
Abstract
Objectives:
The aim of this study is to explore the contribution of genetically driven cardiometabolic risk factors for development of carotid arterial thickening in patients with type 2 diabetes.
Methods:
In total, 12 genetic risk scores for blood pressure, blood lipids and glycaemic traits were constructed. The genetic risk scores were tested for association with carotid intima-media thickness and plaques in patients with type 2 diabetes (n = 401) and in non-diabetic individuals (n = 648) and for association with glucose levels in two population-based cohorts (n = 1328 and n = 6161).
Results:
In patients with type 2 diabetes, the genetic risk scores for pulse pressure were positively associated with plaque formation (β = 0.036 ± 0.01 standard deviation/allele, p = 0.003). The genetic risk score for diastolic blood pressure was negatively associated with carotid intima-media thickness (β = –0.037 ± 0.01 standard deviation/allele, p = 0.005), although not significant after correction for multiple testing (p < 0.0042). In a meta-analysis of individuals with and without type 2 diabetes, the high-density lipoprotein genetic risk scores showed a trend towards an inverse association with carotid intima-media thickness and plaques, while the low-density lipoprotein genetic risk scores showed a trend towards a positive association with plaque formation but did reach the statistical threshold.
Conclusion:
Genetic loci for pulse pressure are associated with plaque formation among patients with type 2 diabetes, suggesting an underlying genetic contribution to arterial stiffening and atherosclerosis.
Introduction
Patients with type 2 diabetes (T2D) have increased risk of developing atherosclerosis and cardiovascular disease (CVD).1–3 Even when addressing the classical risk factors for CVD such as obesity, hyperglycaemia, hypertension, dyslipidaemia, smoking and physical inactivity; patients with diabetes still have a two- to threefold higher risk of CVD and death hereof.2–5
Subclinical atherosclerosis is a non-symptomatic abnormality that precedes atherosclerosis and CVD. In larger vessels, such as the carotid arteries, identification of subclinical atherosclerosis predicts atherosclerosis-associated CVD such as myocardial infarction and stroke. 6 Carotid intima-media thickness (IMT) is a non-invasive ultrasound measure of atherosclerosis that is used as a surrogate marker for predicting the probability of CVD in both diabetic and non-diabetic populations.7–10 Carotid IMT is a measure of the distance between the lumen-intima interface and the media-adventitia interface in the carotid arterial wall. A thickening of the intima-media distance can reflect the presence of atherosclerosis in the carotids and is a good marker of general atherosclerosis at other key arterial beds.6,11,12
Individuals with T2D have an increased carotid IMT compared with normoglycaemic individuals, and up to 73% of patients with diabetes have atherosclerosis in the extracranial carotids.13 –16 Subclinical atherosclerosis is a complex condition influenced by both genetic and environmental factors. The underlying genetic component of subclinical atherosclerosis has a heritability of 30%–65% in population-based studies and up to 92% in family studies.17–22 Only five independent loci have been identified by large genome-wide association studies (GWAS) in individuals of European ancestry to be associated with IMT or plaque in the carotids. 23 Therefore, the heritability of subclinical atherosclerosis may not only be influenced by genetic variants associated with carotid IMT but also by genetic variants associated with risk factors of atherosclerosis.
In this study, we aimed to explore the association of genetic determinants of different cardiometabolic risk factors with the development of carotid arterial thickening and plaque formation in patients with T2D. In order to test the association between the genetically driven contribution of risk factors and carotid IMT and plaque formation, we used genetic risk scores (GRSs) as an analytical tool and calculated 12 different GRSs for blood pressure, lipids and glycaemic traits. The major benefit of using GRSs is that their effects can be assumed not to be affected by confounding or reverse causation by health status in adult life.
We explored the impact of genetically driven cardiometabolic risk factors for blood pressure, blood lipids and glycaemic traits on carotid atherosclerosis and plaque formation using three different approaches. First, in order to test the genetically driven contribution of cardiometabolic risk factors to subclinical atherosclerosis in patients with T2D, we examined the association between 12 different cardiometabolic GRS with carotid IMT and plaques in a cohort of 401 individuals with T2D. Second, we tested if the genetically driven contribution of cardiometabolic risk factors to subclinical atherosclerosis was independent of diabetes status by examining the association between the cardiometabolic GRS and carotid IMT and plaques in a cohort of 638 normoglycaemic individuals. Third, in order to test if genetically driven cardiometabolic risk factors may influence glycaemic traits, we explored the association between the GRSs associated with arterial thickening with glucose levels in two population-based cohorts (n = 1329 and n = 6184) individuals at low to high risk of T2D.
Methods
Study population
CIMT trial: Data from the Copenhagen Insulin and Metformin Therapy trial (CIMT) was used for this study. 24 The CIMT trial is a multicenter, randomized, placebo controlled trial, which was conducted in the period May 2008–December 2012 in the Capital Region of Denmark, as previously described. 25 In short, the CIMT trial was conducted to evaluate the effect of treatment with metformin versus placebo in combination with insulin on carotid IMT among patients with T2D. The trial was conducted in a 2 × 3 factorial design with patients randomized to either metformin or placebo and furthermore randomized to one of the three insulin analogue regimens for 18 months. Participants were >30 years of age, with a body mass index (BMI) >25 kg/m2 and HbA1c > 7.5% (58 mmol/mol) and had been treated with oral antidiabetic treatment for at least 1 year or insulin treatment for at least 3 months prior to inclusion. Participants were excluded if they had major CVD within the last 3 months, carotid artery stenosis >70%, heart failure, recent cancer, kidney or liver disease, alcohol or drug abuse, unstable retinopathy, were pregnant or lactating, fertile women not using birth control, or if they were allergic to medication used in the trial. We used data on carotid IMT and plaque measures from the inclusion in the CIMT trial for the analyses in this study.
1936 Cohort: Data from the 1936 cohort was used as a replication cohort. The 1936 cohort consists of 1052 individuals born in 1936, used as a study cohort since 1976.26,27 In 1996, the participants were examined at an age of 60 years (n = 696). 26 The cohort was used to compare measures of carotid arterial thickening and plaque in a non-diabetic population to the diabetic population in the CIMT cohort. Participants in the 1936 cohort were excluded if they had T2D at the time of examination. Characteristics of the 1936 cohort are given in Supplementary Table 1.
ADDITION-PRO cohort: ADDITION-PRO is a cohort study of individuals at low to high risk of T2D, nested within the population-based ADDITION-Denmark. 15 The cohort was used as a control population to compare the CIMT cohort of patients with T2D to individuals without diabetes. Characteristics of the ADDITION-PRO participants included in this study are given in Supplementary Table 2. Overall, the ADDITION-PRO cohort comprises 1329 individuals − 708 with normal glucose tolerance (NGT), 254 with isolated impaired fasting glucose (IFG), 103 with isolated impaired glucose tolerance (IGT); and 116 had both IFG and IGT and 148 had screen detected T2D. All individuals who fasted <8 h before the blood samples were taken, or who used diabetes medication, or individuals with already known diabetes were excluded (n = 22).
INTER99 COHORT: Inter99 is a population-based randomized intervention study of 6784 individuals with the primary aim of preventing ischaemic heart disease by non-pharmacologic intervention. The Inter99 study has previously been described in details. 28 We included 6161 individuals with no prior history of T2D. Characteristics of the Inter99 cohort are given in Supplementary Table 2.
The CIMT protocol was approved by the Regional Committee on Biomedical Research Ethics (H-D-2007-112) and the Danish Medicines Agency, registered within ClinicalTrials.gov (NCT00657943). The 1936 cohort was approved by the Ethical Committee of the Capital Region (KA96008). The ADDITION-PRO study was approved by the Ethical Committee of the Central Denmark Region (journal no. 20080229) and the National Board of Health. The Inter99 cohort was approved by the Ethical Committee of the Capital Region (KA 98155) and registered with ClinicalTrials.gov (NCT00289237). All studies were conducted in accordance with the Declaration of Helsinki and guidelines for Good Clinical Practice. All participants provided written informed consent before participation.
Measurement of carotid IMT
CIMT cohort: Ultrasound scans of the carotid arteries were performed by two technicians using General Healthcare Logic 9 (Milwaukee, Wisconsin, USA). The ultrasonic assessment of the carotid arteries was done in two steps. First, plaques or stenoses were identified in the left and right bifurcation, common and internal carotid artery and quantified 0–5 (if there were more than five plaques, it was accounted as five). Second, carotid IMT was measured in the far wall of the common carotid artery 10 mm proximal to the bulb and averaged from the left and right side. Details on carotid IMT analysis and reproducibility have been published previously.24,28
1936 Cohort: Ultrasound scans of the carotid arteries were performed by the same technician in all patients. The examinations were performed using Vingmed CFM 800 with an annular transducer (7.5 mHz). Participants were lying on the back with their head turned 45 degrees towards left to measure carotid IMT on the right side. Carotid IMT was measured in the near and far wall of the common carotid artery and in the bulbus of the internal carotid artery. Measurements were synchronized after the R spike in the electrocardiogram. Occurrence of plaques in the carotids was visually evaluated. Plaques were defined as a thickening of the carotid IMT of at least 50%, compared to the normal IMT. Plaques occurring in all parts of the carotids were calculated and measured. Carotid IMT measurement methods have been described previously.26,29
Genotyping
Individuals of the CIMT cohort (n = 435), 1936 cohort (n = 688), ADDITION-Pro cohort (n = 1657) and Inter99 cohort (n = 6161) were genotyped by the Illumina Infinium HumanCoreExome Beadchip platform (Illumina, San Diego, CA, USA) and genotypes were called using the Genotyping module (version 1.9.4) of GenomeStudio software (version 2011.1, Illumina). In all four cohorts, we excluded individuals who had a call rate <95%, had extreme inbreeding coefficients, were ethnic outliers, or had mislabelled gender. We also checked for duplicates or first-degree relatives and excluded variants with a call rate <95%. Overall, 401 individuals of the CIMT cohort, 656 individuals of the 1936 cohort, 1342 individuals of the ADDITION-PRO cohort and 6161 individuals of the Inter99 cohort passed all quality control criteria.
All cohorts had, independently, their missing genotypes imputed on the Haplotype Reference Consortia panel (HRC version r1.1) by following the standard protocol on the Michigan Imputation Server. 30
Genetic risk scores
The GRSs were based on data from recent GWAS or meta-analyses of GWAS and calculated as: GRS for carotid IMT and for plaque, 23 GRS for fasting plasma levels of total cholesterol, high-density lipoprotein (HDL), low-density lipoprotein (LDL) and triglycerides (TG) 31 , GRS for systolic blood pressure (SBP), diastolic blood pressure (DBP) and pulse pressure (PP) 32 , GRS for fasting insulin (FI), fasting glucose (FG) and 2 h glucose (GLC) including variants identified at a genome-wide significance (p < 5 × 10−8).33,34 We calculated weighted GRSs for all abovementioned traits and tested for associations between the risk factor traits and carotid IMT and plaque formation. We constructed weighted GRSs by summing the number of effect alleles weighted by the effect sizes of the variants estimated in the GWAS studies outlined above23,31–34 and normalized with the sum of all effect sizes of the variants in the GRS. The effect alleles were defined as the alleles associated with the specified trait (for instance, triglyceride levels for the TG GRS). In total, 12 GRSs were constructed: Carotid IMT GRS, Plaque GRS, PP GRS, SBP GRS, DBP GRS, Total Cholesterol GRS, LDL GRS, HDL GRS, TG GRS, FG GRS, FI GRS and 2 h GLC GRS. A list of variants included in the GRS is included in Supplementary material.
Statistical analysis
Statistical analyses were performed using R, version 3.4.1 (http://www.r-project.org).
Measure of carotid IMT in mm and number of plaques in the carotids were used as the primary outcome in the CIMT cohort. Phenotypic traits were rank-normalized to achieve normal distributions prior to analyses.
We used additive linear regression analyses to evaluate the association between the 12 GRSs (defined above) and carotid IMT and carotid plaque. We performed linear regression analyses on the raw phenotype levels and on variables following a standard normal distribution by using a rank-based inverse normal transformation on the unadjusted variable. In all models, we adjusted for age and sex. Beta values are reported as standard deviations (SDs)/weighted allele for rank transformed variables, and as either mm/weighted allele for associations with carotid IMT or in number of plaques/weighted allele for associations with plaque formation.
For the meta-analysis, we used an inverse-variance weighted model with both a fixed and a random effect as implemented in metagen from the R-package meta (https://cran.r-project.org/web/packages/meta/meta.pdf). We reported I2 and p(Het) from test for heterogeneity between studies. Correction for multiple testing using the Bonferroni threshold yielded a significance threshold of (0.05/12) p < 0.0042, corresponding to the use of 12 different GRSs.
Results
Ultrasound measures of carotid IMT and presence of plaques were evaluated in 401 patients with T2D in the CIMT cohort. The median age was 62 years, with 33% women and 67% men included. The median carotid IMT was 0.77 mm with (1st quartile 0.68; 3rd quartile 0.88; Table 1).
Characteristics of the participants in the CIMT cohort.
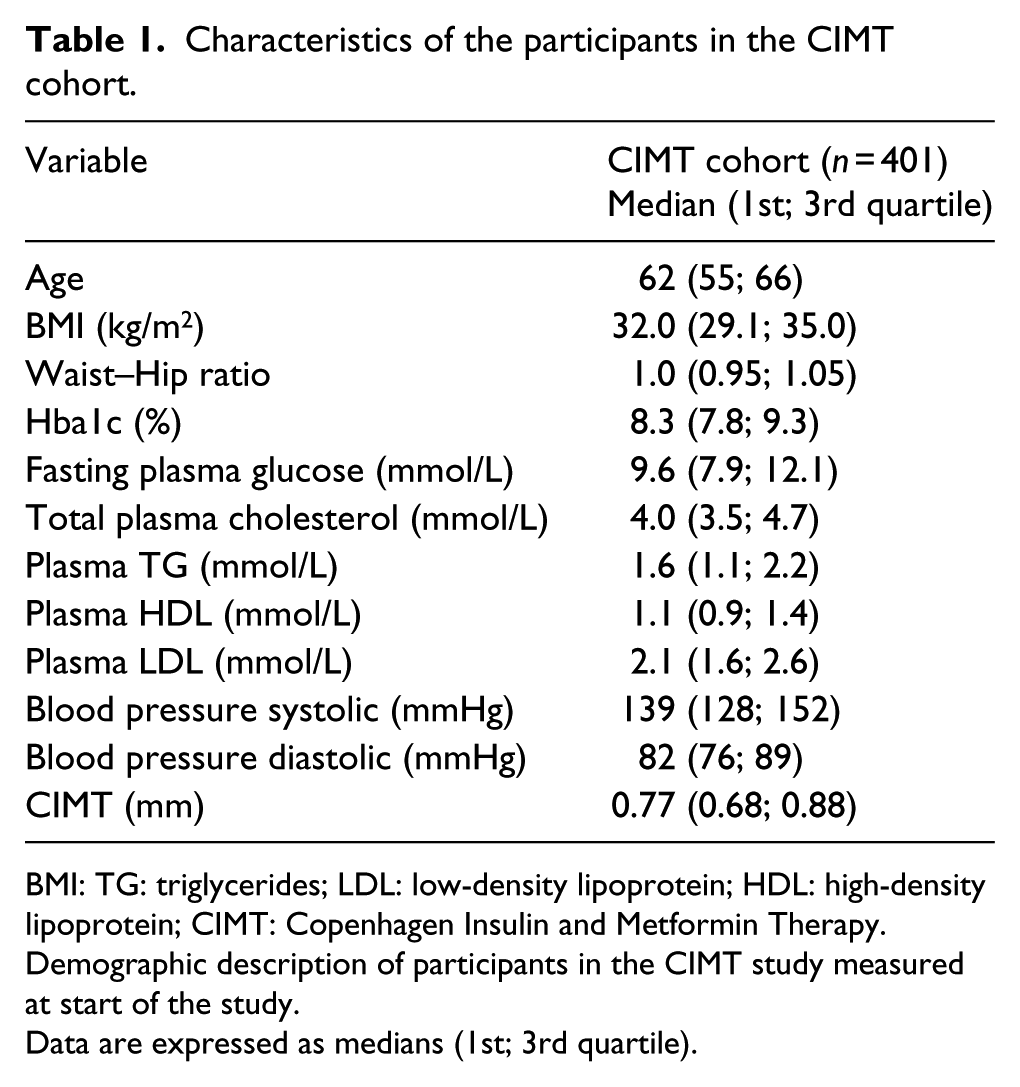
BMI: TG: triglycerides; LDL: low-density lipoprotein; HDL: high-density lipoprotein; CIMT: Copenhagen Insulin and Metformin Therapy.
Demographic description of participants in the CIMT study measured at start of the study.
Data are expressed as medians (1st; 3rd quartile).
Association of GRS with carotid IMT and plaques among patients with T2D (CIMT cohort)
First, we tested 12 GRSs for association with carotid IMT in the CIMT cohort (Table 2). The plaque GRS was associated with a higher mean carotid IMT [β = 0.126 ± 0.043 (standard error, SE) SD/allele, p = 0.003]. In contrary, the DBP GRS was associated with mean carotid IMT [β = –0.037 ± 0.013 (SE) SD/allele, p = 0.005], but after correction for multiple testing the association was no longer significant (Figure 1, Supplementary Table 3). None of the other GRSs were associated with mean carotid IMT. We found a positive association between the PP GRS and number of plaques (β = 0.036 ± 0.012SD/allele, p = 0.003) in the carotids.
GRSs of risk factors for subclinical atherosclerosis associated with mean carotid IMT.
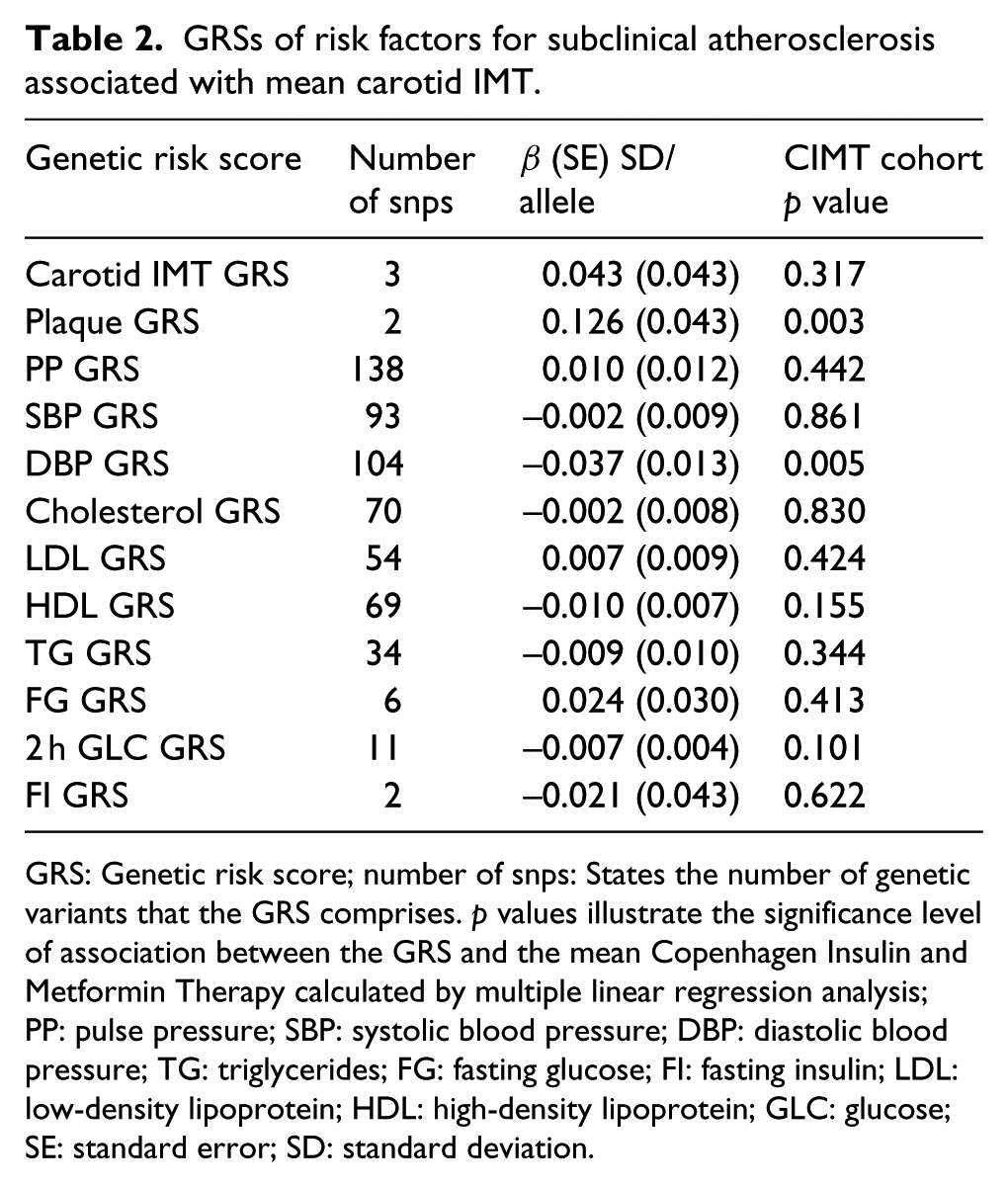
GRS: Genetic risk score; number of snps: States the number of genetic variants that the GRS comprises. p values illustrate the significance level of association between the GRS and the mean Copenhagen Insulin and Metformin Therapy calculated by multiple linear regression analysis; PP: pulse pressure; SBP: systolic blood pressure; DBP: diastolic blood pressure; TG: triglycerides; FG: fasting glucose; FI: fasting insulin; LDL: low-density lipoprotein; HDL: high-density lipoprotein; GLC: glucose; SE: standard error; SD: standard deviation.
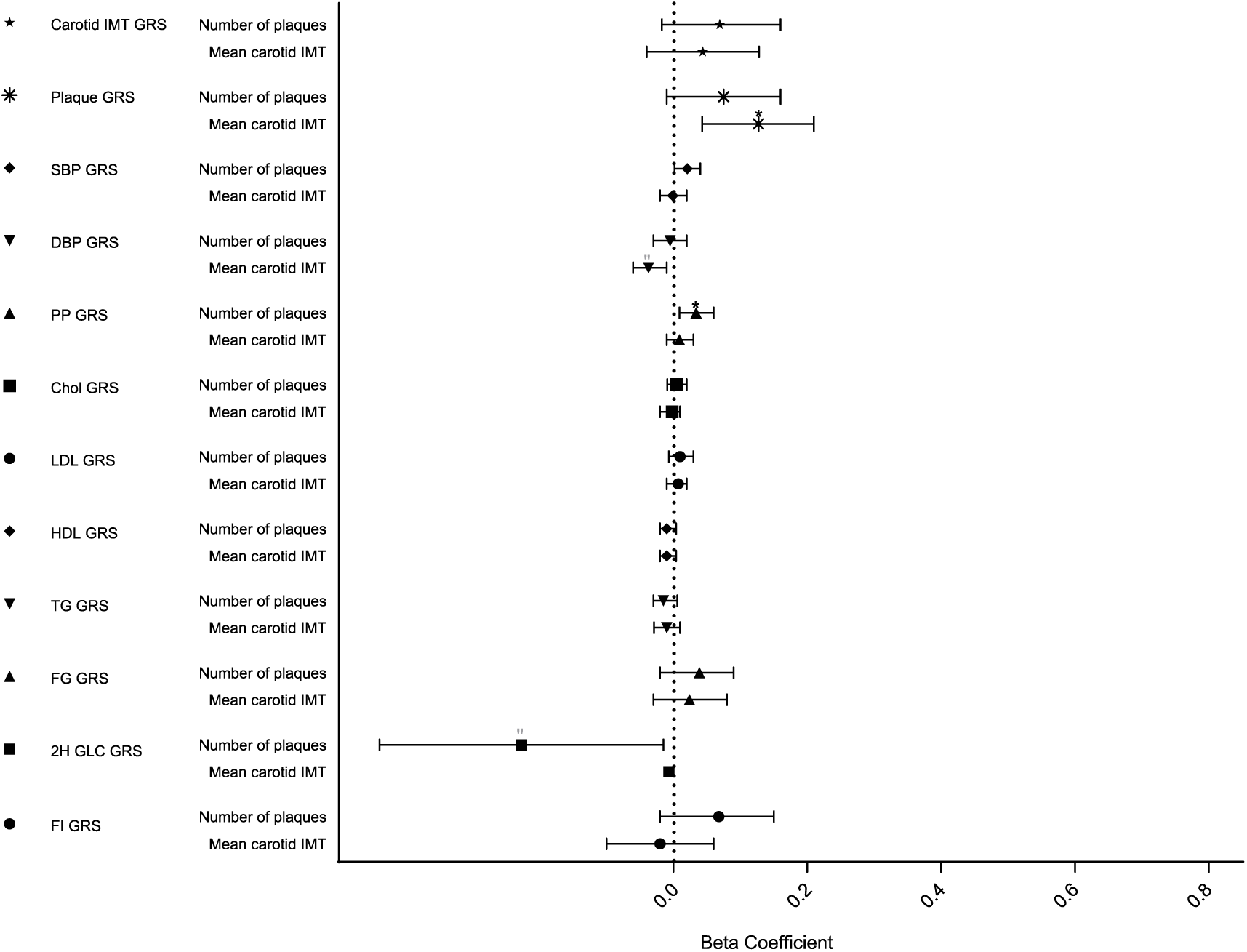
Association of genetic scores with carotid IMT variables in the CIMT cohort.
Association of GRS with carotid IMT and plaques in non-diabetic individuals (1936 cohort)
Second, we tested whether the genetically driven contribution of cardiometabolic risk factors to subclinical atherosclerosis was independent of diabetes status by examining the association between the GRS with carotid IMT and plaques in the 1936 cohort of normoglycaemic individuals. We found significant association between the carotid IMT GRS and mean carotid IMT [β = 0.117 ± 0.04 SD/allele, p = 0.004]. The SBP GRS was associated with mean carotid IMT [β = 0.019 ± 0.008 SD/allele, p = 0.029] but did not reach the Bonferroni threshold after adjustment for multiple testing (Supplementary Figure 1).
In a meta-analysis pooling the results from the CIMT cohort and the 1936 cohort, we found the same direction of effect of the HDL GRS on carotid IMT and plaque formation in individuals with and without diabetes. The association between the fixed effects of the HDL GRS and carotid IMT [β = –0.01 ± 0.01 SD/allele, p = 0.034] and with plaque formation [β = –0.01 ± 0.01 SD/allele, p = 0.036; Figure 2]. For the LDL GRS, we also found the same direction of effect on plaque formation in individuals with and without T2D. The LDL GRS showed a positive association with plaque formation [β = 0.01 ± 0.01 SD/allele, p = 0.039; Figure 2]. None of the associations in the meta-analysis remained significant after correction for multiple testing.
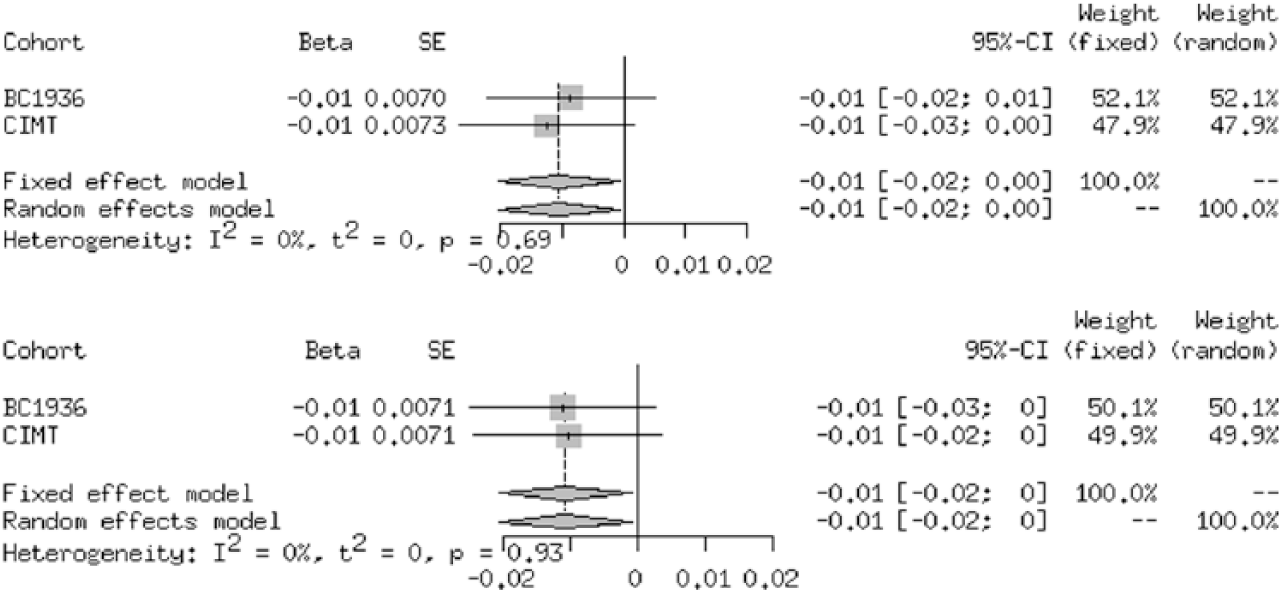
Meta-analysis of GRS and association with plaques in the carotids in the CIMT and 1936 cohort: HDL GRS and association with plaque, HDL and association with carotid IMT, LDL and association with plaque.
Association of genetic risk scores on glucose levels (ADDITION-PRO and Inter99 cohort)
In order to assess whether glucose potentially mediates the association between the HDL GRS, DBP GRS and PP GRS and arterial thickening and plaque formation in the CIMT cohort, we tested for association with glucose levels in the ADDITION-PRO cohort (n = 1329) and the Inter99 cohort (n = 6184; Supplementary Table 4). None of GRS for HDL, DBP or PP were associated with either fasting plasma glucose levels or Hba1c levels in the ADDITION-PRO cohort. There was a trend towards association between the HDL GRS and HbA1c (β = –0.005 ± 0.002, p = 0.015) and the PP GRS and fasting plasma glucose (β = 0.003 ± 0.002, p = 0.048) in the Inter99 cohort, but the findings were not significant after correction for multiple testing.
Discussion
In this study, we explored the associations between GRSs of risk factors for cardiovascular disease and carotid arterial thickening in patients with T2D. We found a positive association between the PP GRS and plaque formation, which may suggest a genetic link between arterial stiffness and carotid plaque formation. Furthermore, we found suggestive evidence of a protective effect of the DBP GRS on carotid IMT, suggesting that genetically determined higher DBP are associated with lower degrees of subclinical atherosclerosis. These findings may enable a deeper understanding of the underlying pathophysiology of atherosclerosis among patients with T2D.
Overall, the genetic contribution to elevated levels of blood pressure traits do not draw a simple picture of how genetic components of blood pressure affect carotid thickening and plaque formation among patients with T2D. However, when addressing the findings in relation to arterial stiffness, which is an independent predictor of cardiovascular disease and mortality in patients with T2D, our findings may represent novel insights into the development of cardiovascular complications among patients with T2D.35–37 In general, blood pressure traits change with age, and until middle age, any rise in SBP will lead to a parallel rise in DBP. 38 However, as the arterial compliance worsens with age and arteries become stiffer, the elasticity and capacity of the arteries to dilate during the systole diminishes. This can be seen as a decrease in DBP, an increase in SBP and subsequently a higher PP.35,38
In this study, we report that the DBP GRS may be associated with lower carotid IMT (p = 0.005), indicating that the genetic mechanisms sustaining a higher DBP may also protect from carotid IMT thickening. However, after correction for multiple testing the association was no longer significant (p < 0.0042). A higher genetically determined DBP may reflect less arterial stiffening in individuals with a high DBP GRS. These associations could suggest less vascular remodelling in individuals maintaining a high DBP, limiting the change in structural proteins from elastin to collagen in vessel walls and thereby also a smaller carotid IMT. 39 In line with these findings, we report that the PP GRS are associated with a higher number of plaques in the carotids. It is well known that a higher PP (and SBP) will lead to turbulence at the carotid bifurcation and cause a worsening of the sheer stress that leads to plaque formation. 40 The contribution of PP to cardiovascular disease among patients with T2D has previously been addressed by comprehensive arterial hemodynamics, which revealed that increased PP in T2D is caused by increased aortic stiffness and lower total arterial compliance. 41 In this study, we were unable to detect an association between measures of PP (actual levels in mmHg) and plaque formation and subsequently, testing for causality was not possible. Studies with larger samples sizes are needed to clarify, whether there is a causal relation between genetically determined PP and plaque formation.
The associations between the DBP and PP GRS with carotid IMT and plaque could not be found in the 1936 cohort of non-diabetic individuals. The reason for discrepancy between individuals with and without diabetes may be due to differences in arterial compliance. 42 When comparing the carotid IMT between the cohorts, they are almost similar in size (0.77 mm vs 0.78 mm), but it is very likely that the CIMT cohort will have worse arterial compliance due to their diabetes status, as demonstrated in previous studies.43–45 In addition, the individuals in the CIMT cohort have received statin treatment prior to the trial due to their diabetes status, which may have decreased the carotid IMT measures. 46 We pooled the results from both cohorts in a meta-analysis, which demonstrated that the HDL GRS was associated with decreased carotid IMT and plaque formation. In addition, the fixed effects in the meta-analysis showed positive associations between the LDL GRS and plaque formation. Although none of these findings remained significant after correction for multiple testing and requires replication in a larger cohort.
The strength of this study is that we used GRSs as genetic instruments, which are not affected by confounding or reverse causation by health status later in life. All participants in the CIMT cohort had a diagnosis of T2D and were receiving treatment with oral antidiabetic treatment and/or insulin, as well as lipid lowering medication (mostly statins) and antihypertensives. 25 These medications influence levels of plasma lipids and the blood pressure levels, however, have no effect on the genetic contribution to the risk factors.
There are several limitations to this study. First of all, concerning generalizability of analytical outcomes, we are using a cohort of patients with T2D, which may have higher carotid IMT and degree of subclinical atherosclerosis than the general population. In addition, they may have competing comorbidities and treatments that can influence carotid IMT and plaque formation. Still, these factors should not affect the genetic contribution to the traits and can therefore not confound the associations. The GRSs used in this study are based on a number of assumptions: an additive effect of the alleles, no gene–gene interactions and a linear relationship between the traits and carotid IMT, which may not be a correct assumption for all examined traits. However, using GRS and combining the effect of the gene variants in scores, provides a strong analytical tool to assess the overall genetic influence on carotid IMT compared to single variant association analyses. It is also important to emphasize that our findings of associations between the GRSs for risk factors and carotid arterial thickening may be influenced by pleiotropy between the traits. Since we were unable to perform mendelian randomization analyses, it is unclear whether the associations between the GRS and arterial thickening are driven by the proportion of the genetically determined increase in a given risk factor, or if the variants included in the GRS are directly affecting arterial thickening through pleiotropy. Finally, one of the limitations to this study is the sample size of the population, which may limit the power to detect true associations between GRS and subclinical atherosclerosis.
In conclusion, our results suggest that the genetic contribution to pulse pressure seems to increase the risk of plaque formation in patients with T2D. Ideally, these findings should be followed up in larger study populations to establish causal links and may enable a deeper understanding of the genetic contribution to the pathogenesis of atherosclerosis in patients with T2D.
Footnotes
Acknowledgements
H.V. and T.H. planned the study. Statistical tests were performed by L.E. and V.A. L.E., V.A., T.M.S., N.G., T.H. and H.V. analysed the results. L.E. wrote the first draft. All authors participated in revising and editing the manuscript. L.E. and E.V.A. contributed equally.
The CIMT Trial Group: Søren S Lund, Steno Diabetes Center Copenhagen and Boehringer Ingelheim International GmbH, Ingelheim, Germany, Denmark; Trine Welløv Boesgaard, Novo Nordisk, Denmark; Birger Thorsteinsson, Department of Cardiology, Nephrology and Endocrinology, Nordsjællands Hospital, Denmark and Department of Medicine, Copenhagen University, Gentofte, Denmark; Tonny Jensen, Department of Endocrinology, Rigshospitalet, University of Copenhagen, Denmark; Lise Tarnow, Steno Diabetes Center Copenhagen, Denmark; Simone B Sneppen, Department of Medicine, Copenhagen University Hospital, Gentofte, Denmark; Sten Madsbad, Department of Endocrinology, Copenhagen University Hospital, Hvidovre, Denmark, and University of Copenhagen, Denmark; Christian Gluud, Copenhagen Trial Unit, Centre for Clinical Intervention Research, Rigshospitalet, Copenhagen University Hospital, Denmark
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Søren S. Lund own shares in Novo Nordisk A/S and shares in dynamically traded investment funds, which may own stocks from pharmaceutical companies. Søren S. Lund has reported former employment at Steno Diabetes Center, which is a diabetes hospital and academic institution previously owned by Novo Nordisk. Søren S. Lund is now employed at Boehringer Ingelheim International GmbH, Ingelheim, Germany. Søren S. Lund’s contribution was his alone and does not necessarily reflect the official position of Boehringer Ingelheim.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a research grant from the Danish Diabetes Academy supported by the Novo Nordisk Foundation.
Supplemental material
Supplemental material for this article is available online.