
Abstract
Purpose:
To evaluate the association of diabetic retinopathy with subclinical atherosclerosis in middle-aged and elderly Chinese with type 2 diabetes.
Methods:
A cross-sectional community-based study was performed among 1607 patients aged 40 years or older in Shanghai. Non-mydriatic digital fundus photography examination was used in diabetic retinopathy detection. Presence of elevated carotid intima-media thickness or carotid plaque was defined as subclinical atherosclerosis.
Results:
The prevalence of diabetic retinopathy was 15.1% in total patients. Patients with diabetic retinopathy were more likely to have elevated carotid intima-media thickness, carotid plaque and subclinical atherosclerosis than those without diabetic retinopathy (37.9% vs 30.7%, 57.6% vs 49.6% and 64.6% vs 57.1%, respectively). The presence of diabetic retinopathy was significantly associated with increased odds of subclinical atherosclerosis (odds ratio = 1.93, 95% confidence interval = 1.03–3.60) after full adjustments.
Conclusion:
The presence of diabetic retinopathy was significantly associated with subclinical atherosclerosis in middle-aged and elderly patients with type 2 diabetics in China.
Background
Cardiovascular diseases (CVD) have become the main causes of mortality among patients with type 2 diabetes, which emphasizes the importance of early detection and intervention of CVD. Conventional cardiovascular risk factors including obesity, abnormal metabolism of glucose and lipids and hypertension are well known. However, those conventional risk factors only explained part of CVD risk. Therefore, detection of novel risk factors of CVD in diabetic patients is warranted.
It has been shown that alterations in the structure and function of microcirculation were associated with atherosclerosis in the heart, retina and kidney.1–3 As a specific marker of microvascular disease in type 2 diabetes, diabetic retinopathy (DR) was suggested to be associated with subclinical atherosclerosis and risk of CVD in patients with type 2 diabetes.4,5 However, other studies indicated that retinal microvascular abnormalities were not independently associated with large artery atherosclerosis after adjustments for conventional cardiovascular risk factors. 6 Furthermore, limited evidence was available regarding the association of DR with atherosclerosis in Chinese. Lian-Xi Li et al. 7 found that retinal microvascular abnormalities were independently associated with early carotid atherosclerotic lesions in hospitalized Chinese patients with type 2 diabetes. Hospitalized patients usually had a more severity of their disease, thus the association might not be generalized to general population. Currently, there is no study designed to investigate the relationship between DR and large artery atherosclerosis in community-based Chinese type 2 diabetes patients.
Therefore, using carotid intima-media thickness (CIMT) and carotid plaque as markers of atherosclerosis, we aimed to evaluate the prevalence and association of DR with subclinical atherosclerosis in a sample of middle-aged and elderly Chinese type 2 diabetic patients.
Subjects and methods
Subjects and study design
The cross-sectional study involving type 2 diabetes patients aged 40 years or older was preformed based on the diabetes health management program at Meilong Town, Minhang District, Shanghai, China, between March and September 2013. The diabetes health management program set up in 2010 is a community-based system composed of electronic health records of local diabetes patients, recruited via free health check-up annually for residents and household survey at Meilong Town. The Institutional Review Board of the Renji Hospital, Shanghai Jiao Tong University, School of Medicine, approved the study. The informed consents were obtained from all participants. The diagnosis of type 2 diabetes was defined according to the 1999 World Health Organization 8 criteria.
In brief, a total of 1950 patients aged 40 years or older involved in the program were informed to participate in the examination. Patients meeting the following criteria were excluded: (1) those with reported history of CVD (n = 189), (2) those without completed fundus photography examination (n = 152) and (3) those without ultrasound measurements of carotid (n = 2). Thus, a total of 1607 participants were eventually included in the analysis.
Questionnaire data, anthropometric and biochemical measurements
A half-day examination was performed including interview, anthropometric measurements and biochemical tests. Lifestyle information and medical histories were obtained through face-to-face interviews. The smoking and alcohol consumption habits were defined as ‘never’, ‘current’ (smoking or consuming alcohol regularly in the past 6 months) and ‘former’ (cessation of smoking or alcohol consumption more than 6 months).
Body height and body weight were measured to the nearest 0.1 cm and 0.1 kg with patients wearing light-weight clothes. Body mass index (BMI) was calculated as body weight in kilogram divided by body height squared in meters. Blood pressure was measured with an electronic sphygmomanometer (OMRON Model HEM-752 FUZZY; Omron Company, Dalian, China) two times consecutively with 1-min interval after at least 5 min rest in the seated position.
Fasting blood samples and first morning spot urine samples were obtained after at least 8-h fasting. Fasting plasma glucose (FPG), fasting serum triglycerides (TG), total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), alanine aminotransferase (ALT), aspartate aminotransferase (AST) or γ-glutamyl transferase (GGT) were determined using an autoanalyser (OLYMPUS AU640 Biochemical Autoanalyzer; OLYMPUS OPTICAL Co., Shizuoka, Japan). Haemoglobin A1c (HbA1C) was measured by high-performance liquid chromatography (MQ-2000 PT; Medconn Medical Technology Ltd, Shanghai, China). The Modification of Diet in Renal Disease formula recalibrated for Chinese was adopted to estimate glomerular filtration rate expressed in mL/min per 1.73 m2: estimated glomerular filtration rate (eGFR) = 186 × [serum creatinine (millimoles per litre) × 0.011]–1.154 × (age)–0.203 × (0.742 if female) × 1.233. 9 Urine albumin-to-creatinine ratio (UACR) was calculated by dividing the urinary albumin concentrations (OLYMPUS OPTICAL Co.) by the urinary creatinine concentrations (millimoles per litre) measured using an automatic analyzer (Beckman Coulter AU680; Beckman Coulter, Inc., Pasadena, CA, USA) and expressed in milligrams per gram.
Digital non-mydriatic fundus photography and image
Patients were leaded into a darkened room for adaptation for 5 min. A high-quality fundus photographs centred on the macula were taken on both eyes by an experienced technologist, using a Canon CR-2 camera. The photographs were stored and then graded by an experienced ophthalmologist, according to the criteria of International Clinical Diabetic Retinopathy Disease Severity Scale. 10 Grade 0: No apparent retinopathy: no abnormalities, Grade 1: Mild non-proliferative diabetic retinopathy (NPDR), Grade 2: Moderate NPDR, Grade 3: Severe NPDR and Grade 4: Proliferative diabetic retinopathy (PDR). Patients with NPDR or PDR were considered to be DR patients.
Assessment of subclinical atherosclerosis
The measurements of CIMT and carotid plaque were performed using a high-resolution B-mode tomographic ultrasound system (Voluson 730 Pro V; GE, Tiefenbach, Austria) with a linear 7.5 MHz transducer by an experienced sonographer. The measurements were carried out on the far wall of the right and left common carotid arteries, 1.5 cm proximal to the bifurcation. The transducer was manipulated so that the lumen diameter was maximized in the longitudinal plane. CIMT was measured on-line at the end of diastole as the distance from the leading edge of the first echogenic line to that of the second echogenic line. The first and second lines represent the lumen–intimal interface and the collage contained upper layer of tunic adventitia, respectively. The presence of carotid plaque was defined as a focal increase in thickness more than 0.5 mm or 50% of the surrounding CIMT value.
The greater value of the right and left common CIMT was used for analysis. The value of CIMT greater than 1.0 mm, which was the highest level of the quartiles, was defined as elevated CIMT. Presence of elevated CIMT or carotid plaque was defined as subclinical atherosclerosis. 11
Statistical analyses
Statistical analyses were carried out with SAS version 9.2 (SAS Institute, Cary, NC, USA). Continuous variables were shown as mean ± standard deviation (SD) or medians (interquartile range). TG, GGT, eGFR and UACR were logarithmically transformed before analyses due to skewed distributions. Categorized variables were presented as number (proportion).
The Student’s t-tests for continuous variables and χ2 tests for categorical variables were performed to describe and compare the baseline characteristics. Pearson’s correlations were performed to evaluate the relations of CIMT to age, male, current smoking, current drinking, use of antidiabetic drugs, use of insulin, use of antihypertensive drugs, obesity, hypertension, duration of diabetes, HbA1c, Log TG, TC, LDL-C, HDL-C, Log GGT, Log eGFR and Log UACR. Those variables were enrolled into the multivariate stepwise linear regression models to identify the factors that were independently associated with CIMT.
Multiple logistic regression analyses were used to evaluate the associations between DR and elevated CIMT, carotid plaque and subclinical atherosclerosis, respectively. In Model 1, no variables were unadjusted. In Model 2, age, sex, smoking status, drinking status, use of antidiabetic drugs, use of insulin, use of antihypertensive drugs, obesity, hypertension and duration of diabetes were further adjusted. In Model 3, TG, TC, LDL-C, HDL-C, GGT and HbA1c were further adjusted. In Model 4, eGFR and UACR were further adjusted. Two-sided p values <0.05 were considered statistically significant.
Results
General characteristics among patients with or without DR
A total of 1607 type 2 diabetic patients (718 males and 889 females) were included. The mean age of all patients was 65.0 ± 7.6 years. The prevalence of DR was 15.1% (243) in total patients, including 92 (5.7%) patients with mild NPDR, 106 (6.6%) patients with moderate NPDR, 40 (2.5%) patients with severe NPDR and 5 (0.3%) patients with PDR.
Table 1 presents the clinical characteristics of the diabetic patients with or without DR. Patients with DR had longer diabetes durations, higher levels of systolic blood pressure (SBP), FPG, HbA1c, UACR and lower levels of eGFR than those without DR (p values for all variables <0.05). Patients with DR had significantly higher levels of CIMT than those who were free of DR (0.91 ± 0.18 mm vs 0.88 ± 0.17 mm). Furthermore, patients with DR were more likely to have elevated CIMT, carotid plaque and subclinical atherosclerosis than those without DR (elevated CIMT: 37.9% vs 30.7%, carotid plaque: 57.6% vs 49.6% and subclinical atherosclerosis: 64.6% vs 57.1%; all p values < 0.05, Figure 1).
Comparison of general characteristics between subjects with or without diabetic retinopathy.
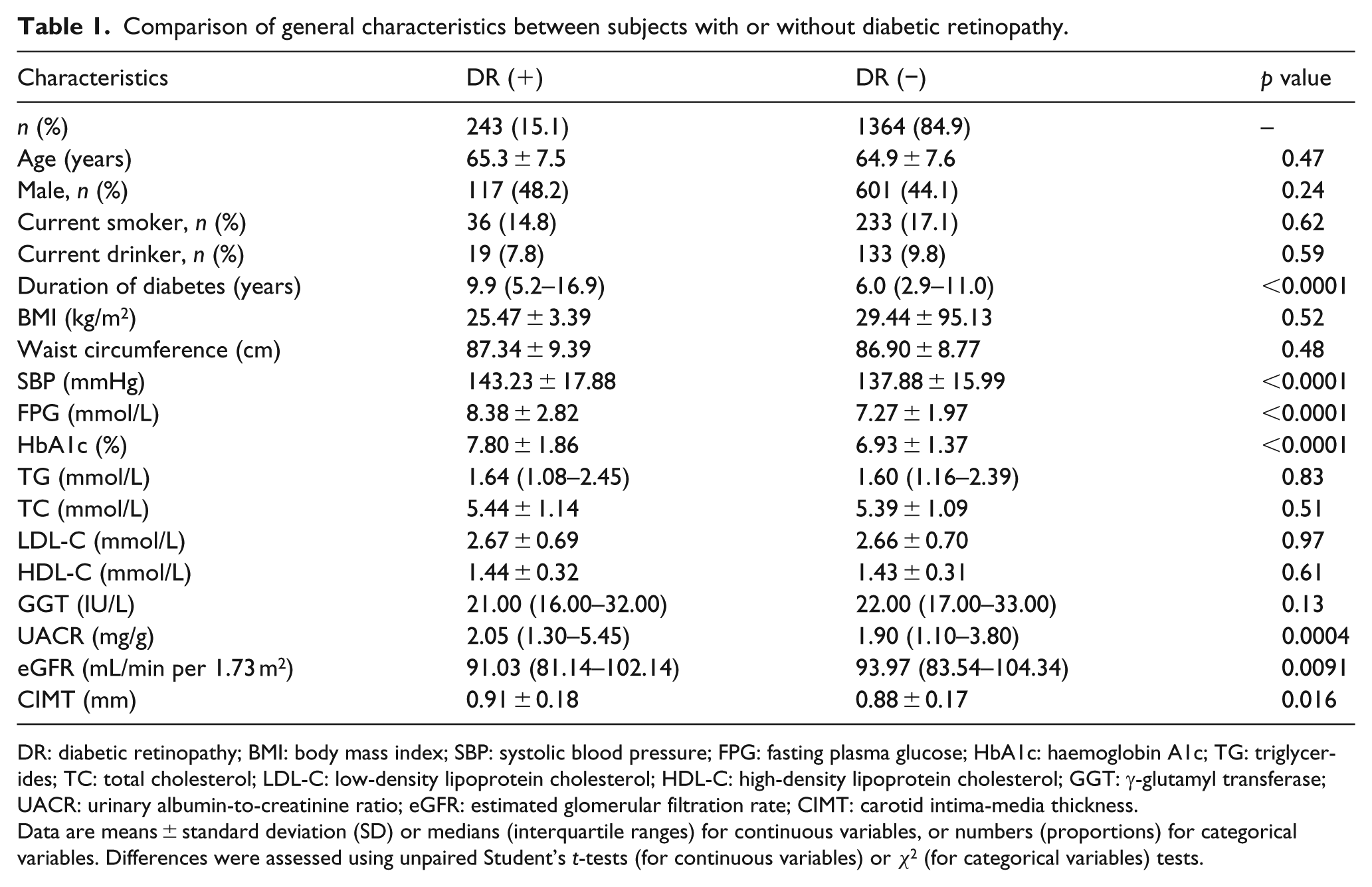
DR: diabetic retinopathy; BMI: body mass index; SBP: systolic blood pressure; FPG: fasting plasma glucose; HbA1c: haemoglobin A1c; TG: triglycerides; TC: total cholesterol; LDL-C: low-density lipoprotein cholesterol; HDL-C: high-density lipoprotein cholesterol; GGT: γ-glutamyl transferase; UACR: urinary albumin-to-creatinine ratio; eGFR: estimated glomerular filtration rate; CIMT: carotid intima-media thickness.
Data are means ± standard deviation (SD) or medians (interquartile ranges) for continuous variables, or numbers (proportions) for categorical variables. Differences were assessed using unpaired Student’s t-tests (for continuous variables) or χ2 (for categorical variables) tests.
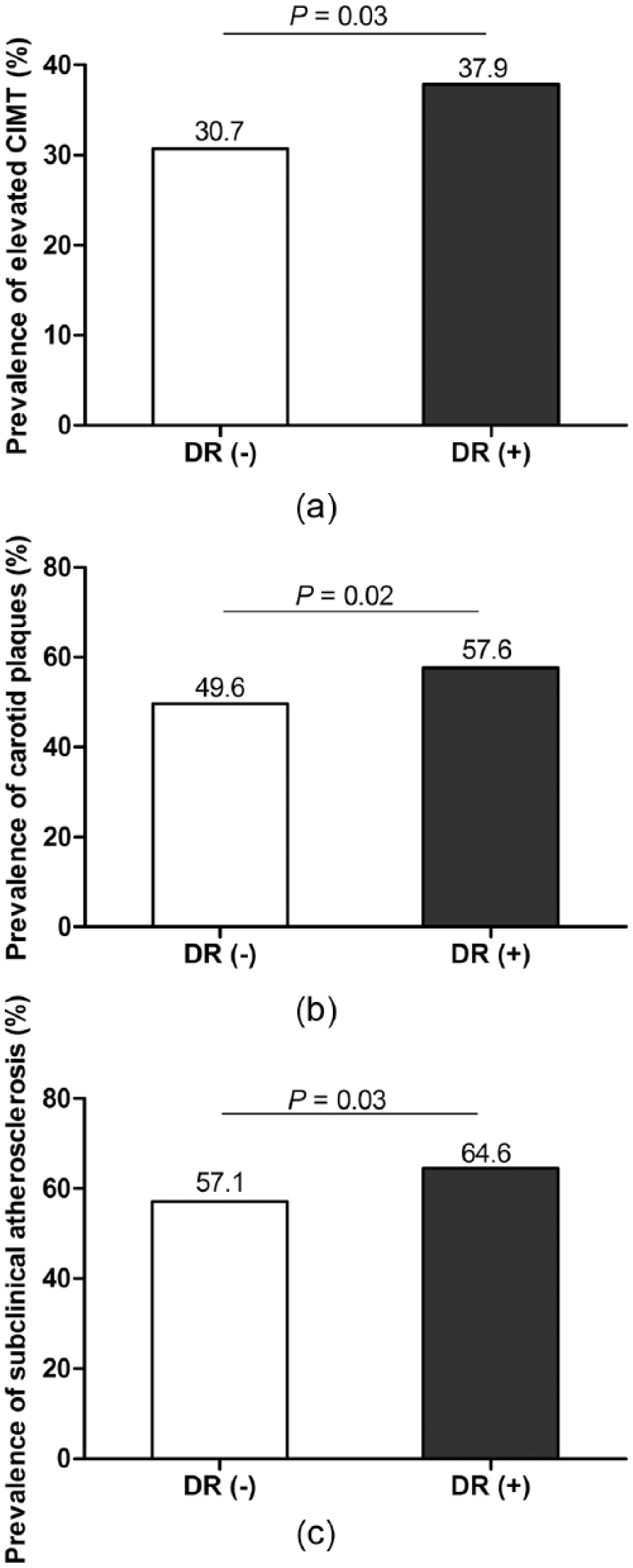
Prevalence of elevated CIMT, carotid plaques and subclinical atherosclerosis in subjects with and without DR: (a) prevalence of elevated CIMT in subjects with and without DR, bar 1: without DR (n = 92), bar 2: with DR (n = 419); (b) prevalence of carotid plaques in subjects with and without DR, bar 1: without DR (n = 140), bar 2: with DR (n = 677) and (c) prevalence of subclinical atherosclerosis in subjects with and without DR, bar 1: without DR (n = 157), bar 2: with DR (n = 779).
CIMT in relation to DR
Pearson’s correlation revealed that age, sex, current smoking, current drinking, hypertension, duration of diabetes, HbA1c, LDL-C, HDL-C, eGFR, UACR and presence of DR were significantly correlated with CIMT (Table 2). After performing multivariate stepwise linear regression analysis, we found that the presence of DR was positively and significantly correlated with CIMT, besides age, sex, current drinking and LDL-C (Table 2).
Pearson’s correlation and multiple stepwise linear regression analysis of risk factors associated with CIMT.
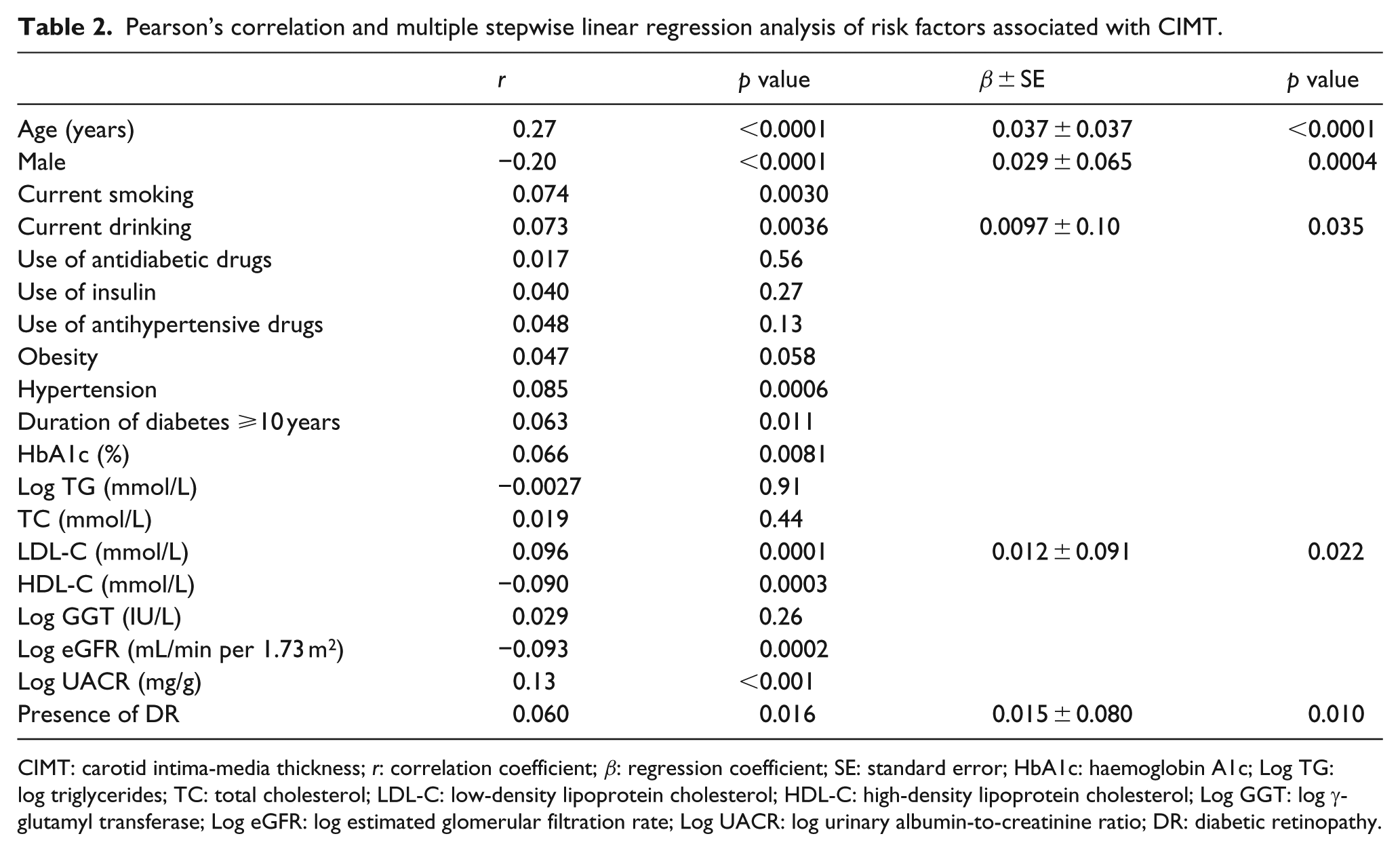
CIMT: carotid intima-media thickness; r: correlation coefficient; β: regression coefficient; SE: standard error; HbA1c: haemoglobin A1c; Log TG: log triglycerides; TC: total cholesterol; LDL-C: low-density lipoprotein cholesterol; HDL-C: high-density lipoprotein cholesterol; Log GGT: log γ-glutamyl transferase; Log eGFR: log estimated glomerular filtration rate; Log UACR: log urinary albumin-to-creatinine ratio; DR: diabetic retinopathy.
Association between DR and elevated CIMT
The presence of DR was significantly associated with increased odds of elevated CIMT (odds ratio (OR) = 1.37, 95% confidence interval (CI) = 1.04–1.83, p value = 0.028) in unadjusted model. Adjustment for age, sex, smoking status, drinking status, use of antidiabetic drugs, use of insulin, use of antihypertensive drugs, obesity, hypertension, duration of diabetes, TG, TC, LDL-C, HDL-C, GGT, HbA1c, eGFR and UACR did not materially change the association (OR = 1.84, 95% CI = 1.02–3.31, p value = 0.043) (Table 3).
Association between DR and elevated CIMT, carotid plaque and subclinical atherosclerosis.
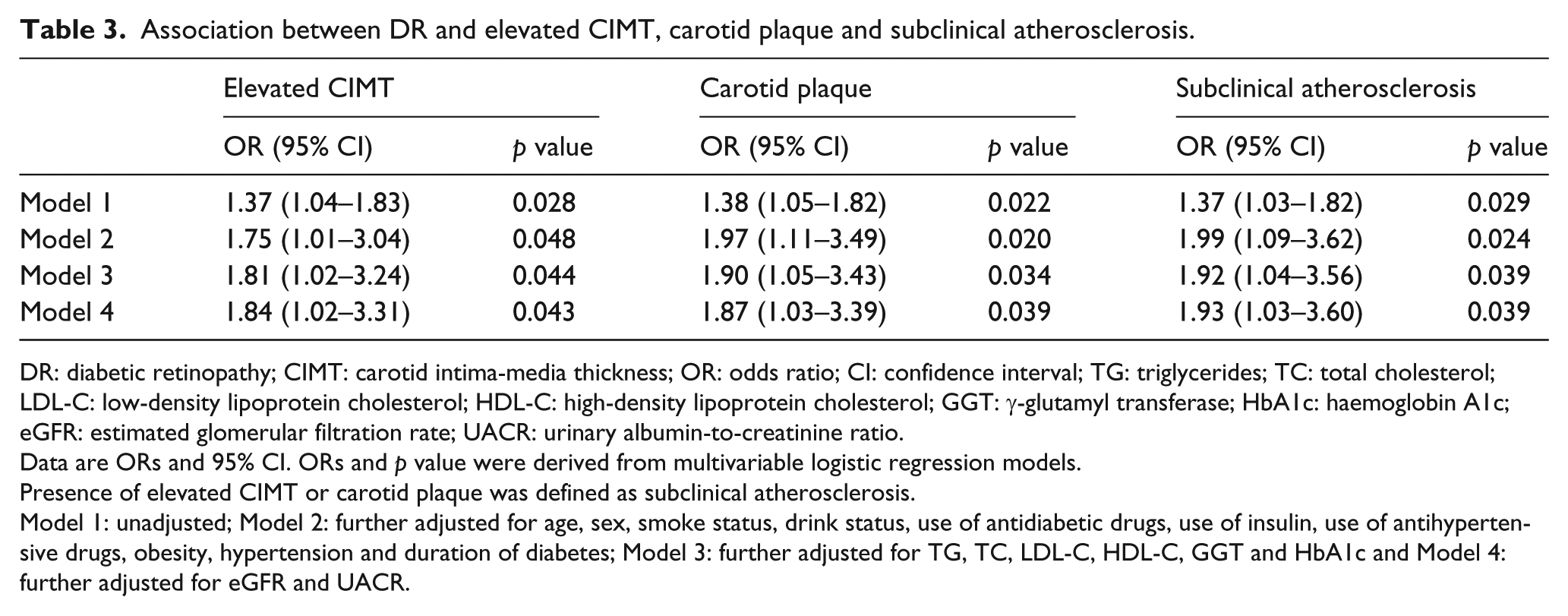
DR: diabetic retinopathy; CIMT: carotid intima-media thickness; OR: odds ratio; CI: confidence interval; TG: triglycerides; TC: total cholesterol; LDL-C: low-density lipoprotein cholesterol; HDL-C: high-density lipoprotein cholesterol; GGT: γ-glutamyl transferase; HbA1c: haemoglobin A1c; eGFR: estimated glomerular filtration rate; UACR: urinary albumin-to-creatinine ratio.
Data are ORs and 95% CI. ORs and p value were derived from multivariable logistic regression models.
Presence of elevated CIMT or carotid plaque was defined as subclinical atherosclerosis.
Model 1: unadjusted; Model 2: further adjusted for age, sex, smoke status, drink status, use of antidiabetic drugs, use of insulin, use of antihypertensive drugs, obesity, hypertension and duration of diabetes; Model 3: further adjusted for TG, TC, LDL-C, HDL-C, GGT and HbA1c and Model 4: further adjusted for eGFR and UACR.
Association between DR and carotid plaque
The presence of DR was significantly associated with increased odds of carotid plaque (OR = 1.38, 95% CI = 1.05–1.82, p value = 0.022) in unadjusted model. Adjustments for age, sex, smoking status, drinking status, use of antidiabetic drugs, use of insulin, use of antihypertensive drugs, obesity, hypertension, duration of diabetes, TG, TC, LDL-C, HDL-C, GGT, HbA1c, eGFR and UACR did not materially change the association (OR = 1.87, 95% CI = 1.03–3.39, p value = 0.039) (Table 3).
Association between DR and subclinical atherosclerosis
The presence of DR was significantly associated with increased odds of subclinical atherosclerosis (OR = 1.37, 95% CI = 1.03–1.82, p value = 0.029) in unadjusted model. Adjustments for age, sex, smoking status, drinking status, use of antidiabetic drugs, use of insulin, use of antihypertensive drugs, obesity, hypertension, duration of diabetes, TG, TC, LDL-C, HDL-C, GGT, HbA1c, eGFR and UACR did not materially change the association (OR = 1.93, 95% CI = 1.03–3.60, p value = 0.039) (Table 3).
Discussion
In this cross-sectional study, we found that in patients with type 2 diabetes free of reported CVD, the presence of DR was significantly associated with increased odds of subclinical atherosclerosis, as measured by CIMT and presence of carotid plaque. The association was independent of age, sex and other traditional cardiovascular risk factors.
Some previous studies have reported that DR was associated with non-invasive measures of subclinical atherosclerosis, such as CIMT, carotid plaque and arterial stiffness.12,13 DR was associated with CIMT in the Chennai Urban Rural Epidemiology Study (CURES-2) study. 14 Jang-Won Son et al. 12 found that DR was an independent risk marker for subclinical atherosclerosis in patients with newly diagnosed type 2 diabetes in Korea. There may be ethnic differences regarding the association of DR with atherosclerosis and there were limited data for evaluating the relationship in China. Lian-Xi Li et al. 7 found that retinal microvascular abnormalities independently associated with increased CIMT in hospitalized Chinese subjects. Consistent with the previous research, our study found that DR was associated with increased risk of prevalent subclinical atherosclerosis in general Chinese diabetic patients. And the association was not explained by a variety of cardiovascular risk factors.
The exact mechanisms linking DR to macrovascular diseases in type 2 diabetes remain to be illustrated. Several possible explanations have been proposed. First, this association may reflect the effects of atherosclerosis on the development of DR.15,16 Effects of lipids on the sclera and Bruch’s membrane lead to high choriocapillary pressure and calcification of Bruch’s membrane, as on medium and large arteries. 16 In our studies, the significant association between DR and CIMT after adjustments of lipids and other traditional cardiovascular factors indicates other underlying mechanisms involving in the association. Second, oxidative stress, inflammation and endothelial dysfunction play a significant role in the pathogenic processes of DR and subclinical atherosclerosis.17–21 However, lack of markers of oxidative stress, inflammation and endothelial dysfunction limits the analysis of these physiological changes in the association between DR and CIMT in the study.
The prevalence of DR, as one of the major causes of blindness globally, was not well evaluated in China. One previous study including 992 type 2 diabetes patients aged ⩾40 years in Shanghai reported that the prevalence of retinopathy was 10.3%. 22 However, one meta-analysis found the pooled estimate of prevalence of DR in diabetic patients was 23% (95% CI: 17.8–29.2) and found a lower prevalence (15.7%) in south China. 23 In our study, the prevalence of DR was about 15.1% in middle-aged and older community-based patients. National survey is warranted to estimate the precise prevalence of DR in Chinese diabetes patients and in different age groups for the prevention and therapy induction of DR.
The limitations of the study must be mentioned. First, this is a cross-sectional study, the association between DR and early atherosclerosis cannot be taken as a cause-and-effect relationship and further prospective survey was required. Second, because of relatively small number of patients among different classifications of DR, no significant increased risks for prevalent subclinical atherosclerosis in patients with mild, moderate and severe NPDR and PDR were found compared with those without DR. The relatively small number of patients with different grades of DR may affect the statistical power. Thus, the risk for prevalent subclinical atherosclerosis across the grades of DR warranted detailed investigation in future large-scale population study. Third, although a wide spectrum of covariates were included in the adjustment, some residual or undetected confounding factors could not be ruled out, such as markers of inflammation and endothelial dysfunction.
In summary, the presence of DR is associated with increased risk of prevalent subclinical atherosclerosis in middle-aged and elderly Chinese type 2 diabetic patients. Future well-designed prospective studies should include longitudinal measures of metabolic factors related to microvascular disorders to elucidate the prospective relationship between DR and CVD.
Footnotes
Declaration of conflicting interests
The authors declared that no competing interests exist.
Funding
This study was supported by grants from the National Natural Science Foundation of China (No. 81270875).