
Abstract
Background:
Type 1 diabetes is associated with increased risk of cardiovascular disease and the diabetic complication cardiovascular autonomic neuropathy in itself entails increased cardiovascular risk by mechanisms not yet fully understood. Arterial calcification is an important predictor of cardiovascular events; the aim of this study was to investigate the level of generalised arterial calcification in patients with long-term, normoalbuminuric type 1 diabetes and the association with cardiovascular autonomic neuropathy, as these factors have not been investigated in type 1 diabetes.
Methods:
Participants were examined for calcification of coronary and carotid arteries through non-contrast multi-detector computed tomography scans. Generalised arterial calcification was defined as the presence of calcium in both the coronary and carotid arteries.
Results:
A total of 53 patients with type 1 diabetes were included. Coronary and carotid artery calcium scores were correlated (r = 0.720, p < 0.0001). Cardiovascular autonomic neuropathy was associated with increased coronary (p = 0.002) and carotid (p = 0.001) artery calcium scores. Seventeen of 20 patients with cardiovascular autonomic neuropathy (85%) demonstrated generalised arterial calcification compared to 11 (33%) patients without cardiovascular autonomic neuropathy; patients with cardiovascular autonomic neuropathy had an odds ratio of 11.3 (95% confidence interval = 2.7–47.1, p < 0.001) for generalised arterial calcification.
Conclusion:
Cardiovascular autonomic neuropathy is associated with increased level of generalised arterial calcification in patients with normoalbuminuric, long-term type 1 diabetes.
Keywords
Introduction
Patients with type 1 diabetes have increased risk of cardiovascular (CV) disease and mortality compared to persons without diabetes. Cardiovascular autonomic neuropathy (CAN) is a severe complication to diabetes and increases the risk of CV disease in itself and aggravates risk of CV events if present alongside other complications such as nephropathy.1,2 CAN is due to damage to the autonomic nerve fibres innervating the heart and blood vessels and is associated with increased coronary artery calcification (CAC) in patients with type 1 diabetes.3,4 The advanced atherosclerotic lesions contain calcium, which can easily and non-invasively be quantified using non-contrast multi-detector computed tomography (MDCT) scans. Quantification of CAC, CAC score, is shown to be a strong predictor of future CV events. 5
Arterial calcification is not always isolated to the coronary arteries, suggesting arterial calcification may be a generalised process. Indeed, correlations of calcifications of varying strengths have been shown between the coronary, carotid, aortic arch, distal aorta and iliac arteries in asymptomatic persons. 6 CAC has also been shown to be associated with carotid stenosis and stroke and associations exist between carotid artery calcium, stenosis and cerebrovascular events. Knowledge of vascular calcification beyond the central, coronary arteries improved prediction of CV outcomes beyond traditional CAC score and classical CV risk factors in persons with type 2 diabetes. 7
To our knowledge, generalised arterial calcification has not been examined in patients with type 1 diabetes. In asymptomatic persons, it was previously demonstrated that the presence of calcium in both the coronary and carotid arteries meant calcification of other arteries; 6 this lead us to investigate the coronary (central) and carotid (peripheral) arteries as a measure of generalised calcification.
The objectives of this study were to investigate generalised arterial calcification in patients with normoalbuminuric, long-term type 1 diabetes with and without CAN and to investigate if CAN increased the level of generalised arterial calcification in these patients.
Methods
The primary outcome in this study was generalised arterial calcification, which was defined as the presence of calcium in both the coronary and carotid arteries.
This study was a cross-sectional study of previously examined normoalbuminuric patients with long-term type 1 diabetes without known CV disease, who were tested for CAN and its association with different CV implications. 4 The participants were recruited at the Diabetes Unit, Rigshospitalet, Copenhagen University Hospital and Steno Diabetes Center, Gentofte. As previously reported, inclusion criteria were type 1 diabetes >10 years, age 18–75 years and HbA1c < 86 mmol/mol (10%) and exclusion criteria were albuminuria (defined as urinary albumin: creatinine ratio > 30 mg/g), elevated S-creatinine > 120 μmol/L, untreated hypertension > 140/85 mmHg and clinical symptoms or electrocardiographic signs of cardiac disease. 4 Participants were examined with MDCT from March 2012 until October 2012.
The study was conducted according to Declaration of Helsinki II as well as approved by the Danish Scientific Ethical Committee and all participants gave oral and written informed consent.
MDCT scan
Participants were examined with a 320-detector CT scanner (Aquillon One, Toshiba Medical Systems, Japan) using electrocardiogram-gated scanning and data were analysed with dedicated software (Vitrea, Vital Images Inc., USA). Non-contrast coronary and carotid images were acquired for arterial calcium scoring and reconstructed with 3 mm slice thickness.
Arterial calcification
CAC score was assessed according to the Agatston method, where calcium deposits in the coronary arteries were identified as a dense area of >130 Hounsfield Units (HU) in the arterial wall. 8
Carotid artery calcium scoring was calculated as dense areas in the carotid wall at the carotid bifurcations ±20 mm 9 (corresponding to 6–7 MDCT slices of 3 mm) >130 HU, adapted from the Agatston method. The presence of calcification was defined as an Agatston score >0.
CAN testing
As previously described in detail, 4 CAN was defined as abnormal results of two or more out of four tests, as proposed by The Toronto Consensus Panel on Diabetic Neuropathy adapted from the original tests proposed by Ewing et al.: (1) heart rate variability (HRV) during deep breathing was abnormal if ⩽10 beats per minute, (2) Valsalva ratio was abnormal if ⩽1.10, (3) lying-to-standing heart rate test was abnormal if ⩽1 and (4) blood pressure in response to standing was abnormal if ⩾30 mmHg.
Statistical analysis
Analyses were carried out using SPSS 22 (IBM SPSS Statistics, New York, NY, USA). Results were considered significant if p < 0.05. Dichotomous variables are presented as number of observations (percentages) and group differences were examined with either chi-square test or Fisher exact test. Continuous variables are presented as medians [(interquartile range (IQR))] when data are skewed or as means ± standard deviation (SD) when data follow normal distribution; group differences were examined with Mann–Whitney U test for skewed data and Student’s t-test for normally distributed data. Correlation of coronary and carotid calcium scores was examined using Spearman’s rho. Odds ratios for generalised calcification were calculated from the chi-square test using the risk function in SPSS 22. A sensitivity analysis was carried out in order to analyse whether the results from the overall population differed when the two CAN-groups were demographically comparable.
Results
A total of 53 patients with type 1 diabetes, 33 without CAN and 20 with CAN, underwent non-contrast MDCT scan of coronary and carotid arteries (Table 1).
Demographic and arterial calcification data in normoalbuminuric patients with type 1 diabetes with and without cardiovascular autonomic neuropathy.
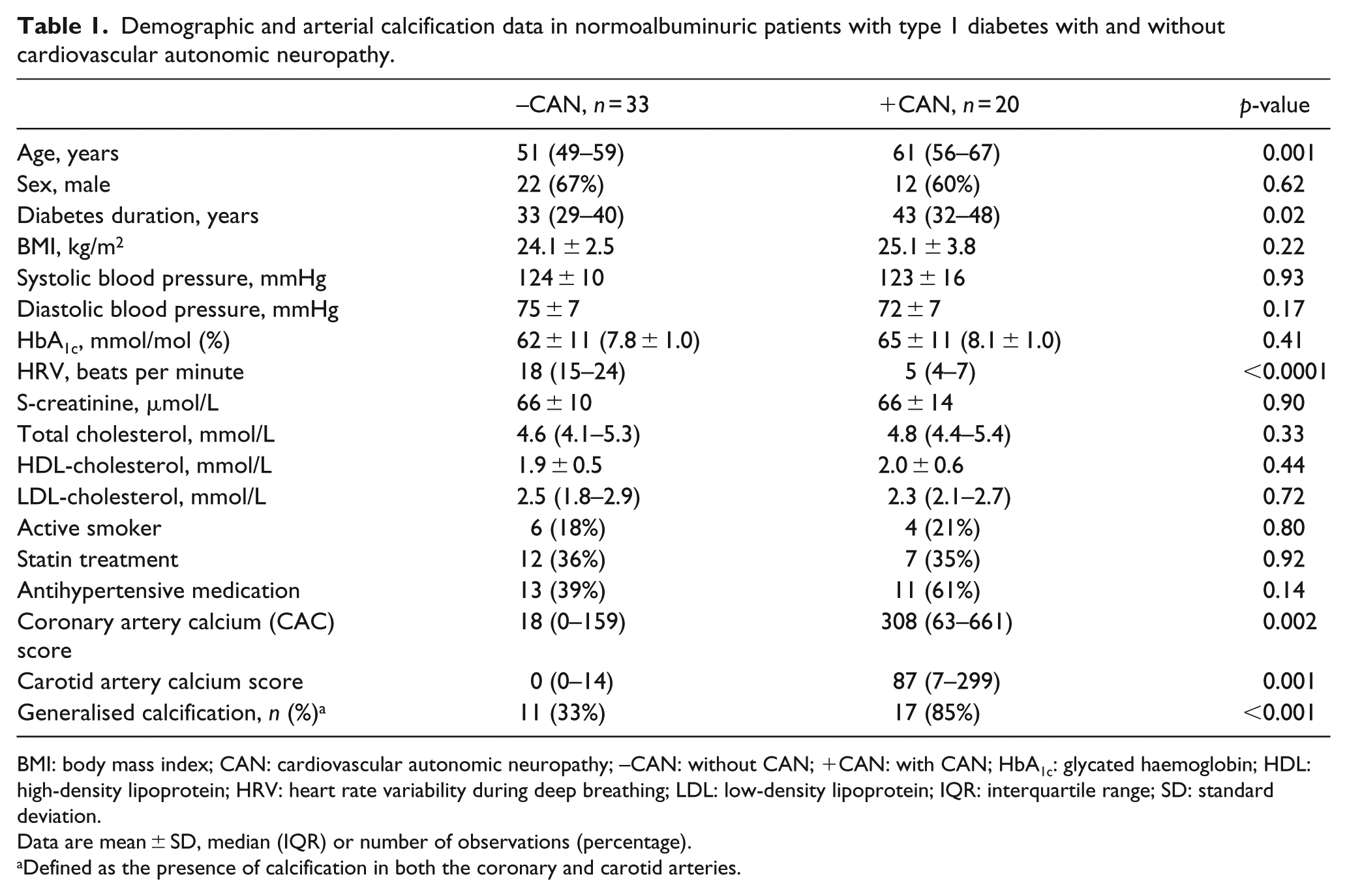
BMI: body mass index; CAN: cardiovascular autonomic neuropathy; –CAN: without CAN; +CAN: with CAN; HbA1c: glycated haemoglobin; HDL: high-density lipoprotein; HRV: heart rate variability during deep breathing; LDL: low-density lipoprotein; IQR: interquartile range; SD: standard deviation.
Data are mean ± SD, median (IQR) or number of observations (percentage).
Defined as the presence of calcification in both the coronary and carotid arteries.
There was a significant correlation between the coronary and carotid artery calcium scores (r = 0.720, p < 0.0001) in the overall population. Generalised arterial calcification (of both the coronary and carotid arteries) was found in 28 (53%) patients with long-term, normoalbuminuric type 1 diabetes. Figure 1 illustrates distribution of arterial calcifications according to CAN status: most of the patients (85%) with CAN had presence of calcium in both carotid and coronary arteries, whereas this was only found in 33% without CAN. Patients with CAN had an odds ratio of 11.3 [(95% confidence interval (CI) 2.7–47.1, p < 0.001)] for generalised calcification compared to patients without CAN.
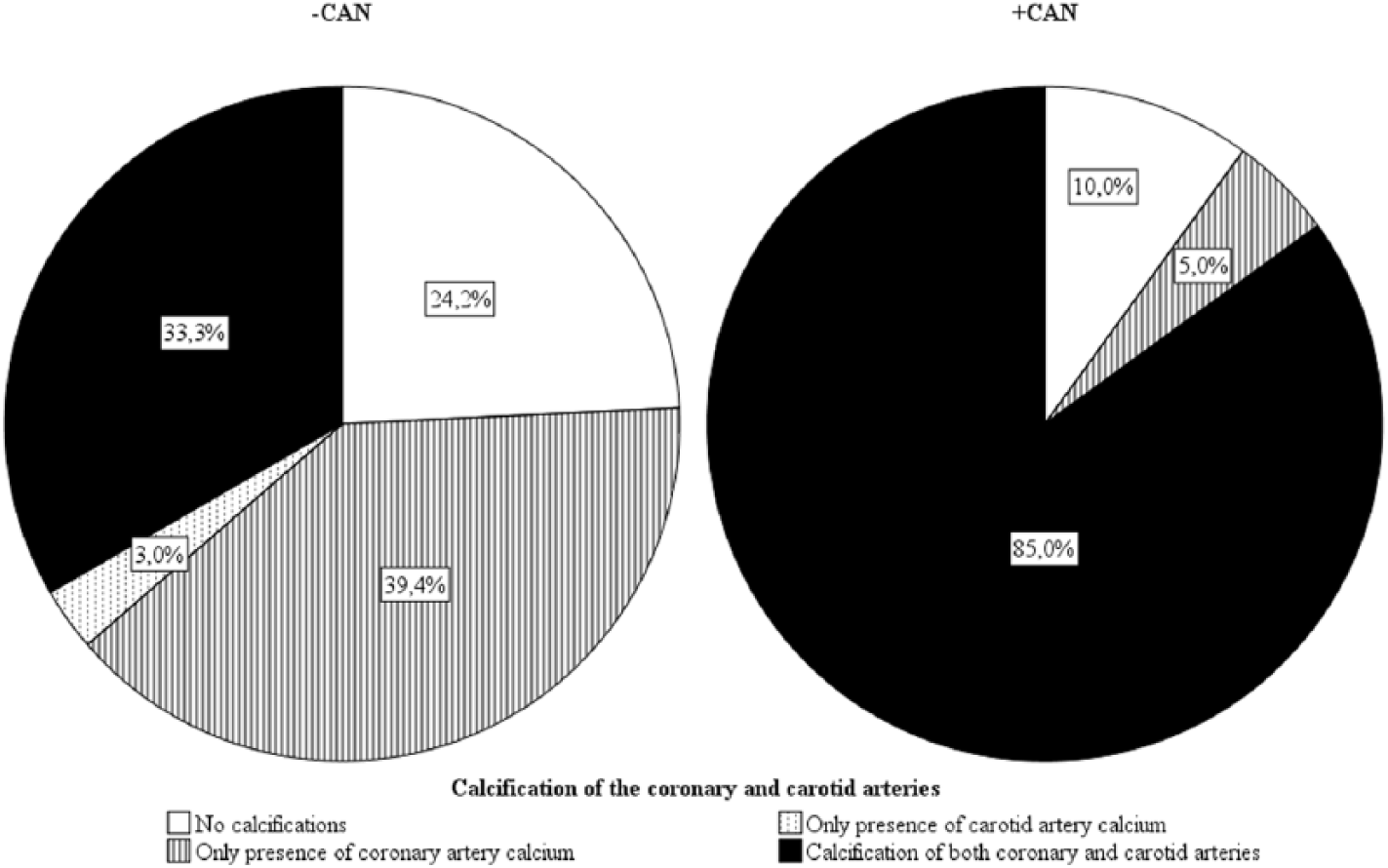
Overview of calcification of coronary and carotid arteries in long-term, normoalbuminuric patients with type 1 diabetes with and without cardiovascular autonomic neuropathy.
Sensitivity analysis
To account for the demographic differences (Table 1), sensitivity analyses were performed by excluding the 13 youngest patients without CAN. This rendered 20 patients with CAN and 20 patients without CAN with no significant demographic differences (data beyond age, sex, duration of diabetes and HbA1c are not shown): the above-mentioned results regarding arterial calcifications remained unaltered. The results are displayed in Table 2. The odds ratio for generalised calcification in patients with CAN in the sensitivity analysis was lower although still significant with a value of 6.9 (95% CI = 1.5–31.2, p = 0.008).
Results from the sensitivity analyses of arterial calcification without demographic differences in normoalbuminuric patients with long-term type 1 diabetes with and without cardiovascular autonomic neuropathy.
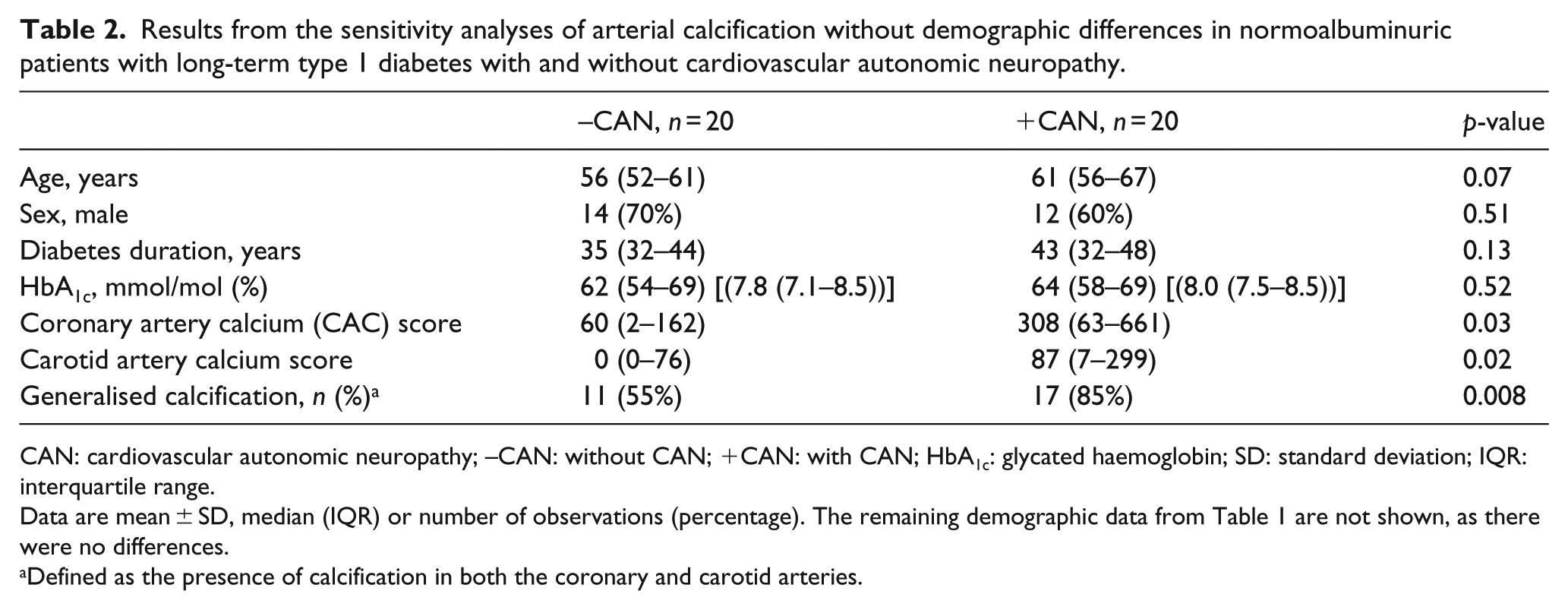
CAN: cardiovascular autonomic neuropathy; –CAN: without CAN; +CAN: with CAN; HbA1c: glycated haemoglobin; SD: standard deviation; IQR: interquartile range.
Data are mean ± SD, median (IQR) or number of observations (percentage). The remaining demographic data from Table 1 are not shown, as there were no differences.
Defined as the presence of calcification in both the coronary and carotid arteries.
Discussion
The main finding of this study is that the majority (85%) of the patients with CAN had generalised calcification in both coronary and carotid arteries, contrary to one-third of patients without CAN (Figure 1). A study by Allison et al. 6 found that classical risk factors for CV disease such as age and hypertension were risk factors related to diffuse arterial calcium deposits. The data presented in this study suggest that CAN may also be an important risk marker for generalised arterial calcification in patients with type 1 diabetes. It may be speculated that increased arterial calcification in patients with CAN is, at least partly, a result of the autonomic denervation in CAN, 4 as surgical sympathectomy leads to arterial calcification. As CAN is associated with increased risk of generalised arterial calcification, this could explain some of the increased CV risk in patients with type 1 diabetes complicated by CAN.
It is not possible to directly compare our results with other studies of generalised calcification in patients with type 1 diabetes, as no studies have investigated multiple vessel beds for calcifications at the same time. One previous study by Costacou et al. 10 found calcification of the peripheral arteries in the lower extremities (in particular in the ankle and foot) to be associated with the presence of CAC 6 years later, although this finding was solely significant until adjustment for autonomic neuropathy.
Limitations
As this is a cross-sectional analysis, it is not possible to determine a causal relationship between CAN and generalised calcification, but the presented results suggest a strong association between these factors. Demographic differences in factors such as age and duration of diabetes between the CAN groups may be important confounders; however, these were accounted for in the sensitivity analyses, where the calcification results persisted. Furthermore, the presented data set is rather small and the findings should be confirmed in larger studies, where it will also be statistically possible to generate larger multivariable models to account for more confounders.
Conclusions
In conclusion, the majority of patients with CAN showed generalised calcification of the investigated arteries (coronary and carotid arteries) as opposed to patients without CAN. It remains to be determined whether these vascular calcifications are indeed associated with cardio- and cerebrovascular events in these patients with type 1 diabetes. The presented findings may explain some of the increased CV risk in patients with CAN and type 1 diabetes.
Key messages
Cardiovascular autonomic neuropathy (CAN) aggravates the risk of cardiovascular (CV) disease in patients with type 1 diabetes.
Arterial calcification can easily be measured with non-contrast computed tomography scans.
85% of the patients with long-term, normoalbuminuric type 1 diabetes and CAN had generalised arterial calcification.
Patients with type 1 diabetes and CAN had increased level and odds ratio for generalised arterial calcification compared to patients with type 1 diabetes without CAN.
Generalised arterial calcification may be a novel CV risk marker and improve risk stratification in patients with type 1 diabetes.
Footnotes
Acknowledgements
H.Ø.H., T.J., J.H., U.M.M. and K.F.K. made substantial contributions to the conception and design of the work as well as acquisition, analysis and interpretation of data. P.R. and L.K. made substantial contributions to the conception of the work and acquisition of data for the work. H.Ø.H., T.J., J.H. and K.F.K. drafted the work. U.M.M., P.R. and L.K. revised it critically for important intellectual content. All authors approved the final version to be published. H.Ø.H. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. The data have not been presented previously. The data are confidential and, as such, are not accessible.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article: We report no conflicts of interests. Outside the presented work, P.R. reports stock ownership or options: Novo Nordisk A/S; research funding: Abbvie and Novo Nordisk; honoraria to institution for consulting and lectures: Astra Zeneca, BMS, Boehringer Ingelheim, Eli Lilly, Novo Nordisk, Sanofi Aventis, Astellas and Abbvie.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from Arvid Nilssons Foundation and A.P. Moeller Foundation.