursement Fund #2 of Communities Foundation of Texas and Coca-Cola Enterprises.